Article Text

Abstract
Aim To evaluate the therapeutic effect of continuous treatment with topical dorzolamide (a carbonic anhydrase inhibitor) for cystoid macular oedema (CME) associated with retinitis pigmentosa (RP).
Methods 18 eyes in 10 patients with CME secondary to RP were included. Baseline visual acuity, visual field and optical coherence tomography (OCT) measurements were obtained for all patients. All patients used 1% dorzolamide three times daily in each affected eye. Patients underwent follow-up examinations at 1, 3, 6, 12 and 18 months after treatment. The response to treatment was monitored by the Humphrey field analyser (HFA: the central 10-2 program); in addition, foveal thickness was measured by OCT. Evaluation of ‘macular sensitivity’ was calculated by HFA as the average of 12 central points.
Results The ‘macular sensitivity’ in 10 eyes in which CME was almost completely resolved was significantly improved (p<0.05). In eight of the nine eyes in which CME was almost completely resolved within 6 months, the therapeutic efficacy persisted through 18 months. Five eyes which were almost completely resolved or showed an initial response within 6 months experienced recurrence of CME.
Conclusions The prolonged (longer than 1 year) use of topical dorzolamide is effective for the treatment of CME in patients with RP. Therefore, we propose topical dorzolamide treatment as a first choice.
- Retina
Statistics from Altmetric.com
Introduction
Retinitis pigmentosa (RP) is a heterogeneous group of inherited retinal diseases caused by mutations in various genes (more than 45 responsible genes).1–3 Patients typically report impaired night vision and a gradual loss of visual fields.4–6 Macular complications such as cystoid macular oedema (CME) and the development of an epiretinal membrane lead to unexpected central vision impairment. CME is one of the common complications associated with RP. The prevalence of CME in RP is 10–40% and the condition is usually bilateral.7–9 The condition causes blurred vision, reduced visual acuity and subsequent atrophic changes in the fovea, and thus it is necessary to find an effective treatment for CME in RP patients.
The exact mechanism of its aetiology in RP is poorly understood, however one putative mechanism of CME is thought to be a failure of the pumping activity in the retinal pigment epithelium (RPE).10 Treatment with a carbonic anhydrase inhibitor (CAI) may modulate membrane-bound carbonic anhydrase IV in the RPE and restore the pumping activity in the RPE.11–13 Many previous reports have shown the efficacy of CAI for the management of CME in patients with RP.10–16 However, severe side effects have been associated with oral administration of CAI.10 ,14 ,15 Grover et al first reported the efficacy of a topical dorzolamide.11 In similar fashion, we previously demonstrated significant improvement in macular function as well as a significant decrease in retinal thickness in response to topical dorzolamide treatment within a short period.16 Although other reports have shown that continued treatment with topical dorzolamide was also effective, a certain percentage (about 50%) of no response or rebound was observed.12 ,13 Thus we need the efficacy criteria for the continued treatment of topical dorzolamide.
In the present study, we investigated the longer than 1-year therapeutic efficacy of a topical CAI for the management of CME in patients with RP. The response to treatment was monitored by ‘macular sensitivity’ using the Humphrey field analyser (HFA: the central 10-2 program), in addition to the foveal thickness measured by optical coherence tomography (OCT).
Methods
This prospective study included 10 consecutive patients (one male and nine female) diagnosed with CME secondary to typical RP. Patients with CME secondary to an epiretinal membrane or vitreal traction were excluded. All patients were seen at Kyushu University Hospital (Fukuoka, Japan) from June 2010 to January 2011. The study was approved by the Institutional Review Board of Kyushu University and was conducted in accordance with the tenets of the Declaration of Helsinki on biomedical research involving human subjects. Informed consent for the research was obtained from all 10 patients.
The diagnosis of RP was based on the patients’ history of night blindness, side vision restriction, and markedly reduced or non-recordable a- and b-wave amplitudes on electroretinogram testing, in addition to ophthalmoscopic findings (ie, characteristic fundus changes in attenuated retinal vessels and bone-spicule-like pigment clumping). We excluded patients with uveitis and those diagnosed with any disease that could cause RP-like fundus changes. All 10 patients had a cystic lesion in the fovea that was apparent on fundus examination and was confirmed by OCT measurement.
Ophthalmic data collection
Best-corrected visual acuities (BCVAs) at baseline and subsequent visits were obtained for all patients with full subjective refraction using a Landolt ring chart at 5 m. Visual acuity was converted into a logarithm of the minimal angle of resolution (logMAR) for statistical analysis. Slit-lamp biomicroscopy of the anterior segment and funduscopic examination by both direct and indirect ophthalmoscopy were also carried out on all patients. Intraocular pressure was measured at baseline and at subsequent visits by a non-contact tonometer.
Baseline OCT measurements were obtained for all patients by spectral domain OCT (SD-OCT; Cirrus, Carl-Zeiss Meditec, Dublin, California, USA) as previously described.16 Research software V.3.0 (Carl-Zeiss Meditec) was used to measure central subfield thickness (CST). The average thickness of all points within the inner circle of 1 mm diameter was defined as CST of the fovea. We defined the almost complete resolution (which showed well defined central foveation with only a few small cystic lesions) or more than 20% reduction of CME from baseline in the OCT as the ‘improvement’ in this study.
For the macular sensitivity measurements, all patients underwent automated static perimetry testing (HFA; Humphrey Instruments, San Leandro, California, USA).16 For this examination, the central 10-2 SITA standard program was used. An appropriate lens correction was made for the test distance. The visual field test was repeated if the test reliability based on the manufacturer's recommendations was not satisfactory (fixation loss >20%; false positive >15%; and/or false negative >33%). The calculation of the mean deviation (MD) value involved averaging the differences between the measured sensitivities and the age-adjusted normal sensitivities (total deviations) at each test point. According to a previous report, the ‘macular sensitivity’ was calculated as the average of the 12 central points, excluding foveal points.16
After baseline measurements were obtained, all patients were instructed to use 1% dorzolamide three times daily in each eye during the follow-up period. Follow-up took place at 1, 3, 6, 12 and 18 months during treatment. All patients were asked to report the development of any subjective visual changes as well as any side effects. BCVAs, slit-lamp biomicroscopy of the anterior segment, intraocular pressure measurements, and funduscopic examination were obtained and/or conducted as performed at baseline. Repeat visual field tests using HFA were obtained in order to minimise the learning effect. OCT measures were also obtained.
Statistical analysis
All values are expressed as the mean±SD. The data were analysed by Wilcoxon signed rank test. N-numbers per group are as indicated. p Values of less than 0.05 were considered to indicate statistical significance.
Results
The clinical data are summarised in table 1. The mean age was 43.0 years (20–60 years), and the patients comprised one man and nine women. Eight patients showed CME in both eyes and two patients showed unilateral CME. No severe side effects were observed in any of the patients during the course of the experiment. Patient #1 showed an initial response and a subsequent rebound of CME after 6 months’ treatment. Therefore, she discontinued topical dorzolamide at 1 year after treatment initiation. We could not collect the HFA data of patient #5 at 18 months after treatment, because the test reliability was not satisfactory despite repeated examinations.
Clinical characteristics of patients with retinitis pigmentosa associated with cystoid macular oedema
On OCT examination, quantitative assessment of retinal thickness (CST) showed an improvement (almost complete resolution of CME or more than 20% reduction from baseline) in 14 (77.8%) of 18 eyes within 6 months. In eight (88.9%) of the nine eyes in which CME was almost completely resolved within 6 months, the therapeutic efficacy persisted for 18 months (figure 1). In addition to one of the nine eyes in which CME was almost completely resolved within 6 months, four (80.0%) of the five eyes that showed an initial response (more than 20% reduction from baseline but not near-complete resolution) within 6 months experienced recurrence of CME (figure 2). Four eyes showed no response (under 20% reduction from baseline) within 6 months. Thus, at the end of the observation period, CME was almost completely resolved in 10 (55.6%) of 18 eyes, and statistically significant improvement of retinal thickness was attained (baseline: 443.5±99.8 μm; after 12 or 18 months’ treatment: 380.5±106.1 μm; table 1 and figure 3; p<0.001).
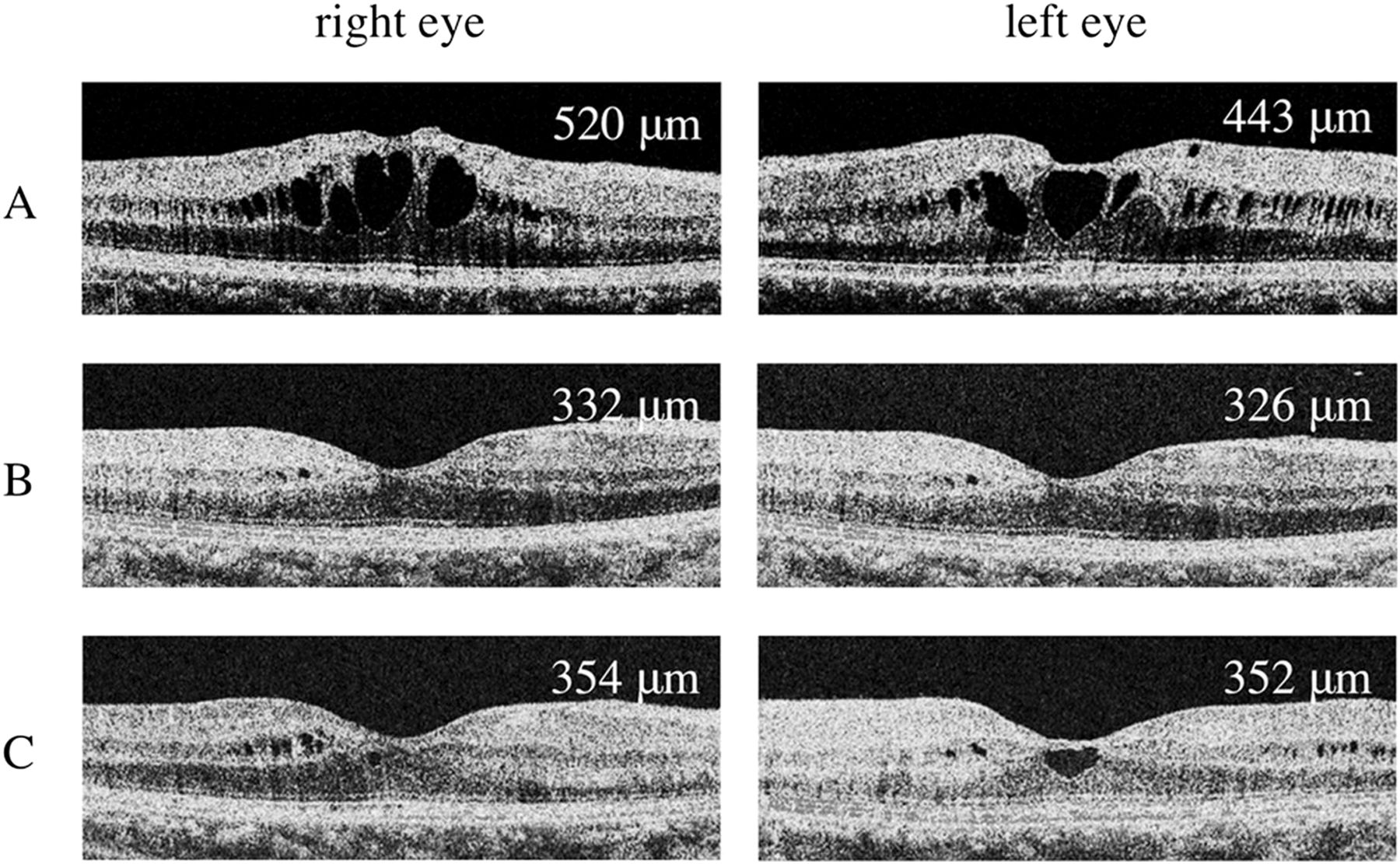
Images of horizontal optical coherence tomography macular scan from patient #2. (A) The baseline scan showed cystoid macular oedema (CME) in both eyes. (B) After 6 months of treatment, CME in both eyes was almost completely resolved. (C) The therapeutic efficacy persisted for 18 months.

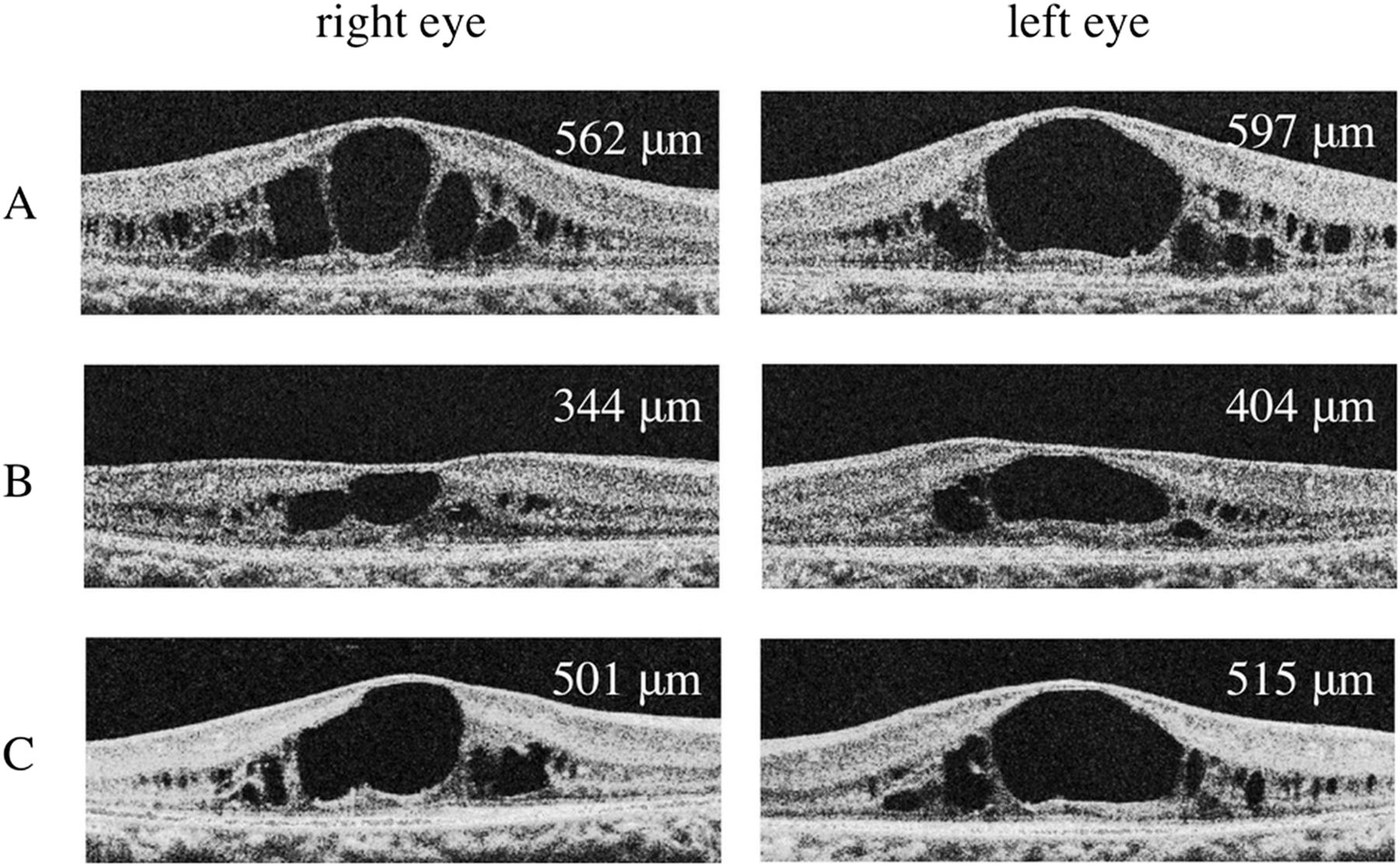
Images of horizontal optical coherence tomography macular scan from patient #7. (A) The baseline scan showed cystoid macular oedema with a dome-shaped foveal profile in both eyes. (B) After 6 months of treatment, both eyes showed a significant decrease in retinal thickness but not near-complete resolution. (C) At the 18-month follow-up, both eyes showed a worsening of retinal thickness compared to that observed at the 6-month follow-up visit.
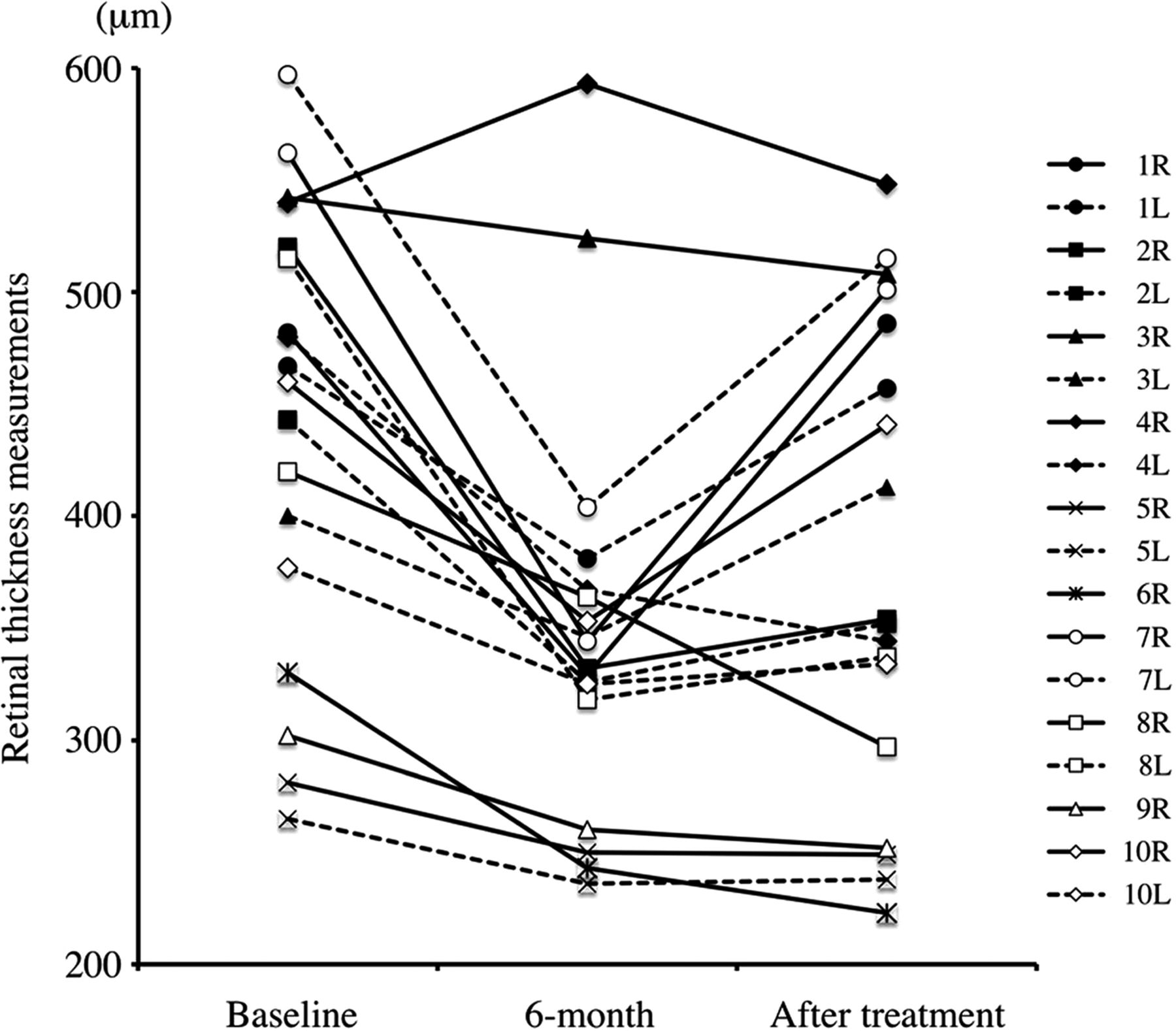
Temporal changes in the retinal thickness (central subfield thickness) on optical coherence tomography. At the end of the observation period, cystoid macular oedema was almost completely resolved in 10 (55.6%) of 18 eyes.
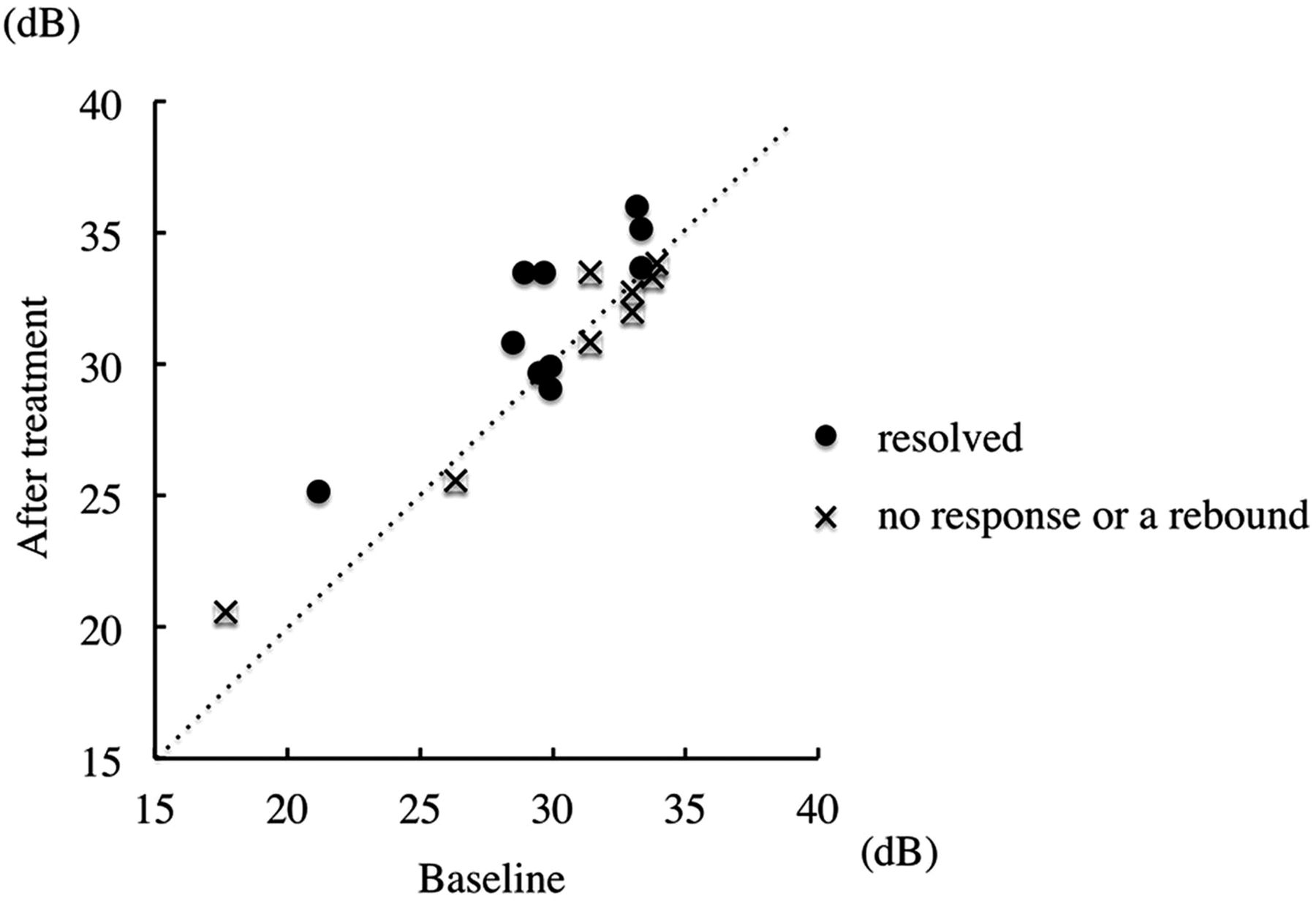
The BCVA, the MD value and the ‘macular sensitivity’ on HFA are summarised in table 1. Despite the reduction in retinal thickness, visual acuity was not significantly improved (p=0.11) and the MD values were variable. However, the ‘macular sensitivity’ in all 10 eyes in which CME was almost completely resolved was significantly improved by the end of the observation period (baseline: 29.7±3.6 dB; after 12 or 18 months’ treatment: 31.7±3.3 dB; figure 4; p<0.05). On the other hand, the ‘macular sensitivity’ in the eight eyes which showed no response or a rebound was not significantly improved (baseline: 30.1±5.6 dB; after 12 or 18 months’ treatment: 30.3±4.8 dB; figure 4; p=0.74).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in the ‘macular sensitivity’ on Humphrey field analyser 10-2 program. The ‘macular sensitivity’ in all 10 eyes in which cystoid macular oedema was almost completely resolved had significantly improved by the end of the experimental period. On the other hand, the ‘macular sensitivity’ in the eight eyes which showed no response or a rebound was not significantly improved.
Discussion
In the present prospective study, we investigated the therapeutic effects of a topical CAI for the management of CME in patients with RP over a 1-year period. We demonstrated the following: (1) on OCT examination, 10 (55.6%) of 18 eyes showed a significant decrease in retinal thickness at the observation period; (2) in eight (88.9%) of the nine eyes in which CME was almost completely resolved within 6 months, the therapeutic efficacy persisted for 18 months; (3) on HFA examination, the ‘macular sensitivity’ in all 10 eyes in which CME was almost completely resolved was significantly improved by the end of the observation period; and (4) no severe side effects developed in any of the patients.
To evaluate the macular function separately from visual acuity, we measured the ‘macular sensitivity’ using HFA in this study. We previously reported that the ‘macular sensitivity’ was increased with a reduction of central macular thickness measured by OCT in RP patients with CME,16 indicating that the ‘macular sensitivity’ is a valid evaluation method. Recently, Iijima demonstrated that not only the MD values but also the average sensitivity of the central 12 points (‘macular sensitivity’) and of the central four points on the HFA10-2 program were correlated with the BCVA converted into logMAR, especially in advanced RP.17 Thus, it is possible that the ‘macular sensitivity’ is a valuable parameter for macular function in patients with RP. In this study, we demonstrated a significant difference in the ‘macular sensitivity’ between eyes in which CME had almost completely resolved and ones in which CME still remained (table 1 and figure 4). As in previous reports,12 ,13 our results showed that the longer than 1-year topical administration of dorzolamide was effective.
We observed that the therapeutic efficacy persisted through 18 months in eight (88.9%) of the nine eyes in which CME was almost completely resolved within 6 months. On the other hand, as shown in figure 2, in four (80.0%) of the five eyes which showed an initial response (more than 20% reduction from baseline but not near-complete resolution) within 6 months, CME returned. Moreover, three of the four eyes that showed no response within 6 months did not respond at all throughout the observation period. Therefore, the effectiveness of topical dorzolamide treatment can be assessed within the first 6 months. If the therapeutic efficacy is not sufficient, the treatment should be supplemented or changed.
The therapeutic rates presented in this study are limited because of the study design (ie, treatment for both eyes of the same patient). In the previous study, however, we demonstrated that therapeutic effects were observed only in the treated eye.16 Moreover, we demonstrated the left–right asymmetric efficacy in four patients (#1, #3, #4, #8) at 6 months after treatment in this study. Although further study of asymmetric treatment is needed, we consider it possible that dorzolamide directly diffuses from the posterior periocular tissue to the posterior retina–choroid.
Alternative treatments of CME associated with RP, such as oral administration of CAI,10 intravitreal triamcinolone,18 ,19 intravitreal anti-VEGF20 and vitrectomy21 are not standard therapy, because of the severe complications. Following oral administration of CAI, severe side effects such as appetite loss, fatigue and the development of kidney stones have been reported.18 ,19 For surgical treatments, there is a slight risk of severe complications, such as infection or bleeding. On the other hand, topical dorzolamide is safer because it has caused no severe complications, both in this study and in the general treatment for patients with glaucoma.
In conclusion, the prolonged (longer than 1 year) use of topical dorzolamide is effective and safe for the treatment of CME in patients with RP. Therefore, we consider topical dorzolamide to be the first choice for treating CME associated with RP. Additional or other treatment will be required for eyes in which CME does not completely resolve within 6 months.
Acknowledgments
KN International provided language assistance.
References
Footnotes
-
Contributors Involved in conception and design of study (YI and TI); analysis and interpretation (YI, NY, SN and YM); writing of the article (YI); critical revision of the article (HE and TI); final approval of the article (YI, NY, SN, YM, TH, HE and TI); and data collection (YI, NY, SN, YM and TH).
-
Funding This work was supported in part by a Grant-in-Aid (to YI and TI) from the Japanese Ministry of Education, Culture, Sports, Science, and Technology (#24659763 and #24659764).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The Institutional Review Board of Kyushu University.
-
Provenance and peer review Not commissioned; externally peer reviewed.