Article Text

Abstract
Aim: To determine prevalence, demography, mechanism, and visual morbidity of glaucoma in urban Thai people.
Methods: 790 subjects aged 50 years or older from Rom Klao district, Bangkok, Thailand, were enumerated in a population based cross sectional study. Each subject underwent the following investigations: visual acuity, visual field testing, slit lamp examination, applanation tonometry, gonioscopy, and an optic disc examination after mydriasis. Main outcome measures included visual acuity (logMAR), visual fields, intraocular pressure (IOP), gonioscopic characteristics, vertical cup/disc ratio (VCDR), prevalence of types of glaucoma. Glaucoma was diagnosed on the basis of optic disc appearance and visual field defects. In eyes in which the optic disc could not be examined, glaucoma was diagnosed when visual acuity was <3/60 and either IOP >99.5th percentile or there was evidence of previous glaucoma surgery.
Results: 701 subjects were examined (response rate 88.7%). In eyes with “normal” suprathreshold visual fields, the mean IOP was 13.3 mm Hg (97.5th percentile = 20 mm Hg). The 97.5th and 99.5th percentiles of VCDR were 0.72 and 0.86 respectively. Of the 701 subjects examined in the clinic, 27 had glaucoma (3.8%, 95% CI: 2.5 to 5.6), 16 had primary open angle glaucoma (POAG, prevalence 2.3%, 95% CI: 1.3 to 3.7), six were primary angle closure glaucoma (PACG, prevalence 0.9%, 95% CI: 0.3 to 1.9), and five were secondary glaucoma (SecG, prevalence 0.7%, 95% CI: 0.2 to 1.7). Among the 43 unilaterally blind subjects, glaucoma was the cause in five subjects (12%). One subject was bilaterally blind due to glaucoma (prevalence 11%, 95% CI: 0.3 to 61.9). 28 people (4%) were glaucoma suspects on the basis of optic disc appearance and six on the basis of visual fields only. 98 subjects (14%) had “occludable angles” in either eye, 22 of whom had primary angle closure (PAC, prevalence 3.1%, 95% CI: 1.9 to 4.7); 14 had peripheral anterior synechiae in either eye and eight had ocular hypertension (OHT).
Conclusions: POAG accounted for 67% of all glaucoma, PACG 21%, and secondary glaucomas 12%. Glaucoma was the second most common cause of severe unilateral visual loss.
- glaucoma
- Thailand
Statistics from Altmetric.com
The prevalence and characteristics of glaucoma in the people of South East Asia are not well documented. A recent population based study of Singapore Chinese1 showed primary open angle glaucoma (POAG) to be the predominant form (49%) in this population, with primary angle closure glaucoma (PACG) accounting for 31% and secondary glaucoma 16%, of all glaucoma. A prospective, islandwide incidence study2 confirmed the supposition that Chinese ethnicity carried a significantly higher risk of symptomatic primary angle closure (PAC) compared with non-Chinese Singaporeans (relative risk 2.8). There were insufficient numbers to calculate incidence figures for Malay and Indian people in Singapore. Hospital discharge data have helped determine the magnitude of PACG morbidity in the two smaller ethnic groups of Singapore; the discharge rate (per 100 000 per year) for PACG among Malay people was 6.0 and 6.3 for Indians. The rate among Chinese was 12.2.3 These figures probably represent the rate of symptomatic disease, as most non-acute care is provided on an outpatient basis. The rate of symptomatic PAC among Thai people was reported to be 7.0/100 000/year.4 The concordance between these figures for Thai and Malay people is striking.
The aim of this study was to determine the prevalence, associated visual morbidity, and ocular features associated with the glaucoma, in an urban population in Thailand.
METHODS
Sampling strategy
Rom Klao is a suburban area of Lat Krabang district situated about 35 kilometres south east of the central business district of Bangkok. In 1997, the Department of Geriatric Medicine, Chulalongkorn University Hospital, Bangkok, conducted a census of all households in Rom Klao in order to select a cohort of subjects aged 50 years or older for a study of medical problems, their risk factors, and determinants of health among this age group. In order to qualify for selection, one or more of the individuals in a household had to own the home and individuals selected had to have no intention of moving from the area within 3 years, to allow further longitudinal studies to take place. 941 people were identified from a total population of 15 003. During the 2 years that elapsed before the glaucoma survey, 68 subjects emigrated, 64 subjects died, and a further eight subjects refused to continue to participate. 57 of these 140 subjects were men and 83 women (mean age 66.8 (SD 10.5) years). The remaining cohort of 801 people were contacted in late 1999 in order to conduct the glaucoma survey.
Examination
Approval for the study was obtained from the institutional review board at Chulalongkorn University Hospital, Bangkok. Informed consent was obtained from each subject.
Presenting visual acuity (with spectacles if worn) was measured in each eye separately at 4 metres using the reduced logMAR tumbling E chart,5 which was initially validated against an ETDRS chart (Lighthouse).6 If the subject was unable to correctly identify the orientation of one or more of the Es on the top line, they were moved to 1 metre, and the acuity tested again.
A 22 point single stimulus suprathreshold visual field test was performed on both eyes of all subjects (Henson CFA 3200, Clement Clark, Harlow, Essex, UK). If one or more points were missed, the test was automatically extended to 66 points. If the machine registered a “suspect” or “definite” defect, the subject repeated the suprathreshold test after resting for at least 30 minutes.
If, after repeated suprathreshold visual field testing, a reproducible (see “diagnostic definitions”) visual field defect was identified for which no cause could be found on ocular examination, a threshold visual field test was performed. This was performed the following day; similarly, if any of the following optic disc features were identified, regardless of the suprathreshold field test result: CDR of 0.70 or more; focal notching of the neuroretinal rim (rim width reduced to 0.1 CDR or less (between 11 to 1 o’clock or 5 to 7 o’clock)); CDR asymmetry of 0.20 or more; disc margin haemorrhage. These values for CDR and asymmetry of CDR were chosen with reference to data from Singaporean Chinese people.1
Anterior chamber examination with the slit lamp (BM model, Haag-Streit, Bern, Switzerland) was specifically directed at detection of signs of pigment dispersion syndrome, angle closure, pseudoexfoliation, and other secondary causes of glaucoma. Signs of previous surgery were also noted.
Intraocular pressure (IOP) was measured by Goldmann applanation tonometry (calibrated daily) (Haag Streit, Bern, Switzerland), with the median of three consecutive readings taken as the IOP for each eye.
Gonioscopy was performed on all subjects (Goldmann model, Haag Streit, Bern, Switzerland). The angle was described as “occludable” if less than 90° of the posterior (usually pigmented) trabecular meshwork could be seen without manipulation or indentation. In cases where the ciliary body band could not be seen, dynamic, four mirror gonioscopy was performed (Carl Zeiss, Oberkochen, Germany), to establish whether peripheral anterior synechiae were present. Pupils were pharmacologically dilated using tropicamide (1%; Alcon-Couvreux SA, Puurs, Belgium) and phenylephrine (2.5%; Moorfields Eye Hospital, London, UK) in all subjects. Subjects were warned of the symptoms of angle closure and asked to return should these be experienced. Each was given a tablet of acetazolamide (250 mg; Wyeth Laboratories, Maidenhead, UK) after dilatation and a further tablet to be taken several hours later. No subjects experienced an acute episode of angle closure following dilatation.
The optic disc was examined using a contact lens at ×16 magnification. A measuring eyepiece graticule (Haag-Streit, Bern, Switzerland) was used to measure the vertical optic disc diameter and vertical cup diameter. The posterior pole was examined for pathology.
Diagnostic definitions
Visual fields
If two suprathreshold fields were performed on an eye, a defect was judged reproducible if 50% or more points missed on the first test were subsequently missed on the second.
Threshold visual fields were judged acceptable for analysis if there were 50% or fewer false positives (false negatives and fixation losses were ignored). After excluding the superior four points and the four points immediately adjacent to the blind spot, a defect was considered present if it was 18° × 12° or larger in size and 10 dB or more below the age specific threshold normal.
Optic disc parameters
The distribution of vertical cup/disc ratio (VCDR) of the non-glaucomatous population was calculated from data from subjects with a “normal” result on suprathreshold field screening in both eyes. If the VCDR of one or both discs, or disc asymmetry was less than the 97.5th percentile of this distribution, the discs were considered “normal.”
Definition of glaucoma
Cases of glaucoma were defined using the International Society of Geographical and Epidemiological Ophthalmology (ISGEO) scheme.7 The scheme classifies cases of glaucoma according to three levels of evidence or “categories” (Table 1). The highest level of certainty (category 1) requires optic disc abnormalities (VCDR ⩾97.5th percentile in the population with “normal” suprathreshold visual fields) and visual field defect compatible with glaucoma. In the second (category 2), if a visual field test could not be performed satisfactorily, a severely damaged optic disc (VCDR ⩾99.5th percentile of the population with “normal” suprathreshold visual fields) would be sufficient to make the diagnosis. Lastly, (category 3), if the optic disc could not be examined because of media opacity (and, hence, no field test was also possible), an IOP exceeding the 99.5th percentile (of the population with “normal” suprathreshold visual fields), or evidence of previous glaucoma filtering surgery, was taken as sufficient for a diagnosis of glaucoma.
Classification of glaucoma7
Glaucoma suspects were divided into six groups:
(1) Disc suspects—those who met category 1 disc criteria, but were not proved to have definite field defects.
(2) Field suspects—those with definite field defects, but not meeting category 1 disc criteria
(3) Those with optic disc margin haemorrhages
(4) Those with an IOP ⩾97.5th percentile. These subjects had open angles, non-glaucomatous visual fields, and “normal” optic discs.
(5) Those with an occludable drainage angle but “normal” optic discs, visual fields, and an IOP <97.5th percentile.
Cases of primary angle closure (PAC) were defined by the presence in either eye of an occludable angle with an IOP equal to or greater than the 97.5th percentile and/or peripheral anterior synechiae.
Definition of blindness
An eye was considered blind if the visual acuity (using available refractive correction) was worse than logMAR 1.3 (<3/60 Snellen).
Follow up care of established glaucoma cases
Subjects in whom ocular pathology was detected were referred to either the local district hospital or to Chulalongkorn University Hospital for further management.
Statistics and data analysis
Age and sex specific prevalences of glaucomas and their 95% confidence intervals (using the Poisson distribution) were calculated.8 Population prevalence figures were calculated by direct standardisation to the 1999 urban population of Thailand.9
RESULTS
Demographics
Among the 801 subjects identified, five had died, five had moved away from the district, and one was hospitalised. Therefore 790 were considered eligible for the study; 701 subjects were examined in the clinic. Of the 89 people not seen in the clinic, 27 (30.3%) were immobile because of ill health and 62 refused offers of examination. The response rate was therefore 88.7% (701/790). Table 2 summarises the demographics of the 790 subjects who were considered eligible for the study. The 140 subjects (mean age 66.8 years (SD 10.47)) who were lost from the cohort between 1997 and 1999 were older than the 701 subjects (mean age, 63.3 (7.4) years) examined; however, there was no significant difference in sex between the two groups. Among the non-responders at the time of the survey, there were more men than women. However, among those examined, there were more women than men. This difference in sex between those examined and the non-responders was significant (Pearson’s χ2 p <0.001).
Demographics of the study sample
Distribution of CDR and IOP
Of those subjects where the CDR could be measured (669 subjects), the mean CDR (right eyes) was 0.44 (SD 0.19; 95th, 97.5th, 99.5th percentiles: 0.72, 0.83, 0.95). The mean CDR asymmetry (left minus right VCDR) was 0.001 (p >0.5).
There were 498 subjects with normal suprathreshold visual fields. The median VCDR in this group (right and left eyes) was 0.45 with 97.5th and 99.5th percentiles of 0.72 and 0.86, respectively. The mean CDR asymmetry (left minus right VCDR) was 0.002 (p >0.5).
Table 3 gives the VCDR data that was used to categorise the subjects into glaucoma cases, glaucoma suspects and normals.
The distribution of cup/disc ratio in those subjects with normal suprathreshold visual fields in both eyes
Of those subjects in whom the intraocular pressure was measured (696 subjects), the mean IOP (right eyes) was 13.4 mm Hg (SD 3.9; 95th, 97.5th, 99.5th percentiles: 19.0 mm Hg, 21.0 mm Hg, 37.6 mm Hg).
The mean and median IOP in those with “normal” suprathreshold visual fields in both eyes (1018 eyes) was 13.3 mm Hg (SD 3.2). The 97.5th and 99.5th percentiles were 20 mm Hg and 22 mm Hg respectively. The distribution of IOP in this population is illustrated in Figure 1.

The “normal” distribution of intraocular pressure (in subjects with normal suprathreshold visual fields in both eyes; right and left eyes included).
Glaucoma cases
In all, 27 subjects were classified as glaucoma cases, 16 of whom had POAG (59%), six had PACG (22%), and five (18%) had secondary glaucoma (SecG; four traumatic, one phacomorphic). The demographics of glaucoma cases and age and sex specific prevalences of glaucoma are given in Tables 4 and 5, respectively. Of the POAG cases, 13 were in “category 1” (optic disc abnormalities and visual field defect compatible with glaucoma), three in “category 2” (severe optic disc damage; visual field not possible), and 0 in “category 3” (disc examination and visual field impossible; IOP >99.5th percentile or evidence of previous glaucoma filtering surgery). For PACG cases, these numbers were 14, 2, and 0, respectively, and with SecG, 4, 1, and 0, respectively.
The demographics of the glaucoma cases
Prevalence of glaucoma by age and sex
The absolute numbers of male and female cases would suggest a preponderance of glaucoma among women. However, following age standardisation, no significant sex difference existed when considering all cases of glaucoma (χ2 test, p=0.295), or PACG (p=0.085), or secondary glaucomas (p=0.289) individually. However, POAG was significantly more prevalent in women (p=0.006) than men.
Five (31%) of the POAG cases had an IOP in either eye which was equal to or greater than the 97.5th percentile of the population with “normal” suprathreshold visual fields. Three (50%) of the PACG cases and four (80%) of the secondary glaucoma cases had an IOP equal to or greater than the 97.5th percentile in either eye.
The prevalence of all glaucoma cases combined was significantly higher in subjects aged 70 years and older compared with those aged 60–69 years (OR: 2.74 (1.10 to 6.88); p=0.015)) and 50–59 years (OR: 5.50 (1.60 to 20.7); p=0.001)).
Primary angle closure
Twenty two subjects were diagnosed with PAC (prevalence 3.1%, 95% CI: 1.9 to 4.7); 14 had PAS in at least one eye; eight different subjects had an IOP of >97.5th percentile. Only one had PAS and a raised IOP.
Glaucoma suspects
Glaucoma suspects were divided into five groups according to the definitions above. The findings are tabulated in Table 6. Two subjects had ocular pathology associated with secondary glaucoma. One diabetic subject had an occludable angle, and another subject had pseudoexfoliation syndrome and ocular hypertension.
The glaucoma suspects: demographics
Prevalence of blindness
A total of 54 subjects were unilaterally blind on presentation (age and sex standardised prevalence of 7.5% (95% CI 7.4 to 7.5)) and 43 subjects after refractive correction (prevalence of 6.0 (95% CI 5.9 to 6.0)). Fourteen (age and sex standardised prevalence of 1.8% (95% CI 1.8 to 1.8)) were bilaterally blind on presentation and nine remained blind even after refractive correction (age and sex standardised prevalence of 1.21% (95% CI 1.19 to 1.22)).
The causes of blindness are given in Table 7. Cataract was the leading cause of unilateral and bilateral blindness (best corrected) in 23 (53%) and five (55.5%) subjects, respectively. Glaucoma was the second most common cause of unilateral blindness (five subjects, 12%). Trauma resulted in secondary glaucoma in three cases (7%) of unilateral blindness.
Prevalence of blindness
DISCUSSION
Glaucoma was the second most common cause of unilateral blindness (12%) after cataract. This result is similar to that of a survey of hospital records in Thailand in 197310 where glaucoma was found to account for 11.2% of 18 170 cases of blindness.
The mean and median intraocular pressure in this study was 13.3 mm Hg. This is broadly consistent with mean IOP in other population based studies in the region that have used Goldmann tonometry such as 13.4 mm Hg in China11 and 12.7 mm Hg in Mongolia.12 These values are much lower than those reported in white populations.13,14
The distribution of cup-disc ratio is also not dissimilar to that found in the Chinese population of Singapore1 (median VCDR of all eyes 0.47; 97.5th and 99.5th percentiles, 0.71 and 0.81, respectively). In both studies, the same technique of disc assessment was used and the “normal” distribution was derived from those subjects with normal suprathreshold visual fields. Of interest is the similarity of the 97.5th percentile cut off for cup-disc ratio found in this study to that of white population based studies with subjects over the age of 50 years, such as the Netherlands15 (mydriatic ophthalmoscopy without graticule, 97.5th percentile, 0.7).
This definition of an “occludable angle” was arbitrary and was adopted for the sake of consistency with several large population based glaucoma surveys.1,12,16,17
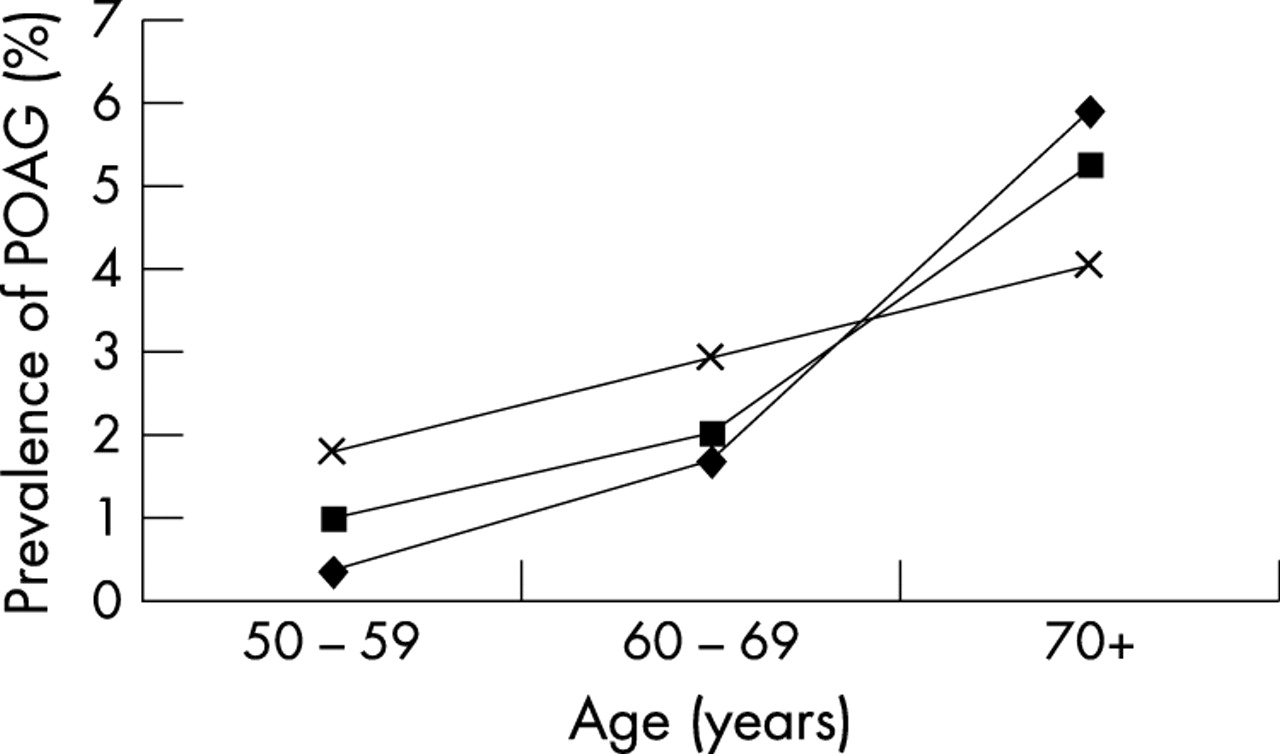
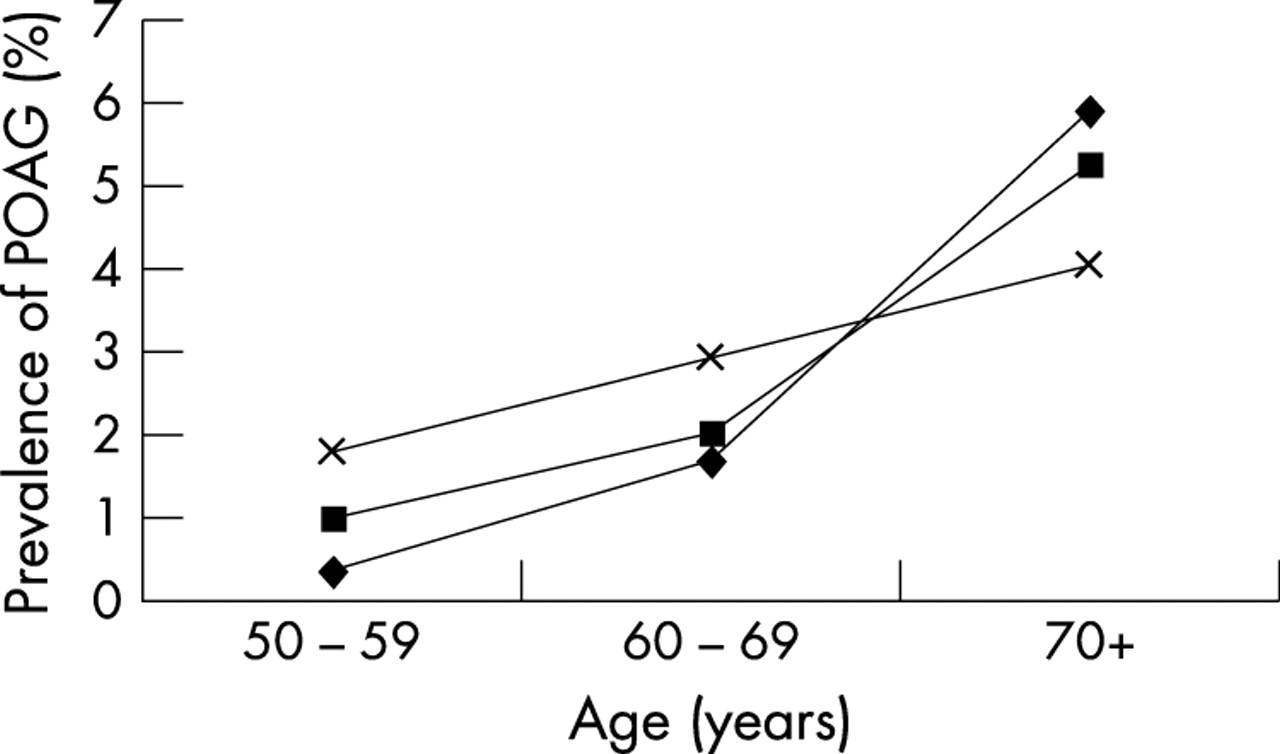
The prevalence of glaucoma increased with age in both sexes. In the 50–59 year age group, the prevalence of glaucoma in males was 2.6%, and 1.2% in females. These proportions were increased in those aged 70 years or more, to 6.8% and 10.1%, respectively. In 1996, Quigley18 published a statistical model of glaucoma prevalence worldwide derived from available published data. These data suggested a linear relation between open angle glaucoma and age in Asians. Both the current study and a recent study of Chinese Singaporeans1 suggest a non-linear increase in POAG with age (Fig 2). This should be interpreted with caution in view of the relatively small numbers of cases in the current study and hence relatively wide confidence intervals. It appears that the pooled data model of POAG prevalence proposed by Quigley18 overestimates the rate in those under the age of 70 and underestimates in those over this age.
The finding in this study, that 50% of PACG cases had been previously diagnosed by a hospital or clinic, in comparison with 25% of the POAG cases (Table 4) is interesting. Although this is not a statistically significant (χ2, p=0.27) difference, involving small numbers of cases, this may suggest that PACG is more likely to be symptomatic than POAG, resulting in the subject seeking medical advice. More PACG subjects (33%) were blind in one or both eyes than POAG (25%; χ2, p = 0.69), so it could be surmised that reduced vision is the main symptom why more PACG subjects present. We did not inquire about other symptoms such as pain; however, other studies in east Asia have found that the painful acute PACG is much less common than the painless chronic PACG.12 No ischaemic sequelae, such as iris whorlling, were observed in any of the PACG cases suggesting that these cases were chronic in nature. Although all subjects with secondary glaucomas in this study were blind in one eye, only 20% had sought a medical opinion, which suggests that there may exist other barriers to the uptake of medical care.
The relative proportions of glaucoma attributable to POAG, PACG, and secondary glaucoma found in this Thai study are presented in Figure 3 alongside data obtained from other studies (some requiring more detailed data from personal communication with Dandona and Foster).1,12,19,20 These studies have used similar diagnostic criteria and were compared by direct standardisation to the population of Thailand.9 The populations of Singapore and Thailand are intermediate between the extremes of Mongolia,12 where there is relatively more PACG, and Ireland,20 where there is relatively more POAG. Dandona et al17 classified ocular hypertensives with occludable angles as cases of PACG. This would have increased the number of PACG cases, when comparing with the other studies illustrated. The ratio of POAG: PACG in Singapore Chinese (1.6:1) compared to that of Thais (3.2:1) and Indians (2.4:1), reflects the findings of a glaucoma incidence study in Singapore,2 where Malays and Indians were found to be at lower risk of symptomatic PAC in comparison with the Chinese population. It also reflects the findings of a study in Thailand4 where the incidence of PACG was much lower than in Singaporean Chinese.
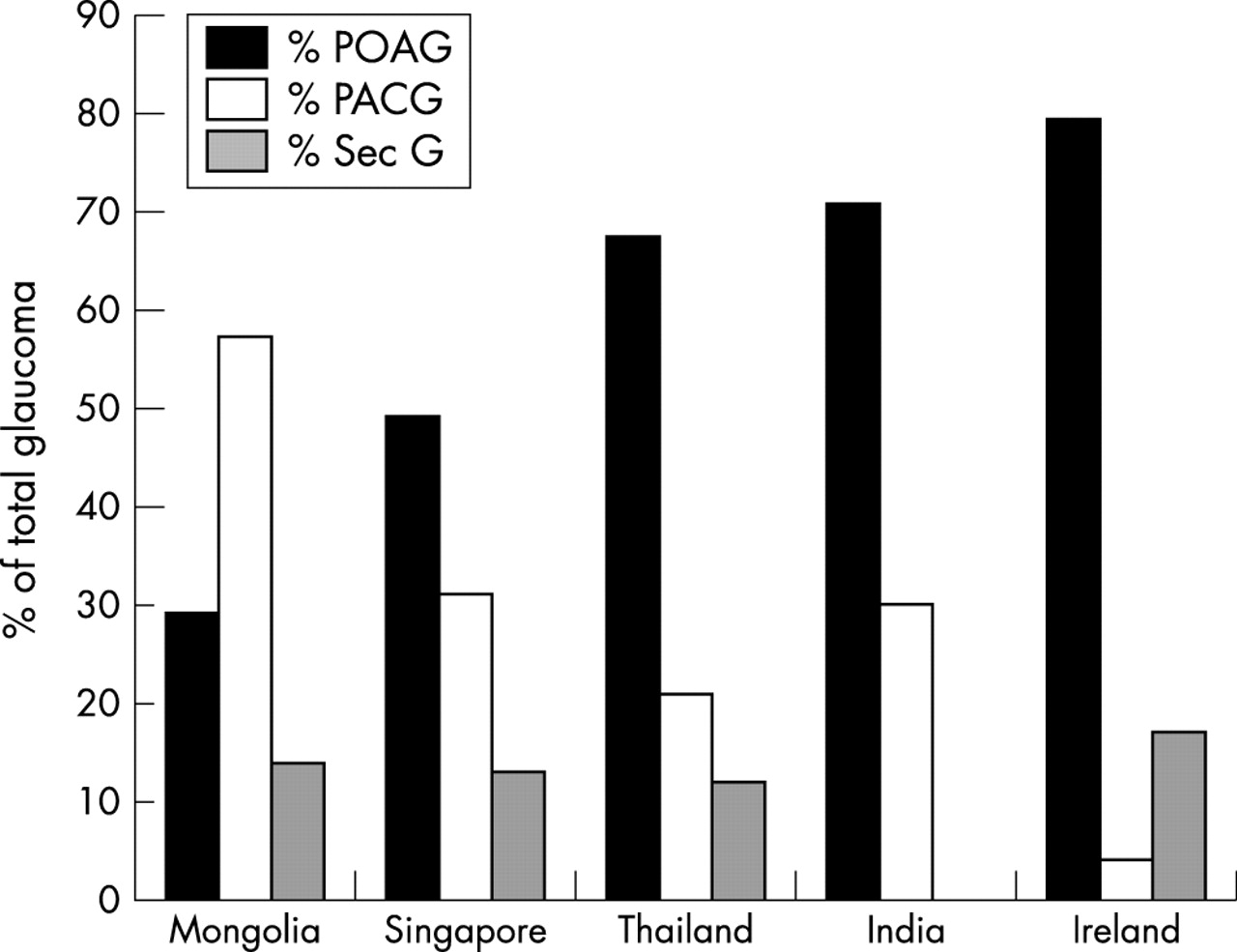
The relative proportion of primary glaucoma attributable to POAG, PACG, and SecG found in Mongolia and Singapore (unpublished data from Foster PJ, 2000), Thailand (current study), India (unpublished data from Dandona L, 2000) and Ireland.20 All data are directly standardised to the urban population of Thailand.9
With the population expansion of those aged 50 or more that is expected in Thailand in coming years, one can project that the prevalence of glaucoma will also substantially increase. Applying the findings of this survey to such a population projection9 (Fig 4), the number of males affected by glaucoma is expected to rise threefold, and for females fourfold, over the next 50 years. The findings of this survey and these future projections emphasise the importance of glaucoma as a cause of visual impairment in Thailand and throughout South East Asia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The projected number of people in Thailand affected by glaucoma from year 2000 until year 2050 (demographic data obtained from age and sex specific country population data9). Figures given were calculated using age and sex specific glaucoma prevalence figures for all glaucomas from Table 5 (squares, men; diamonds, women).
Acknowledgments
The authors wish to thank Ms Benjamas Prapamont, Ms Nattinee Riandara, Ms Siriwan Chatapatama, Ms Wanna Kittiyapison, and Miss Ranee Taveekiteekul who recruited subjects and assisted with the study. Dr Wongwat Luiwlak, the director of the Community Health Centre in Rom Klao gave logistic support. Dr Brendan Dineen assisted with the statistical analysis. The Division of Geriatric Medicine, Department of Medicine, Faculty of Medicine, Chulalongkorn University received funding from the Thai government for the project “Cohort study of problems, their risk factors and determinants of good health among the elderly living in Rom Klao community, Bangkok” (CERB project).
REFERENCES
Footnotes
-
Presented in part at The Association for Research in Vision and Ophthalmology, Fort Lauderdale, Florida, May 2001.
-
Funded by the British Council for the Prevention of Blindness, London, UK, and the Glaucoma Research Fund, Department of Ophthalmology, Chulalongkorn University, Bangkok, Thailand. The authors have no financial interests related to this manuscript.
Series editors: W V Good, S Ruit