Article Text

Abstract
Background The purpose of this study is to evaluate the efficacy of intravitreal bevacizumab as the primary treatment of macular oedema due to retinal vein occlusions.
Methods Patients diagnosed as having central retinal vein occlusion (CRVO) or branch retinal vein occlusion (BRVO) with visual acuity of less than 20/40 and macular oedema with more than 300 μm central retinal thickness were recruited. Patients that had received any prior treatment were excluded. After an initial intravitreal injection of bevacizumab, re-treatment was performed if intraretinal or subretinal fluid with distortion of the foveal depression was found in optical coherence tomography.
Results 18 eyes with CRVO and 28 eyes with BRVO were included. During a 6-month period, the mean number of injections per patient was 3.7 (BRVO group) and 4.6 (CRVO group). In the BRVO group, mean baseline logMAR visual acuity was 0.80 (SD 0.38) and macular thickness was 486.9 μm (SD 138.5 μm). After 6 months, mean logMAR visual acuity improved significantly to 0.44 (SD 0.34), p<0.001. Mean macular thickness decreased significantly to 268.2 μm (SD 62.5 μm), p<0.001. In the CRVO group, mean baseline logMAR visual acuity was 1.13 (SD 0.21) and macular thickness was 536.4 μm (SD 107.1 μm). Mean final logMAR visual acuity improved significantly to 0.83 (SD 0.45), p<0.001. Mean macular thickness decreased significantly to 326.17 μm (SD 96.70 μm), p<0.001.
Conclusions Intravitreal bevacizumab seems to be an effective primary treatment option for macular oedema due to retinal occlusions. Its main drawback is that multiple injections are necessary to maintain visual and anatomic improvements.
- Retinal vein occlusions
- bevacizumab
- macular oedema
- treatment
- branch retinal vein occlusion
- central retinal vein occlusion
- retina
- macula
- drugs
- treatment surgery
Statistics from Altmetric.com
- Retinal vein occlusions
- bevacizumab
- macular oedema
- treatment
- branch retinal vein occlusion
- central retinal vein occlusion
- retina
- macula
- drugs
- treatment surgery
Retinal vein occlusions are a frequent cause of visual impairment. Central retinal vein occlusion (CRVO) is less common than branch retinal vein occlusion (BRVO); however, in both cases, the development of macular oedema is the main cause of visual loss. Treatment remains controversial. The Central Retinal Vein Occlusion Study Group found that laser treatment had a beneficial effect on neovasculatization, but it failed to produce visual improvement in macular oedema.1 The Branch Vein Occlusion Study provided evidence that grid laser photocoagulation of the oedematous macular area leads to a statistically significant benefit in terms of visual acuity and persistence of macular oedema as compared to the natural course of the disease.2 However, mean improvement in visual acuity was only 1.3 lines, and laser treatment leads to the development of scotomas.2
Triamcinolone acetonide represents an alternative to laser treatment for retinal vein occlusions. Although results are positive in terms of reduction of macular oedema and improvement in visual acuity, its effects are only transient, requiring repeated injections.3 4 Furthermore, its use has been associated with the development of posterior subcapsular cataracts and elevation of the intraocular pressure.3–5 Initial treatment outcomes of a long-acting intravitreal fluocinolone acetonide sustained drug delivery implant have been reported in eyes with CRVO and chronic refractory macular oedema.6 Although visual acuity improved in a significant proportion of eyes, with a reduction in macular oedema, cataracts developed in all phakic patients in the study, and 13 of 14 eyes required medical or surgical interventions to lower intraocular pressure.6 Two clinical trials are ongoing to evaluate the treatment of macular oedema in retinal vein occlusions with intravitreal corticosteroids: first is the multicentre randomised study SCORE, which compares the effectiveness and safety of standard care versus triamcinolone acetonide injection in patients with CRVO and BRVO; second is a phase III trial that evaluates the effect of an intravitreal sustained dexamethasone drug delivery system (Posurdex) versus observation for macular oedema secondary to retinal vein occlusions.7 Different surgical approaches have also been reported for the treatment of CRVO (vitrectomy with radial optic neurotomy) and BRVO (vitrectomy with or without sheathotomy at the arteriovenous crossing).8
Vascular endothelial growth factor (VEGF) is a cytokine produced by the hypoxic retina that increases vascular permeability, leading to macular oedema. VEGF also stimulates endothelial cell hypertrophy, which reduces the capillary lumen and causes more ischaemia and thus tends to perpetuate the oedema. Anti-VEGF treatment could break this cycle and facilitate resolution of macular oedema. Bevacizumab (Avastin; Genentech, Inc, San Francisco, California, USA) is a monoclonal antibody that inhibits all isoforms of VEGF. It has been used off-label to treat several ischaemic and oedematous diseases. The purpose of this study is to evaluate the efficacy and safety of intravitreal bevacizumab as the sole treatment of retinal vein occlusions presenting with decreased visual acuity due to macular oedema.
Patients and methods
This is a prospective non-randomised interventional case series of patients diagnosed as having CRVO or BRVO. Ethics committee approval was obtained. The experimental, off-label use of bevacizumab was explained in detail to all patients before inclusion in the study and all patients gave informed consent.
At the visit before inclusion in the study, all patients underwent a complete ophthalmological examination, including best-corrected visual acuity, biomicroscopy of the anterior and posterior segments, intraocular pressure measurement (Goldman applanation tonometry) and macular evaluation with optical coherence tomography, Fast Macular Thickness Map protocol, StratusOCT (Carl Zeiss Meditec, Inc, Dublin, California, USA). Central retinal thickness was measured with the Retinal Map analysis protocol in a circle of 1 mm in diameter centred on the fovea. Optical coherence tomography was repeated on each follow-up visit.
Inclusion criteria were as follows: visual acuity of less than 20/40 and macular oedema of more than 300 μm of central retinal thickness in optical coherence tomography. Patients previously treated for retinal vein occlusions or with any other ocular diseases were not included in the study.
Bevacizumab injections of 1.25 mg/0.05 ml were administered under sterile conditions in the operating theatre. Antibiotic drops were prescribed for 1 week, starting 3 days before the injection.
Patient follow-up was performed 1 day, 1 week and 1 month after each injection and monthly thereafter. Eyes were re-treated if either intraretinal or subretinal fluid with distortion of the normal foveal depression was found in the optical coherence tomography examination.
Statistical analysis was performed with SPSS 13.0 software. Visual acuity was converted to logMAR before analysis. Quantitative variables are described with mean, median and range, and qualitative variables as percentages. The Shapiro–Wilk test was used to evaluate whether the variables analysed followed a normal distribution. Since variables did not follow a normal distribution, non-parametric tests were performed to evaluate changes in visual acuity and retinal thickness.
Results
Forty-six patients were included in the study, 18 patients with CRVO and 28 patients with BRVO. Twenty-one patients were women (46%) and 25 men (54%), with a mean age of 63.96 years (range between 50 and 78 years). No significant complications developed in either group after treatment with bevacizumab.
BRVO group
In the BRVO group, the mean baseline logMAR visual acuity was 0.80 (SD 0.38; range 0.30–1.30); Snellen equivalent was 0.22 (SD 0.16; range 0.05–0.5). Mean baseline macular thickness was 486.9 μm (SD 138.5 μm; range 302–753 μm). The mean time elapsed between the diagnosis of BRVO and the first bevacizumab injection was 4 months (range from 5 days to 2 years).
Every patient was followed for at least 6 months after the first injection. During these 6 months, the mean number of injections per patient was 3.7 (range 1–6). Only one case resolved after a single injection.
Visual acuity improved progressively throughout the follow-up period (figure 1A), although the main improvement occurred during the first 2 months. This improvement was statistically significant as compared to baseline visual acuity at all visits (figure 1A). At 6 months of follow-up, mean logMAR visual acuity was 0.44 (SD 0.34; range 0–1.30); Snellen equivalent was 0.46 (SD 0.28; range 0.05–1). Figure 2A shows the percentage of patients that gained two or more Snellen lines, remained stable and lost two or more lines. Only two patients lost two or more lines as compared to baseline during the first 2 months of treatment; however, after 3 months, vision improved or remained stable in all cases. The median improvement at 6 months was two Snellen lines. Final visual acuity was 0.5 or better (Snellen) in only 14% of patients with a baseline visual acuity equal to or lower than 0.2, as compared with 100% of patients with a baseline visual acuity higher than 0.2.

Branch retinal vein occlusion group. (A) Snellen visual acuity (VA) at baseline and at each visit. (B) central macular thickness at baseline and at each visit (p values provided are those of the comparison between each visit and baseline values, Wilcoxon test).
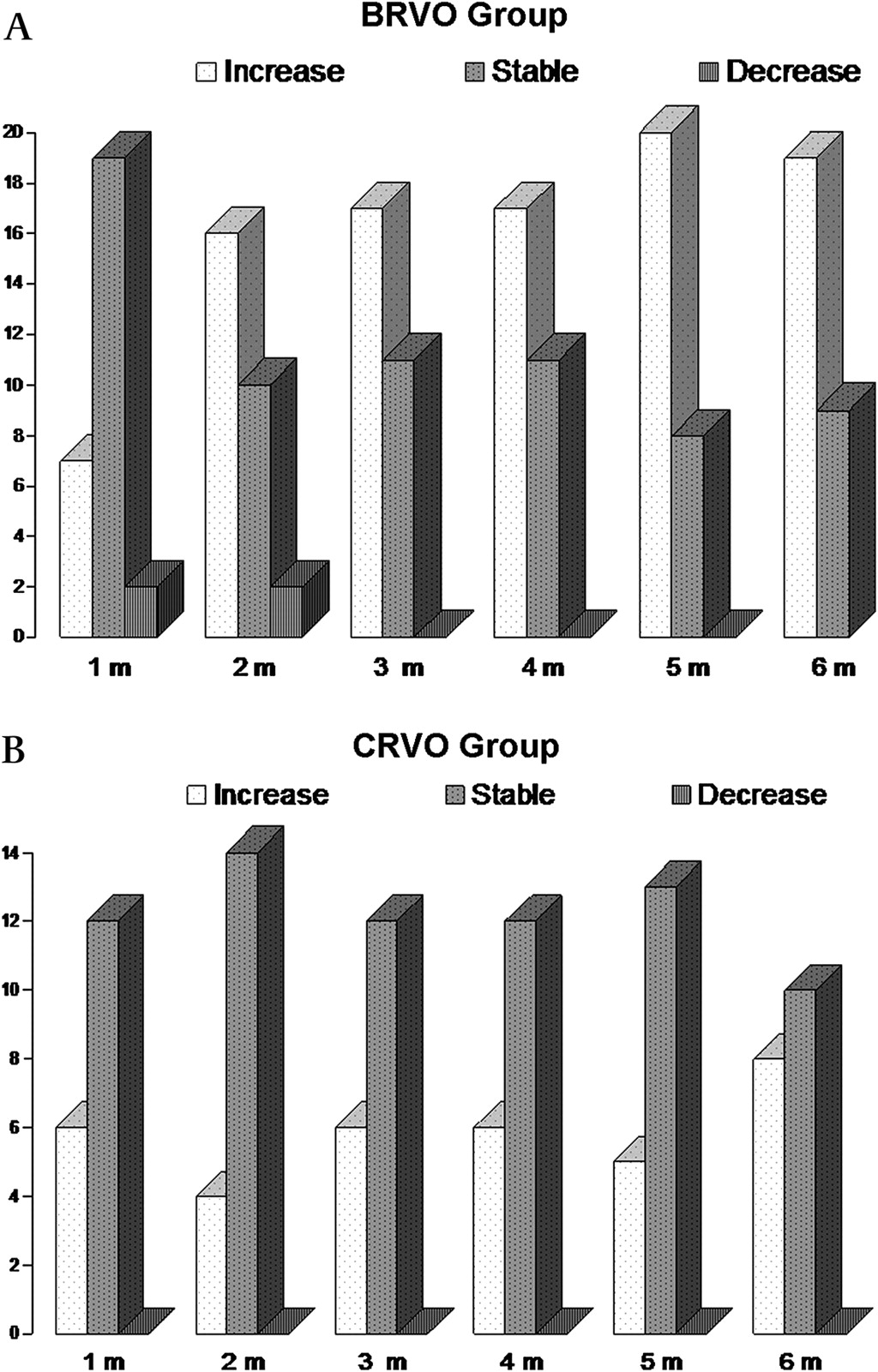
Number of patients in which visual acuity remained stable, increased by two or more Snellen lines or decreased by two or more Snellen lines at each visit. (A) Branch retinal vein occlusion (BRVO) group. (B) Central retinal vein occlusion group (CRVO). m, months.
Mean macular thickness decreased significantly after the injection of bevacizumab (p<0.001; Wilcoxon test). The reduction persisted throughout the whole follow-up period (figure 1B). Final mean macular thickness was 268.2 μm (SD 62.5 μm).
Preinjection visual acuity was significantly correlated with macular thickness before treatment (p<0.001, R=0.686) and with final visual acuity (p<0.001, R=0.772). Similarly, final visual acuity was significantly correlated with preinjection macular thickness (p=0.001, R=0.597) and with macular thickness at 6 months (p=0.001, R=0.578).
CRVO group
In the CRVO group, mean baseline logMAR visual acuity was 1.13 (SD 0.21, range 0.7–1.30); Snellen equivalent was 0.08 (SD 0.05; range 0.05–0.2). Mean baseline macular thickness was 536.44 μm (SD 107.14 μm; range 400–757 μm). The mean time elapsed between the diagnosis of CRVO and the first bevacizumab injection was 6 months (range 1 week to 2 years).
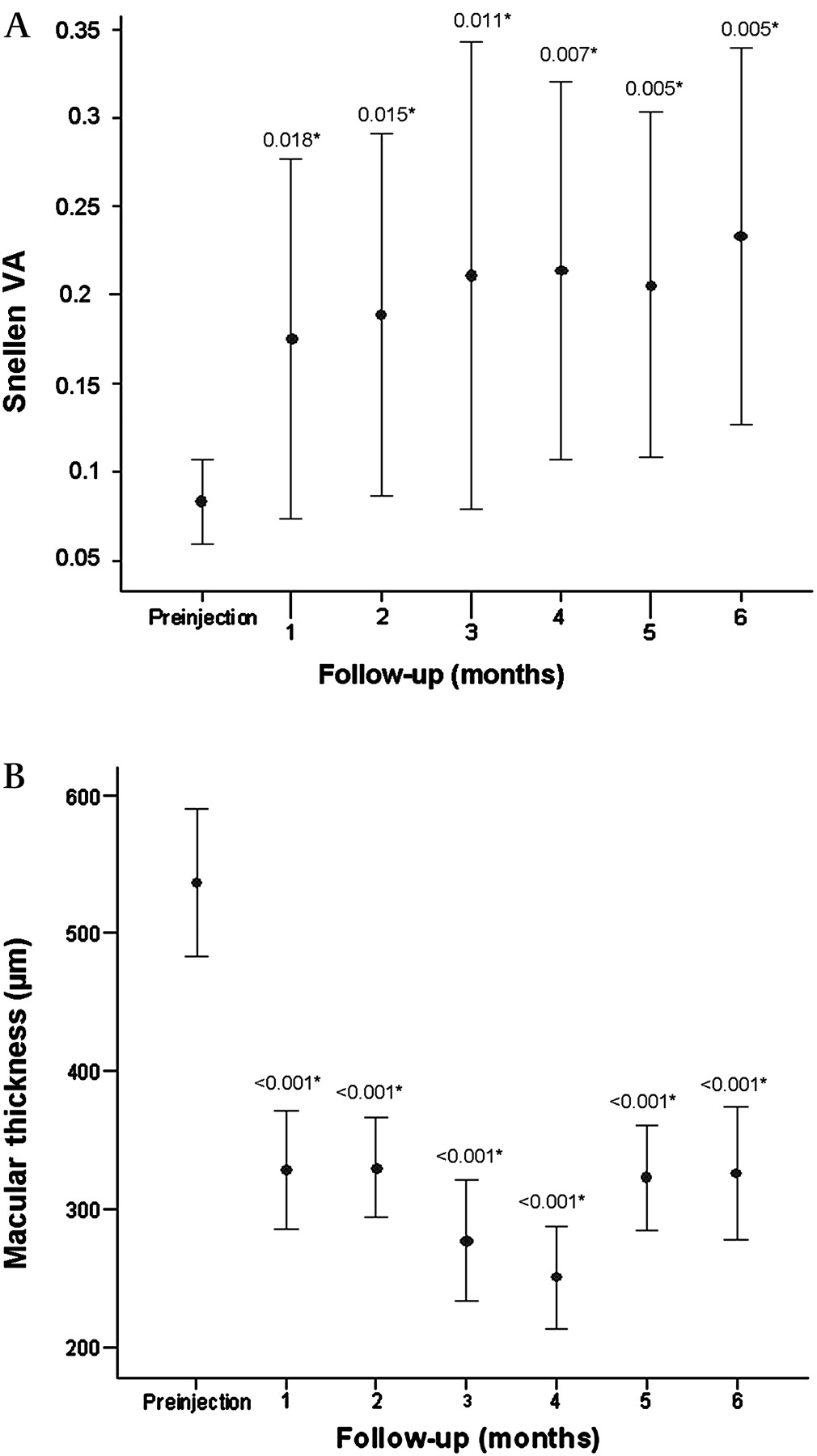
During the 6-month follow-up, the mean number of injections per patient was 4.6 (range 3–6). Mean final logMAR visual acuity was 0.83 (SD 0.45; range 0.15–1.30); Snellen equivalent was 0.23 (SD 0.21; range 0.05–0.7). Visual acuity improved progressively, although the main improvement occurred in the first month. This improvement was statistically significant compared to baseline visual acuity at all visits (figure 3A). Median improvement at 6 months was one Snellen line.

{kind=link}
{kind=link}
{kind=link}
Central retinal vein occlusion group. (A) Snellen visual acuity at baseline and at each visit. (B) central macular thickness at baseline and at each visit (p values provided are those of the comparison between each visit and baseline values, Wilcoxon test).
Mean macular thickness decreased significantly after injections of bevacizumab (p<0.001; Wilcoxon test). This reduction persisted throughout the follow-up period (figure 3B). Final mean macular thickness was 326.17 μm (SD 96.70 μm).
Preinjection visual acuity was significantly correlated with macular thickness before treatment (p=0.002, R=0.679) and with final visual acuity (p<0.001, R=0.781). Similarly, final visual acuity was significantly correlated with preinjection macular thickness (p=0.07, R=0.613) and with macular thickness at 6 months (p=0.044, R=0.479). A correlation was also found between macular thickness reduction at 1 month and final visual acuity: for each 100 μm of macular oedema reduction, there was an improvement of one line in visual acuity.
Discussion
Retinal vein occlusions cause visual loss due to initial hypoxia and delayed macular oedema. The oedema may cause an additional reduction in visual acuity that often exceeds the primary ischaemic damage; it is the most frequent complication of vein occlusions.9 It has been shown that intravitreal levels of VEGF are significantly increased after retinal vein occlusions and that the degree of macular oedema is correlated with VEGF levels in aqueous humour.10 Therefore, several authors have studied the usefulness of intravitreal injections of bevacizumab in both types of retinal vein occlusions.9
Previous reports suggest that visual results are better in BRVO as compared with CRVO. The mean visual acuity improvement was about 0.3 logMAR units in most series of BRVO treated with bevacizumab.11–14 An important feature of our study was that prior treatment was an exclusion criteria: patients were treated exclusively with bevacizumab. Few reports have prospectively studied patients with BRVO having bevacizumab as the sole treatment.
Russo et al13 evaluated bevacizumab versus macular grid laser photocoagulation for macular oedema in 30 patients with BRVO: after treatment, eyes receiving bevacizumab had better visual acuity than those receiving photocoagulation at all times. Visual acuity improved by 0.3 logMAR units 6 months after treatment with bevacizumab. Rensch et al evaluated the results of early treatment with bevacizumab after BRVO: mean visual acuity improved by 0.21 logMAR units 6 months after treatment.11 In this study, mean logMAR visual acuity improved by 0.36 logMAR units after treatment. Thus, most studies to date report similarly positive visual acuity results after the injection of bevacizumab.
Most series have also shown a significant decrease in macular thickness after treatment with bevacizumab, although it is not always correlated with visual acuity. Rensch et al found that the improvement in visual acuity correlated significantly with the decrease in macular thickness.11 We have found that initial and final macular thicknesses are correlated with final visual acuity. There may be several explanations for these results. Chung et al found that in the group of BRVO with no visual improvement, there was a higher proportion of angiographically documented macular ischaemia.15 In this group, the decrease in central macular thickness was not accompanied by a visual acuity improvement. Although baseline visual acuity was not statistically different between groups, patients with no visual improvement had lower visual acuities than those who improved. They also found that those patients who responded early to the first injections were more likely to benefit from bevacizumab treatment. Better initial visual acuities may reflect a preservation of macular function that may not be directly correlated with macular thickness; this would explain why patients with poor initial visual acuity often have poor final visual acuity in spite of the reduction of macular oedema.
Visual results are much more variable in patients with CRVO, since no visual benefits, minimal improvements of nine letters or significant visual acuity improvements have been published.16–21 In our study, mean visual acuity improvement was 0.30 logMAR units, which is similar to that described by Rensch et al in a series of patients with macular oedema caused by non-ischaemic CRVO, with a mean duration before the first injection of 4.2 days (SD 3.6).21 In our study, mean macular thickness in patients with CRVO decreased significantly after treatment. As in the patients with BRVO, macular thickness was correlated with visual acuity. Rensch et al also found that the improvement in visual acuity correlated significantly with the decrease in macular thickness.11 21 Again, not all studies have found a relationship between retinal thickness and visual acuity in patients with CRVO. Beutel et al published a retrospective study with intravitreal bevacizumab for non-ischaemic CRVO in which they obtained a significant decrease in central retinal thickness without significant improvement of visual acuity after 12 months of follow-up.17 In a prospective study of ranibizumab for macular oedema due to CRVO, visual acuity and central retinal thickness were not correlated.16 Sakamoto et al found that the preservation of the foveal inner/outer segment photoreceptor line after resolution of macular oedema was significantly correlated with good visual function.22 As in BRVO, initial visual acuity may reflect macular function and thus bevacizumab may lead to poorer visual improvement in patients with CRVO as compared with patients with BRVO because the macular function may be more seriously damaged due to the greater size of the initial ischaemia in CRVO.
No significant complications developed in our series after treatment with bevacizumab. The main drawback of bevacizumab for the treatment of macular oedema after retinal vein occlusions is the need for repeated injections.11 13 15–18 21–24 No re-treatment schedule has been defined and new injections are performed at monthly or longer intervals at the discretion of the treating physician. However, Jaissle et al observed that the number of reinjections necessary to maintain the effect in BRVO declined over time.12 Although an optimal treatment regimen is as yet unclear, our data suggest that treatment should be initiated even if BRVO or CRVO have been present for some time: in our patients, the temporal delay (range from 5 days to 2 years) from diagnosis to treatment initiation did not influence visual outcome, as reported in other series. An additional benefit that bevacizumab injections may provide as compared with other treatment options is that it may prevent the development of neovascularization or lead to its regression if it is already present.
In summary, this case series supports previous reports that suggest that bevacizumab is a valid, effective treatment for macular oedema due to retinal vein occlusions. However, randomised multicentre studies are necessary to determine the optimal time after the vascular event for initiation of treatment and the schedule of injections.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Comité de Ética del Hospital Universitario Ramón y Cajal.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance