Article Text

Abstract
Objective: To examine the evidence for an association between cognitive impairment or dementia and the presence of retinal microvascular abnormalities.
Methods: A systematic review of observational studies identified through searching five electronic databases and reference lists. Studies were required to have both a recognised cognitive function assessment (either a structured neuropsychological test or a clinical evaluation of dementia), and assessment of the retinal microvasculature (either characteristics associated with generalised retinopathy or changes specific to arterioles or venules).
Results: 6 studies were included. Studies were clinically and methodologically heterogeneous and of variable quality. Some degree of cognitive impairment was found to be associated with the presence of retinal microvascular abnormalities in all studies, although the extent of the association varied. The presence of retinal vascular signs was mostly associated with poorer verbal memory, mental speed and executive function in the general population, but not consistently associated with other cognitive modalities.
Conclusions: There is some evidence suggesting a positive association between retinal microvascular abnormalities and cognitive impairment or dementia in elderly people and in patients with diabetes. Findings are inconclusive, and further better designed studies are required, with standardised and objective retinal vascular assessment and a range of sensitive cognitive tests.
Statistics from Altmetric.com
Cognitive impairment and dementia are important causes of morbidity and mortality in elderly people in Western countries. Apart from the effects of normal ageing, marked inter-individual differences in the rate of cognitive decline indicate that other age-associated pathologies may be involved, such as macro- or microvascular disease. Current primary prevention programmes, aimed at reducing the impact of macrovascular disease, have proved unsuccessful in reducing the risk of cognitive decline, other than by preventing major strokes.1–5 Improved prevention of cognitive dysfunction therefore requires a better understanding of underlying pathogenic mechanisms, identification of novel risk factors and development of new approaches to recognition of people at high risk.6
Several pathobiological markers have been suggested as potential predictors of cognitive dysfunction. These include non-invasive measures of cerebral microvascular disease, such as white-matter hyperintensities and lacunar infarcts detected by magnetic resonance imaging (MRI), and retinal microvascular signs.7–9 Of these, retinal microvascular signs may offer the most promise as a potential tool in clinical practice, as they can be simply and accessibly measured. Based on retinal photographs, retinal microvascular abnormalities, such as the presence of microaneurysms, soft exudates, haemorrhages and generalised arteriolar narrowing, predict incident stroke as well as MRI-identified subclinical stroke independent of other measured risk factors.10–13 Recently, influenced by the homology between retinal vascular disease and cerebral small vessels disease, several studies have investigated retinal microvascular abnormalities and risk of cognitive impairment and dementia in patients and in the general population. These studies are reviewed systematically in this article.
METHODS
We aimed to include all published studies that investigated the association between retinal microvascular abnormalities and cognitive dysfunction in adult subjects, available for review by July 2007. Studies had to meet the following predetermined inclusion criteria: (a) observational epidemiological design (ie, cross-sectional, case-control, cohort), (b) inclusion of a cognitive function assessment tool that was either a structured neuropsychological test or a clinical evaluation of dementia, (c) assessment of the retinal microvasculature (either characteristics associated with generalised retinopathy or changes specific to arterioles or venules, such as focal arteriolar narrowing or venular tortuosity) but not other retinal conditions, which fail to offer a direct measure of retinal vascular signs (such as age-related maculopathy), (d) provision of data relating retinal microvascular lesions to cognitive function. Studies in which participants were selected on the basis of existing infectious disease due to a virus or bacteria were excluded because cognitive dysfunction in these subjects is likely to have specific pathology peculiar to the infectious disease.
Studies were identified by computerised searches of PubMed (Medline), EMBASE, PsycINFO, BIOSIS Previews, and Web of Science, by checking the reference lists of relevant original and review articles, by reference to conference proceedings, and by tracking articles that cited retrieved studies using Science Citation Index. A detailed “topic only” search strategy was adopted, as it proves the most sensitive. The search string for each database was similar with the terms “retinopath* OR (retina* AND (microvascu* OR arteriol* OR venul* OR vascu*)) AND (cognit* OR Alzheim* OR dementi* OR memor* OR neuropsycholog*).” Searches were limited to the English language. Further details on the search strategy are available from the authors on request.
The titles and abstracts of studies identified were screened by one reviewer (JD), and potentially relevant full-text articles were retrieved and assessed according to the inclusion criteria. Data were extracted by two reviewers (RJM and JD), who also independently assessed methodological quality of studies, using a scoring system based on previously published guidelines.14 15 The following information was extracted from included studies: method of assessment of retinal microvascular abnormalities, measurement of cognitive function, and all relevant results, including adjustment for potential confounding factors. Studies were assessed for both internal and external validity (Box). Studies scoring less than six out of a possible maximum nine for case control or cross-sectional studies, and less than seven out of 11 for cohort studies were excluded for further analysis. Disagreements in rating were resolved by discussion or arbitrated by a third reviewer (JP). Owing to a high degree of heterogeneity between studies, including study designs, type of population, measures of retinal vascular characteristics, types of neuropsychological tests and covariates included in analyses, meta-analysis of study results was not possible. A descriptive synthesis approach was therefore used.
Box 1 Quality assessment of studies
Participant selection and recruitment (maximum 2 points)
Well-defined population sample (the final study sample was likely to be representative of the target population) (1)
(Baseline) response rate 70% or more (1)
Participation at follow-up (maximum 2 points)
Follow-up period more than 1 year (1)
Loss to follow-up less than 30–40% (death was excluded from the estimate) (1)
Retinal microvascular abnormalities assessment (maximum 3 points)
Retinopathy status based on self-report or medical records (0)
or
Ophthalmoscopic examination (1)
or
Retinal photography and grading based on a standardised protocol (2)
Assessors blinded to cognitive status (1)
Cognitive function and/or dementia assessment (maximum 3 points)
Only a global functioning test (1)
or
Neuropsychological battery (2)
or
Dementia based on medical records (0)
or
Dementia diagnosed by active screening with specific criteria (1)
or
Dementia based on worldwide recognised criteria by a central consensus committee (2)
Assessors blinded to ocular findings and other major clinical disease status (1)
Adjustment for confounding (maximum 1 point)
Effect of main confounders not investigated (at baseline) (0)
or
Main confounders reported but not adjusted in the final analysis (0)
or
Main confounders reported and adequately adjusted in the analysis (1)
Eligible studies: scoring ⩾7/11 for cohort studies and ⩾6/9 for case-control/cross-sectional studies
RESULTS
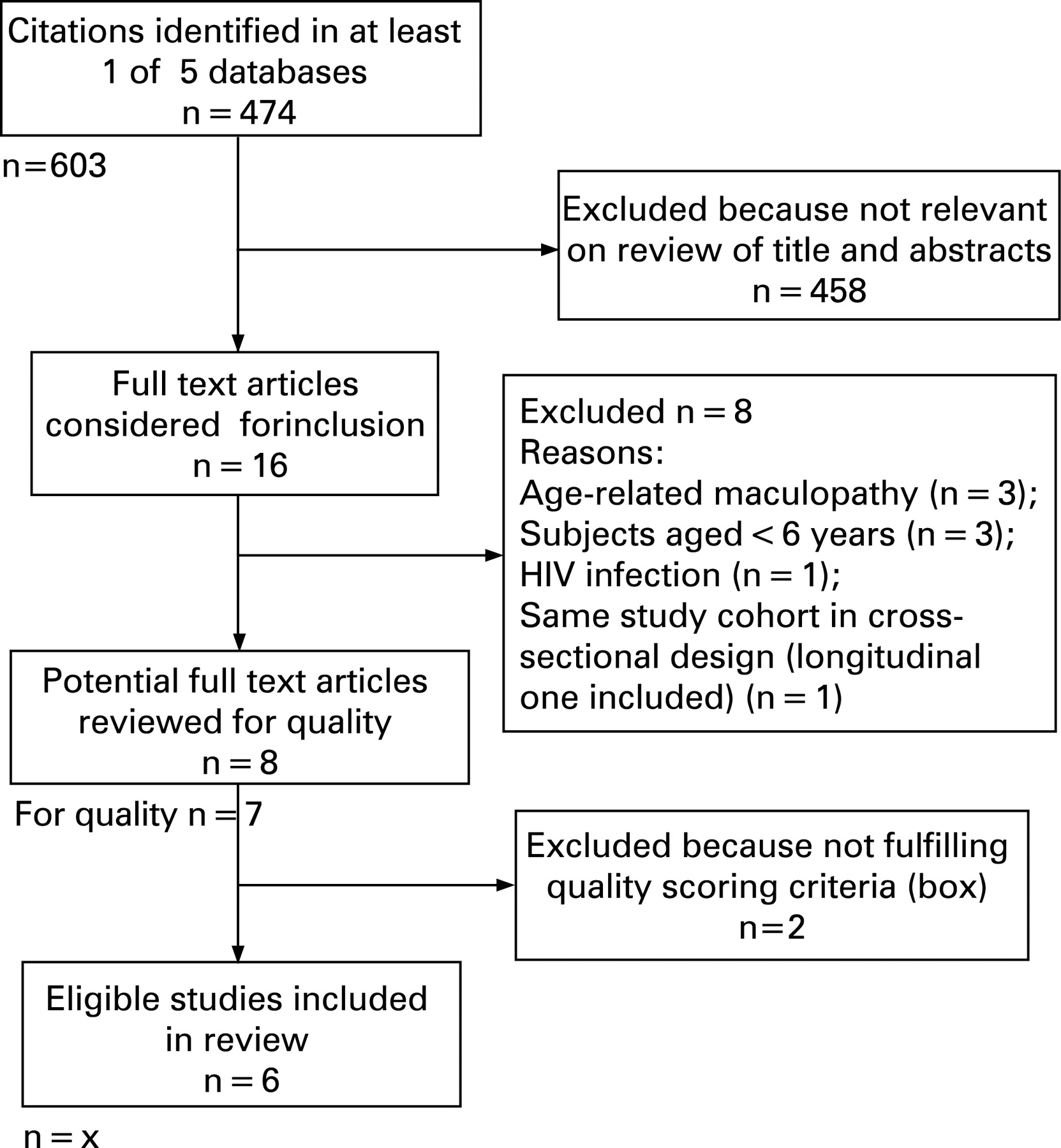
The numbers of studies identified at each stage of the systematic review are shown in fig 1. Of the eight studies meeting our inclusion criteria,16–23 two were subsequently excluded, as they did not fulfil the quality criteria.16 17 The key details of the six included studies are summarised in tables 1, 2.

{kind=link}
Study design and populations
The six included studies comprised two prospective cohort studies in which cognitive function was measured both at baseline (when retinal images were taken) and at follow-up,18 19 and four cross-sectional studies.20–23 Three studies were population-based21–23 and three hospital- or clinic-based.18–20 The populations sampled came from the US, UK and Japan. The clinic and hospital-based studies involved patients with type 1 or type 218 20 and patients with type 2 diabetes after coronary artery bypass grafting (CABG).19 The age range of participants (at baseline) was 18–35 years18 to 83–84 years23 and all studies included both men and women. In the prospective studies, the duration of follow-up was 6 months and 7 years, respectively, with losses to follow-up estimated to be 5%19 and 39%.18
In three of the four cross-sectional studies, a retinal examination was undertaken at the same time as the cognitive testing. In the other study, the cognitive function tests were performed 3 years before or after retinal photography, and the average test scores were used in the analysis.21 One prospective study in which cognitive abilities were assessed both at baseline and at 7 years’ follow-up examined the presence of retinopathy biennially as well as at baseline.18
Assessment of retinal microvascular abnormalities
Both the techniques and grading methods used to evaluate retinal microvascular signs varied between the studies. In one study, the combination of ophthalmoscopic examination with digital retinal photography was adopted,20 whereas in the remaining studies, colour fundus photography alone was used. Prior to retinal photography, pharmacological dilation of the pupil(s) was performed in two studies.18 23 The angle used for the field of view in photography differed, ranging from 30°18–20 to 45°21 22 or 50°.23 Three studies reported that only one eye was assessed21–23 (arbitrarily chosen) but the other studies did not provide such information.
In the studies using a fully manual grading system, subjects were categorised either according to the presence of diabetic retinopathy varying with severity,18–20 or into one of several defined groups, including the presence of: (1) any specific retinopathy signs (microaneurysms, retinal haemorrhages, cotton wool spots, soft exudates, macular oedema, venous beading, etc); (2) arteriovenous nicking; (3) focal arterial narrowing (table 3).21 22 At least three different classification systems for retinal vascular signs were used in five studies. Computer-assisted imaging techniques were applied in three studies to quantify retinal vessel calibre and other parameters of retinal vascular network geometry.21–23 One study focusing on quantitative measures alone assessed five continuous variables: the central retinal arterial equivalent (CRAE), central retinal venular equivalent (CRVE), arteriovenous ratio (AVR), suboptimal geometry of arteriolar branching coefficients and angles (table 3).23
Assessment of cognitive function and impairment
Cognitive function was assessed using four primary methods: (1) specific cognitive tests; (2) a mean/composite score on two or more tests in the battery;18 (3) general cognitive ability score (g) generated by extracting a component reflecting the variance shared by all tests;23 (4) clinical assessment alone (eg, diagnosis of dementia).22 Results were reported as either continuous or categorical outcomes. More than 17 different psychometric tests were used among these studies. To help organise discussion, many of these neuropsychological tests can be classified into the cognitive domains that they examined, including attention/concentration, information processing speed, manual dexterity, frontal lobe/executive function, verbal memory, performance IQ, and mini-mental state examination (table 4).28 29 In one study, patients with dementia were identified through a detailed diagnostic examination, and dementia was defined according to recognised international criteria.22 30
Three of the studies including one of the prospective studies divided the participants into two groups based on whether or not they experienced cognitive impairment or decline (during follow-up). Cognitive impairment was defined in a variety of ways that included: (1) a decline by a particular amount relative to the baseline test score;19 (2) test scores below a particular threshold score;21 or (3) the presence of clinically diagnosed dementia.
Findings from studies on patients with diabetes
The results of the studies on subjects with diabetes are shown in table 1.
In 74 patients with type 1 diabetes,20 the presence of retinal microaneurysms was associated with poorer performance on some tests of performance IQ (Block Design, Digit Symbol Test), information-processing speed and attention but not on other tests of performance IQ or executive function. In a second study of 103 patients with type 1 diabetes,18 the presence of proliferative diabetic retinopathy (PDR) at baseline or development of the condition during follow-up was associated with poorer performance on measures of “psychomotor efficiency” (a composite score based on the results of four tests: Digit Vigilance, Digit Symbol Test, Grooved Pegboard and Part B of the Trail Making). Compared with diabetic people without retinopathy at either assessment, there was a cognitive decline either in subjects with PDR at baseline (change in test score −0.50 vs −0.22, p<0.02) or in incident PDR (change in test score −0.56 vs −0.22, p<0.02) over 7 years. In both studies, the association remained significant after adjusting for a variety of demographic and several important diabetes-related variables. The magnitude of the cognitive deficits observed in these young adult subjects was moderate to large, with effect sizes for the group difference ranging from about 0.3 to 0.7 SD (according to Cohen’s terminology31).
In 180 patients with type 2 diabetes,19 after adjustment for a number of biomedical and demographic variables, the presence of diabetic retinopathy assessed prior to CABG surgery was associated with an increased risk of cognitive decline (compared with preoperative cognitive performance) after 7 days (OR 2.0, 95% CI 1.3 to 3.0) and 6 months (OR 2.1, 95% CI 1.2 to 2.7) following surgery.
Findings from studies on population-based samples
The results from population-based studies are shown in table 2.
In the Atherosclerosis Risk in Communities Study of 8,734 middle-aged men and women free of stroke,21 the presence of any retinopathy, microaneurysms, retinal haemorrhages or soft exudates was associated with an increased risk of impaired performance on tests of verbal memory (Delayed Word Recall), information-processing speed (Digit Symbol Test) and executive function (Verbal Fluency Test). The presence of arteriolar narrowing or AV nicking was not associated with these tests. Subjects with any of these retinal vascular lesions were 2.6 (OR (95% CI 1.3 to 2.9)) to 3.4 (OR (95% CI 2.0 to 5.8)) times more likely to have cognitive impairment than people without these lesions independent of other covariates.
In the Cardiovascular Health Study22 of 2,211 men and women, the presence of any retinopathy was associated with poorer performance on information processing speed (Digital Symbol Test, adjusted mean test scores 39 vs 42, p = 0.02), but not on the MMSE. No association was found with the presence of focal arteriolar narrowing, AV nicking or quintiles of retinal calibre. In a hypertensive subgroup, the presence of any retinopathy (multivariable-adjusted OR, 2.10 (95% CI 1.04 to 4.24)) or focal arteriolar narrowing (OR, 3.02 (95% CI 1.51 to 6.02)) was associated with an increased risk of dementia, but no association was found with the presence of other retinal vascular signs.
In the Lothian Birth Cohort 1921 study23 of 321 elderly men and women, the deviation from optimality of the retinal vascular network geometry was associated with lower cognitive ability scores, but no association was found for retinal arteriolar or venular calibre. After controlling for a variety of other covariates, suboptimality of angles at arteriolar bifurcations (from theoretically derived-optimum values) was associated with poorer verbal memory (Logical Memory) but not other cognitive modalities including general cognitive ability (g), executive function (Verbal Fluency Test) or performance IQ (Raven’s Matrices); suboptimal branching coefficient (from theoretically derived-optimum values) was associated with poorer general cognitive ability and verbal fluency but not other tests. The effect size of the variance in cognitive test scores explained by the retinal vascular abnormalities was small, ranging from 2.6% to 3.7%.
DISCUSSION
This is the first systematic review of the association between retinal vascular signs and cognitive dysfunction. Findings are consistent with the hypothesis that retinal microvascular abnormalities are associated with cognitive impairment or dementia in patients with diabetes and in the general population, although findings are not conclusive due to varied and sometimes limited methodology in the included studies. The presence of retinal vascular signs was mostly associated with poorer verbal memory, information-processing speed (Digit Symbol Test) and executive function (Verbal Fluency Test) in the general population. Furthermore, the longitudinal studies in this review may have underestimated the association with retinal abnormalities and cognitive function in patients with diabetes because of survival bias. Patients with diabetes with retinopathy at baseline were more likely not to attend for follow-up (including deaths), when follow-up success itself could well be related to good cognitive function, but the two studies did not report the retinopathy status of individuals lost to follow-up.18 19 Indeed, one study had a higher proportion of drop-outs.18
If there is indeed a direct relationship between retinal vascular abnormalities and cognitive function, this may reflect the homology between the retinal and cerebral microvasculatures.9 Similar to changes in the retinal vasculature, these microvascular changes might lead to chronic ischaemia of the brain and the development of white-matter lesions. In epidemiological studies, the presence of retinal vascular lesions that reflect a breakdown of the blood–retinal barrier, including microaneurysms, retinal haemorrhages and soft exudates, was related most consistently to stroke, stroke mortality, white-matter lesions and cerebral atrophy.10–13 Thus, the similar disruption of the blood–brain barrier of the cerebral microcirculation could be an important pathophysiological feature in the occurrence of cognitive impairment and dementia.32
Compared with ophthalmoscopic examination, the assessment of retinal photographs has been suggested as a more reliable method for measuring a number of retinal vascular signs, including generalised and focal arteriolar narrowing, arteriovenous (AV) nicking, isolated retinal haemorrhages, microaneurysms and cotton wool spots.6 33–35 Computer-assisted measures of retinal vascular widths (to define generalised arteriolar narrowing, venular dilation and other measures of retinal vascular network geometry) have been found to detect subtle microvascular changes with low intra- and inter-observer variability.10 13 35 36 Grading of other abnormalities (such as focal arteriolar attenuation and retinal haemorrhages) is still largely done manually and therefore highly operator-dependent, though automated techniques are being developed. The reliability of grading of focal retinal abnormalities has also been shown to be dependent on the classification system used.37 Despite the use of standardised protocols, differing methods and grading systems for measuring retinal microvascular abnormalities could explain at least in part some of the inconsistent findings between studies in this review.
Many observed changes in cognitive function of interest in studies are generally small,38 and mild cognitive impairment is an established risk factor for the subsequent development of dementia39 This requires measurement of cognitive function that use validated (sensitive to small increments of change) and reliable psychometric tests. In one of the studies, MMSE scores were used as a measure of cognitive function.22 However, the MMSE is a relatively insensitive test, which is designed to screen for dementia but not to measure subtle changes in cognitive decline.40–42
The majority of cross-sectional studies of cognitive function relied on cognitive performance at a single time point, which does not capture the pathological process under study—cognitive decline or change over time. Premorbid cognitive ability represents the highest level of ability attained prior to any cognitive decrements taking place and is also known to account for a substantial proportion of the variance in cognitive function scores in old age.28 43 44 Some studies estimated prior ability by a patient’s education and occupation history, but this is limited in that these features may be influenced by lack of opportunity rather than lack of ability.28 45 The National Adult Reading Test (NART) could be a more useful measure, as word reading ability is preserved even in generalised cognitive decline.45 Adjusting scores on a fluid mental test for NART has been shown to be a valid, instantaneous measure of lifetime cognitive change or decline.46 47 Only one study adjusted for premorbid IQ in an attempt to get a direct measure of lifetime cognitive decline.23
Most studies assessed important potential confounders such as age, gender, lifestyle factors and medical conditions. Patients with neurological conditions (including a history of stroke) that might interfere with cognitive abilities were also excluded from all studies. However, subjects with a history of chronic alcohol or drug abuse were only variably excluded. In addition, inadequate adjustment was generally made for visual acuity and depression. Some of the cognitive tasks may require at least moderate visual function to complete and if diabetic people with severe retinopathy have greatly impaired vision, their scores on the relevant cognitive testing could be affected. Two of the studies collected data on visual acuity18 23 and one study controlled for this.23 Depression may confound the association between retinal microvascular disease and cognitive dysfunction because depression can be mistaken for dementia (and vice versa), and is associated with deficits of memory and learning, and occurs more frequently in those with diabetes-related complications including retinopathy.48–53 Two studies assessed the potential effects of low mood.18 20
It should be noted that we reviewed only published studies, and it is possible that studies which did not show an association between retinal vascular disease and cognitive dysfunction may not have been published as often as studies that did. It was not possible to test for this formally (eg, by use of a funnel plot) because studies were too few and too methodologically heterogeneous. Clinic-based studies on patients with diabetes used variable inclusion criteria and this limited the generalisability of the results. Diabetes-related cognitive impairment may have different underlying mechanisms from cognitive dysfunction in the general population and may differ in patients with type 1 diabetes, type 2 diabetes and postoperatively. However, population-based studies are scarce so far restricted to a cross-sectional design, which makes it impossible to determine the temporal relationship between retinal vascular disease and cognitive dysfunction (though it is perhaps unlikely that cognitive impairment leads directly to retinal vascular abnormalities). Findings are not consistent regarding the importance of the association which are limited by substantial differences in methodology between the studies, small size of some of the studies, restricted controlling for potential confounding factors and variability in the range of cognitive domains and retinal microvascular abnormalities measured. Further better-designed studies are required, with a common, standardised and objective retinal vascular assessment, together with a range of sensitive cognitive tests.
Acknowledgments
We would like to thank M Dozier at Edinburgh University for help with literature searches and retrieval of references.
REFERENCES
Footnotes
Competing interests: None.