Article Text

Abstract
AIMS/BACKGROUND Thyroid associated ophthalmopathy (TAO) of euthyroid patients is difficult to diagnose because clinical findings overlap with other conditions, and no confirmatory diagnostic tests are available. Recently, it was reported that TSH binding inhibitor immunoglobulin (TBII) and thyroid stimulating antibody (TSAb) are sensitive markers of TAO. The sensitivity of these antibodies in the detection of TAO were therefore studied to determine if they could be a useful criterion in the diagnosis of TAO of euthyroid patients.
METHODS Serum values of TBII and TSAb of 35 patients with euthyroid TAO (group A) were compared with those of 27 patients with Graves’ disease and TAO (group B). The relation between the serum value of TSAb and the eye symptoms of patients with euthyroid TAO were also examined by multiple linear regression analysis.
RESULTS In group A, TBII was positive in 10 cases (28.6%) and TSAb was positive in 29 cases (82.9%). In group B, both TBII and TSAb were positive in all cases (100%). The titre of serum TBII in group A (15.6% (SD 18.0%)) was significantly lower (p<0.0001) than in group B (57.9% (21.5%)). The titre of serum TSAb in group A (1400.9% (2163.9%)) was significantly lower (p=0.0026) than in group B (2243.9% (1472.8%)). Among the eye findings of patients with euthyroid TAO, keratopathy was significantly (p=0.034) related to the value of TSAb.
CONCLUSION These results suggest that the activity of TSAb is a more sensitive marker of euthyroid TAO than is TBII, and could be a useful criterion in the diagnosis of TAO of euthyroid patients.
- thyroid associated ophthalmopathy
- euthyroid
- Graves’ disease
- thyroid stimulating antibody
- thyroid stimulating hormone
Statistics from Altmetric.com
- thyroid associated ophthalmopathy
- euthyroid
- Graves’ disease
- thyroid stimulating antibody
- thyroid stimulating hormone
Thyroid associated ophthalmopathy (TAO) of euthyroid patients was reported decades ago.1 The diagnosis of TAO of euthyroid patients is, however, often difficult because it depends on the clinical examination and lacks objective standards.2-4 The laboratory evaluation of Graves’ disease rests on commonly used tests of thyroid status; serum free T3, T4, and the level of circulatory thyroid stimulating hormone (TSH). The diagnosis does not normally depend on the evaluation of autoantibodies to the TSH receptor. While it is widely accepted that TAO in Graves’ disease is an autoimmune process, the precise mechanism remains conjectural and the search for an ideal test for the diagnosis of TAO continues. Recent immunocytochemical studies suggest that autoantibodies against retrobulbar tissue may play a role in the development of TAO.5 Although TSH binding inhibitor immunoglobulin (TBII) may block thyroid hormone production and thus be related to euthyroid or hypothyroid TAO,6 patients also exist with clinically evident euthyroid TAO in whom TBII is negative. Therefore, a more sensitive autoimmune marker is needed to detect these cases of TAO.7 Thyroid stimulating antibody (TSAb) has been detected in many patients with euthyroid TAO,8 and has potential as an alternative marker for the disease. We studied the sensitivity of TSAb in the detection of euthyroid TAO, and examined the correlation between TSAb activity and ocular findings of patients with euthyroid TAO. We discuss whether TSAb can be a useful adjunct in the diagnosis of euthyroid TAO.
Subjects
We examined 35 consecutive patients with euthyroid TAO (group A), and a control group of 27 patients with Graves’ disease and TAO (group B) between July 1991 and July 1994. Ages ranged from 15 to 65 years (average 47.0 (SD 12.6) years) in group A, and 17 to 64 years (35.6 (14.7) years) in group B. Patients in group A had a male to female ratio of 14 to 21, compared with 6 to 21 in group B. The male to female ratio in group A was not statistically different from that in group B. However, the mean age in group A was significantly higher than that in group B.
The diagnosis of euthyroid TAO of euthyroid patients was made on the basis of clinical signs of TAO in the presence of normal serum free thyroxine (T4) and free triiodothyronine (T3) concentrations without a history of hyperthyroidism. TAO was diagnosed by clinical features of the disease including at least one of the following signs: exophthalmos (Hertel measurement ⩾17 mm; exceeding the upper limit of the normal for healthy Japanese adults9), lid retraction (upper eyelid margin at or above the superior corneoscleral limbus in primary gaze), extraocular muscle dysfunction (restrictive myopathy assessed by Hess chart or objective evidence of enlarged muscles assessed by computed tomography (CT) or magnetic resonance imaging (MRI)), and optic nerve dysfunction (abnormal visual acuity, pupillary reaction, and perimetry not attributable to other causes). Other possible causes for these findings were carefully eliminated by patient history, examination including CT or MRI, and laboratory testing.
The diagnosis of Graves’ disease was established by detection of elevated serum free T4 and free T3 concentrations and decreased TSH concentration before antithyroid drug treatment. Other possible causes of hyperthyroidism, such as thyroid carcinoma, were ruled out by performing thyroid scans.
Methods
Antithyroid thyroglobulin antibody (TGHA) and antithyroid microsomal antibody (MCHA) were measured by haemagglutination assay.10 The TBII was measured by radio receptor assay11 using a commercial kit.12 The result was expressed as a percentage of the normal control value using the following formula:
The TSAb was measured using cultured functional rat thyroid lined (FRTL-5) cells13 by a method reported previously.14 Briefly, polyethylene glycol was reconstituted with hypotonic Hanks’ balanced solution, then added to FRTL-5 cells. For measurement of TSAb, after a 2 hour incubation, cyclic AMP (cAMP) in the medium was measured using a commercially available kit (Yamasa Shouyu, Chiba, Japan). The result was expressed as a percentage of the normal control value using the following formula:
Results were expressed as the mean (SEM). One way layout analysis of variance was used to evaluate differences between the two groups, and the relation between TBII and TSAb was assessed from correlation coefficients (r) determined by linear regression analysis using the method of least mean squares. The difference was considered significant for p <0.05. Multiple linear regression analysis was done to examine the correlation between the activity of TSAb and eye symptoms.
Results
Ocular findings noted in patients with euthyroid TAO included eyelid retraction in 26 cases (74.3%), extraocular muscle dysfunction in 26 cases (74.3%), extraocular muscle swelling (by CT or MRI) in 24 cases (68.6%), eyelid oedema in 23 cases (65.7%), exophthalmos in 20 cases (57.1%), keratopathy in 14 cases (40.0%), and optic neuropathy in three cases (8.6%). Exophthalmos, a typical sign of TAO, was observed less frequently than lid retraction or extraocular muscle dysfunction.
The concentrations of serum free T4 and T3 were normal in all patients in group A, but were elevated in all patients in group B. The serum TSH concentration in group A patients was low in four cases, normal in 30, and high in one. In contrast, the serum TSH concentration was low in all group B patients (Fig 1). The value of TGHA was positive in three patients (8.6%) in group A and in 10 patients (37.0%) in group B. The value of MCHA was positive in six patients (17.1%) in group A and in 20 patients (74.0%) in group B.

Serum value of free T4, T3, and TSH in group A (euthyroid patients with thyroid associated ophthalmopathy) and in group B (patients with Graves’ disease and ophthalmopathy). The shaded area indicates the normal range.
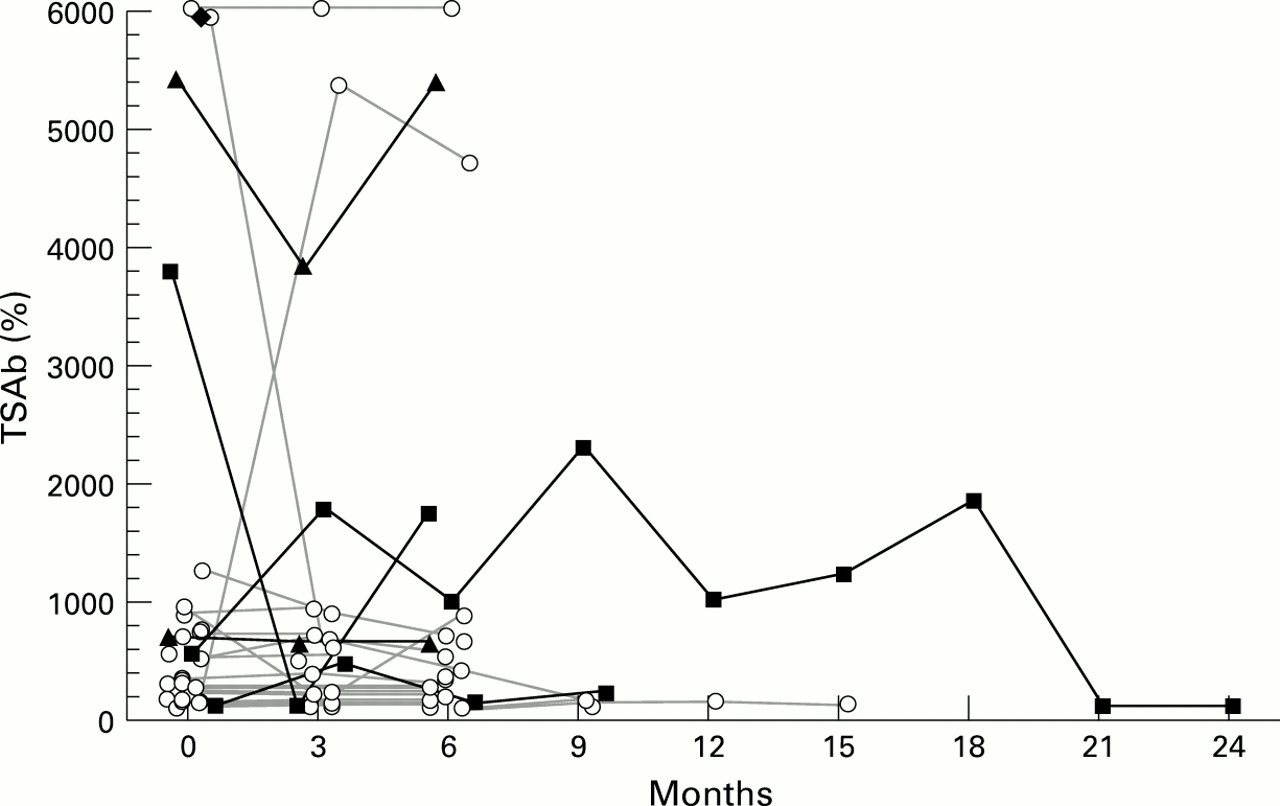
In group A, TBII was positive in 10 cases (28.6%) and TSAb was positive in 29 cases (82.9%). In group B, both TBII and TSAb were positive in all cases (100%). The mean titre of serum TBII in group A (15.6% (18.0%)) was significantly lower (p<0.0001) than that for group B (57.9% (21.5%)). The mean titre of serum TSAb in group A (1400.9% (2163.9%)) was significantly lower (p=0.0026) than that for group B (2243.9% (1472.8%)) (Fig 2). As shown in Figure 3, there was a significant correlation between the mean value of TBII and TSAb (r=0.341, p=0.0063) when both groups A and B were combined. The TSAb titre was markedly elevated in seven patients in group A (>5000%). One of these patient became hyperthyroid, two patients developed Hashimoto’s disease, one patient was later diagnosed with adenocarcinoma of the thyroid, and three patients remained euthyroid (Fig 4). Multiple linear regression analysis revealed that the activity of TSAb was significantly (p=0.034) related to keratopathy, but not to other ocular findings.

Serum value of TBII and TSAb in groups A and B. The shaded area indicates the normal range.

Relation between serum value of TSAb and TBII in both groups. The linear regression analysis has been done on the combined data from group A and B.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in serum value of TSAb in group A. The follow up period was from 6 to 21 months. (○ euthyroid throughout the follow up period, •, became hyperthyroid, ▴, developed Hashimoto’s disease, ♦, adenocarcinoma of thyroid was diagnosed.)
Discussion
Thyroid associated ophthalmopathy is generally considered an organ specific autoimmune disease which causes proliferation of fibroblasts in the retrobulbar tissue, and swelling of the extraocular muscles.16 TSH receptor antibody (TRAb) is a generic term that includes TBII and TSAb, which both bind to the TSH binding site. TSAb is an antibody that mimics the action of TSH in that both stimulate thyroid hormone production. TBII binds to the TSH receptor and inhibits the binding of TSH.
TRAb has been linked to the pathogenesis of autoimmune thyroid disease, and has also been implicated as causative in TAO.1718TSH receptor specific mRNA and TSH binding sites have been identified in the orbital tissue of patients with TAO,519suggesting that orbital tissue can be a target of TRAb.
Current assays for TRAb measure their ability either to compete with TSH for binding (TBII) or to stimulate cAMP production (TSAb). TBII and TSAb have been detected in patients with TAO820 despite the presence of normal serum concentrations of free T3 and free T4, and normal values of TSH. Which of these factors has a greater role in the genesis of TAO of euthyroid patients is not known. Some studies have shown a correlation between the activity of TBII and TSAb,820 but others have failed to show this relation.21-23
In the current study, the activity of TBII showed a good correlation with that of TSAb (Fig 3). We also found elevated levels of TSAb in the majority of patients with euthyroid TAO (82.9%). On average, TSAb levels were lower in patients with euthyroid TAO than patients with Graves’ disease and TAO (Fig 2), but some patients with euthyroid TAO had very high levels of TSAb (>5000%). Indeed, TSAb levels divided patients with euthyroid TAO into two groups, those with ‘moderate’ serum elevations (22 patients) and a smaller group with extremely high levels (seven patients). Of these seven patients, one went on to develop manifest Graves’ disease, two developed Hashimoto’s thyroiditis, and one was found to have adenocarcinoma (Fig 4). Excluding these atypical cases with extreme elevations of TSAb, patients with euthyroid TAO seem to have a milder systemic immunological disturbance than patients with Graves’ disease and TAO. This may be related to the presumed limited area of involvement by disease in patients with euthyroid TAO. We found a much lower detection rate of abnormal TBII values (28.6%) than for TSAb (82.9%) (Fig 2). This suggests that TSAb is a much more sensitive marker for euthyroid TAO than TBII.
Antithyroid thyroglobulin antibody was detected in 8.6% of patients with euthyroid TAO and antithyroid microsomal antibody was detected in 17.1% of them. Therefore, these two autoantibodies are also not effective in detecting euthyroid TAO.
As noted above, four of seven patients with euthyroid TAO with markedly elevated levels of TSAb were found to develop other conditions, including Graves’ disease, Hashimoto’s thyroiditis, and adenocarcinoma. Therefore, it is important for the treating ophthalmologist to arrange careful medical follow up for such patients. Conversely, in some patients with euthyroid TAO, TSAb was negative. Some of these ‘false negative patients’ did not have exophthalmos or lid retraction on examination, and the diagnosis of TAO was based on muscle dysfunction and goitre of the thyroid gland. Symptoms did not progress in these patients suggesting that muscle restriction was due to chronic fibrotic changes, and that disease activity was low. Such ‘burnt out’ cases may be one situation in which TSAb is not a useful marker. The other patients with negative TSAb had exophthalmos and lid retraction, but generally to a mild degree. On repeat testing, TSAb became positive in four patients, all with initially mild disease. Therefore, it may be advisable to check TSAb levels several times, as some false negatives may represent very early disease.
Multiple linear regression analysis revealed that the activity of TSAb was significantly related to keratopathy. Keratopathy can be caused by several mechanisms; exposure keratopathy due to increased orbital volume, entropion due to retraction of the lower lid, or superior limbic keratoconjunctivitis related to the increased friction between the upper lid and superior limbus. Since keratopathy is more likely to occur by any of these means as they become more severe, keratopathy may reflect the activity and severity of the disease process better than any other single findings. The activity of TSAb may also reflect the severity of TAO, and we would therefore expect the two to be related.
The current study was not intended to determine the pathogenesis of euthyroid TAO. However, the fact that TSAb was detected in the majority of these patients suggests that it may be a sensitive marker for patients with euthyroid TAO. Future studies including larger numbers of patients will help to better elucidate the relation between TSAb, TBII, and TAO of euthyroid patients.
Acknowledgments
We appreciate the help of Dr Amino and Dr Kashiwai in the Department of Laboratory Medicine, Osaka University Medical School, for the measurement of TSAb.