Article Text

Abstract
Aims: To evaluate the posthepatectomy survival of uveal melanoma patients with liver metastases.
Methods: Data were collected from the files in the Departments of Ophthalmology, General Surgery and Oncology, for uveal melanoma patients who were seen in the Ocular Oncology Clinic at the Hadassah Medical Center from 1988 to 2007. The main outcome was posthepatectomy survival. Statistical analysis was performed using JMP statistical software.
Results: Of the 558 patients, 74 (13%) developed metastases after a median of 35.0 months from the initial diagnosis. Thirty-five patients underwent hepatectomy. These patients had similar clinical characteristics as those who did not undergo hepatectomy. The median survival time from the detection of metastasis was 3.7-fold higher in the operated patients in comparison with the non-operated patients. Posthepatectomy survival of patients who were found in surgery to have 1–5 metastatic nodules was 3.1 times longer than those with six or more lesions. The hepatectomies of 13 patients resulted in complete resection of the hepatic metastases with clean histological margins (R0). These patients survived 1.9 times longer than those with residual disease (R1/R2).
Conclusion: It is possible to extend significantly the life expectancy of uveal melanoma patients who develop isolated hepatic metastases by complete resection of the lesions.
Statistics from Altmetric.com
Treatment of uveal melanoma has evolved from enucleating all eyes, to eye- and even sight-sparing treatments. The Collaborative Ocular Melanoma Study group (COMS) reported that even in 10 years of follow-up, brachytherapy with Iodine-125 (I-125) is as good as enucleation in terms of survival.1 However, in spite of excellent control of the local disease within the eye, patients still develop metastases leading to their death. Most of the metastases develop in the first 5 years after the diagnosis, but there have been reports of metastases appearing more than 25 years after the ocular treatment.2 The COMS reported a 25% metastatic rate in 5 years, with a death rate of 92% at 2 years following the diagnosis of metastatic disease.3 Uveal melanoma metastasizes primarily to the liver.34 Progression of the metastatic disease leads to additional locations for metastases, mostly lungs and bone, as reported from autopsies.5
There is a constant search for treatments for the metastatic disease using various chemotherapy agents, mainly fotemustine or a combination of gemcitabine and treosulfan administered intravenously, or more commonly into a hepatic intra-arterial port.6789 These treatments were found to extend the median metastatic survival (time from detection of metastases) up to 24 months.9 Additional research is being conducted on immunotherapy as an alternative or adjunctive treatment.10 Surgery is usually the initial step in treating the metastases, and its initial goal is to resect completely or debulk the metastases. An additional goal is to prepare the patients for additional treatments by inserting an intra-arterial port for chemotherapy, and obtaining tissue for the immunotherapy. A complete resection with clear histological margins (R0) is not always possible, but resection with microscopically involved margins (R1) or merely debulking the metastases (R2) is feasible in most of the patients.11
Here we report our experience with surgical treatment for metastatic uveal melanoma to the liver, and compare the outcome of the operated patients with that of metastatic patients who did not undergo any abdominal surgery.
Materials and methods
All patients with a diagnosis of uveal melanoma who were followed at the Ocular Oncology clinic of the Hadassah-Hebrew University Medical Center from 1 January 1988 through 1 January 2008 were included in this study. Data were available for 558 patients.12 Seventy-four of them developed metastases and are the study group for this report.
Patients were followed every 6 months. The systemic evaluation included abdominal ultrasonography (US) and liver function tests (alanine aminotransferase (ALT), aspartate-aminotrasferase (AST) alkaline phosphatase (ALK), gamma glutamyl transpeptidase (γGT), lactate dehydrogenase (LDH) and total bilirubin (TBil)). An upward trend in the liver function tests, even without exceeding the normal values,13 or suspicious lesions in the abdominal US, were verified by computed tomography (CT) of the abdomen. When fluorine-18 fluordeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) scanning became available in 2004, a combined PET-CT approach was used. A chest x ray was performed only at the time of diagnosis of uveal melanoma, as a baseline for future comparison.14
Surgical intervention was offered to patients who complied with the following criteria: (1) metastases confined to the liver; (2) liver imaging indicated a feasible curative resection; and (3) no prohibiting comorbidity.
Therapeutic protocol
All patients were approached with a curable intent as deemed by the preoperative evaluation. The surgery was initiated by a thorough exploration of the entire abdominal cavity. The liver was evaluated both by inspection/palpation and by intraoperative US to detect additional metastases that could not be identified by external imaging. Whenever possible, partial hepatectomy with clear histological margins (R0) was performed, and tissue was sent for histopathological diagnosis and cell culture for adjuvant immunotherapy preparation (this intervention will be referred to as “hepatectomy” throughout the manuscript). Patients were not operated on when (1) metastases were diagnosed before 1994; (2) they had known miliary disease by imaging; (3) they refused surgical treatment. Some patients received chemotherapy intravenously or through an intra-arterial hepatic port, and some received adjuvant immunotherapy. Data regarding the exact immunotherapy and chemotherapy protocols are beyond the scope of this manuscript.
We collected the following information from the patients’ medical records: demographic details; age at diagnosis of the ocular tumour; laterality of ocular involvement; intraocular location of the tumour; status of the extraocular disease; treatments for the ocular disease; time to metastasis; the metastases detection method and their preoperative numerical assessment; type of abdominal surgery performed; number of metastases found in the abdominal surgery; use of hepatic intra-arterial port for chemotherapy; histological surgical outcome (clear—R0, microscopic involvement—R1 or macroscopic involvement—R2); length of follow-up; length of survival from diagnosis and from the abdominal surgery, if applicable; and cause of death if applicable. The main outcome was posthepatectomy survival.
Statistical analysis (one-way analysis of variance (ANOVA), Kaplan–Meier product-limit (survival) analyses, Pearson χ2 test, and Wilcoxon signed-rank test) was done using JMP statistical software (SAS Institute, Cary, North Carolina) and SPSS Statistics (SPSS, Chicago).
Results
Seventy-four of the 558 patients (13%) developed metastatic disease 35.0 months (15.9 to 63.9 months) (median (interquartile range)) after the initial diagnosis. All the 74 patients had liver metastases. Four patients had additional metastases at other sites at the time of diagnosis of metastatic disease: one had a stomach metastasis, and three had lung metastases. One of the patients with lung metastases also had lesions in the adrenal gland and the thigh.
Seventy-three metastatic patients were sent for preoperative evaluation in preparation for a surgical intervention in an attempt to resect the liver metastases and to implant a hepatic port for intra-arterial chemotherapy. Metastases were diagnosed in one patient before surgical treatment became available in October 1994. Thirty-five patients underwent a liver resection. These patients had similar demographic and ocular characteristics to the patients who had not undergone hepatectomy in their gender, age, location of the primary tumour within the eye, primary tumour size, the primary treatment for the ocular tumour and the time to detection of metastatic disease. One eligible patient with a solitary liver metastasis underwent two embolisation attempts and refused any further treatment. Two additional patients refused any treatment for their metastatic disease. Two of the patients who had unresectable disease received alternative treatments: one received chemoembolisation and the other IV chemotherapy.
Table 1 summarises the type of procedures performed during the laparotomy. Table 2 provides the number of liver metastases found during surgery. Patients with six metastases or more were considered to have multiple lesions. The mean number of lesions for patients with five metastases or less was 2.3 (SD 1.6). Abdominal imaging with ultrasonography, CT and FDG-PET scanning underestimated the extent of liver involvement in eight patients who were found to have a disseminated (⩾6 metastases) or miliary liver disease intraoperatively by clinical impression and intraoperative ultrasonography. In five of these patients, we managed to resect the metastases by varying the amounts of liver resection. In the remaining three patients, the tumour was unresectable, and so they underwent only wedge sampling of metastatic tissue for pathological diagnosis and for immunotherapy. No significant surgical complications were experienced.
Type of abdominal surgery performed
Number of metastases detected during the abdominal surgery
By the end of the study period, 52 of the 558 patients (9%) were known to have died of metastatic disease, and 45 died of other causes. Table 3 provides the Kaplan–Meier product-limit (survival) analyses results. The survival of the entire metastatic group correlated highly with the metastasis-free interval, in years, from the initial diagnosis of uveal melanoma to the detection of liver metastases, when stratifying the metastasis-free interval into groups of ⩽1, 1–5 and >5 years (medians: 19.0, 61.1 and 141.7 months, respectively). However, the metastatic survival (survival from the diagnosis of metastases) did not differ among these metastasis-free-interval groups, unless we compared only the ⩽1 with the >5-year groups (11.4 vs 45.1 months).
Kaplan–Meier product-limit (survival) analysis
We compared the metastatic survival rates of patients who underwent hepatectomy with those who did not undergo surgery. No difference was found between these two groups in the median metastasis-free interval (35.0 vs 37.0 months, for the non-operated and operated groups, respectively). However, fig 1 shows that from the time of diagnosis of metastatic disease onwards, the survival rates of the patients who underwent surgery was significantly higher.
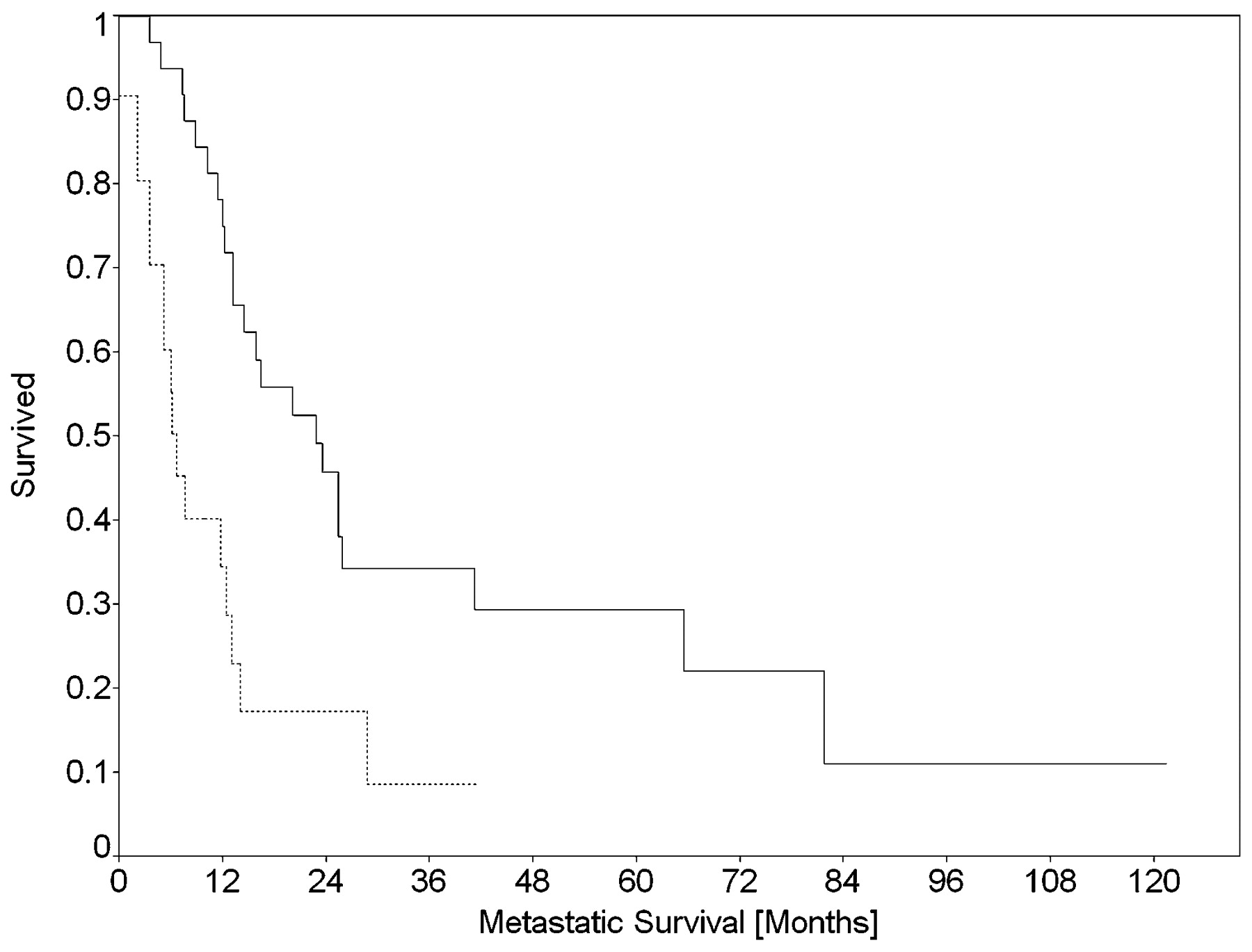
Effect of hepatectomy on the metastatic survival (time from detection of metastases) of uveal melanoma patients. Solid line, patients after hepatectomy; dashed line, non-operated patients.
A Kaplan–Meier survival analysis for the postoperative survival (metastatic survival) was performed per the number of lesions found in surgery, stratified by groups of one, two to five and six metastases or more. Patients with a single metastasis survived for 81.3 months (range 14.6 to 126.0 months), patients with two to five metastases survived for 29.7 months (range 9.0 to 65.9 months), and patients with multiple metastases or with miliary liver disease survived for 25.6 months (range 3.7 to 46.7 months). When the first two groups were combined into a group of one to five metastases, the median survival for this group was 55.2 months (range 9.0 to 126.0 months). Patients with one to five metastases had statistically significant higher survival rates than patients with six or more metastases. At the end of the study, 18% of the patients who had one to five hepatic lesions were still alive versus 9% of the patients who had six or more metastases.
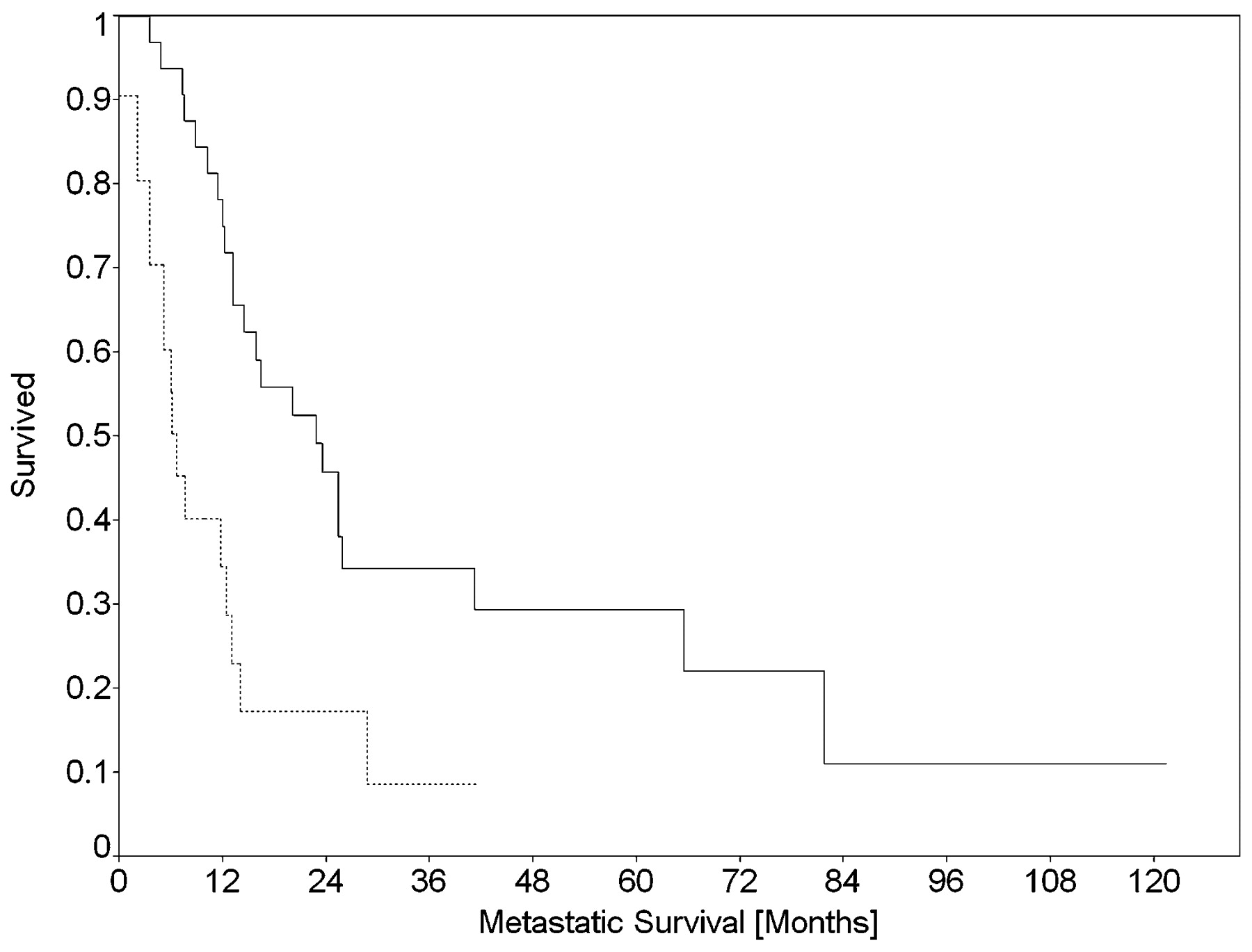
The aim of any surgical resection is to excise the tumour with clear histopathological margins (termed R0). This goal was reached in 13 patients. Their median posthepatectomy survival (fig 2) was almost fourfold longer than that of patients with residual disease, be it microscopic (R1) or macroscopic (R2) (R0: 65.6 vs R1/R2: 16.6 months). However, similar survival rates were noted after 12 months and at the end of the study (19% and 15% for Ro and R1/2, respectively) with no statistical significance (table 3). A high correlation was found between the number of lesions found in surgery (in groups of one, two to five and more than five metastases) and the probability of achieving a complete (R0) resection of the liver metastases (Pearson χ2 = 14.48, p = 0.0007).

{kind=link}
{kind=link}
Effect of the type of resection on the metastatic survival (time from detection of metastases) of uveal melanoma patients. The involvement of the surgical margins by residual tumour is termed: R0 resection, if there was no involvement (solid line), R1 resection, if there was a microscopic involvement, and R2 resection, if there was a macroscopic involvement (R1/R2—dashed line).
In nine patients, metastases recurred in the liver, and a second surgery was performed after a median of 7.4 months (range 1.1 to 63.3 months). When the metastases recurred, they appeared solely in the liver in five patients and in other organs in addition to the liver in four other patients: lung (one patient), lung and lymph nodes (one patient), lung and brain (one patient), skin and bone (one patient). In one patient, the metastases did not recur in the liver but appeared in the peritoneum and the lungs. There was no correlation between the status of the surgical borders (R0 or R1/2) and recurrence of the metastases (Pearson χ2 = 0.07, p = 0.7945).
Discussion
Our study encompassed uveal melanoma patients from a single National Ocular Oncology clinic over the past two decades. A total of 13% of our patients developed metastatic disease during the study period. The prognosis of patients from the time of diagnosis of metastases varies in the literature from 7 to 15 months.615 However, Pawlik et al reported that after surgical resection of the metastases, despite a 75% recurrence rate, their patients had a median survival of 23.6 months,16 with one patient even surviving for 93.7 months. Moreover, Aoyama et al reported on the survival of 12 patients who underwent surgical resection with survival ranging from 11 to 86 months.17 These median survival rates after “metastasectomy” are similar to the survival rates reported here.
Previous studies have found that patients who developed metastatic disease later did not survive longer with the metastases.151819 In our study, the metastatic survival period was independent of the metastasis-free survival. However, we found that patients who underwent hepatectomy had a more than threefold longer metastatic survival than metastatic patients who had not undergone abdominal surgery. It can be argued that this finding comes from a bias towards a worse survival for patients with a more disseminated disease who are less likely to be operated on. Bearing in mind that all our patients underwent a metastatic evaluation every 6 months, it could also be argued that if a patient developed multiple liver metastases in the same period of time that another patient developed only a few, the metastatic spread is more aggressive and could lead to a shorter survival. However, we conclude that the abdominal surgery has a beneficial effect on the survival in and of itself, and the finding of a longer metastatic survival for patients who underwent hepatectomy, by us and others,192021 supports the need to resect the liver metastases, whenever feasible, to prolong the patients’ survival.
Kodjikian and colleagues found that patients with more than 10 liver metastases had a fourfold risk of dying. Their choice of 10 as a cut-off was arbitrary despite the fact that the mean number of metastases in the “less than 10 lesions” group was three,19 similar to our finding for patients with fewer than six metastases. We found that patients with a single metastasis had a fivefold longer median survival than patients with diffuse or disseminated disease, and almost threefold longer median survival than patients with two to five metastases. A few solitary lesions, up to the three lesions reported by Kodjikian and colleagues, or up to the five lesions in our study, should be similarly resectable. The difference may imply that the surgery was performed at an earlier stage of the metastatic disease, thus leading to a better response to the treatment. However, it seems that the correlation between the number of lesions and the chances of completely resecting them has a major influence. This highlights the benefit of the surgical procedure for the patients’ survival, and the need for early detection of metastatic disease.
The first location for metastatic disease, in all our patients, was the liver. Yet, in three patients, the lung was also involved, and in one patient there was a metastasis to the stomach. It thus seems justified to concentrate the screening efforts on a combination of abdominal ultrasonography and various serum markers and to expose patients to irradiation by means of CT or PET-CT only when there are suspicious findings. A similar screening approach with abdominal ultrasonography is applied in other centres.182223 Freudenberg and colleagues reported a case in which a combined FDG-PET/CT found metastases not detected by CT alone.24 Since this test became available to us in 2004, we have utilised it in patients whose abdominal sonogram was suspicious for liver metastases, but in some cases both the CT and the PET could not account for the number of lesions detected during the surgery.
We have been working on methods for earlier detection of metastatic uveal melanoma by means of various serum biomarkers.25 We found these markers to be effective in diagnosing liver metastases, and preliminary findings show that these markers can detect the metastases months before they can be detected by imaging (US and CT) or by changes in the liver-function tests.13 Although the ideal serum marker is not yet at hand, the prospects of detecting the metastases at an early stage and treating them by surgical resection, immunotherapy and/or chemotherapy may bring hope for a much longer survival for these patients and maybe even a cure.
In conclusion, patients with one to five liver metastases, which could be fully resected with clear histopathological margins, survived much longer than patients who did not undergo abdominal cytoreductive surgery, irrespective of any additional intervention. Early detection of liver metastases and referral to surgery can prolong the life of uveal melanoma patients with metastatic disease. Further studies are required to improve the detection of metastatic disease and to offer additional treatment modalities towards a cure for these patients.
REFERENCES
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the Committee on Research Involving Human Subjects of The Hebrew University-Hadassah Medical School, Jerusalem, Israel.
Linked Articles
- At a glance