Article Text

Abstract
AIMS Micromorphological examination of the central cornea in myopic patients 8–43 months after excimer laser photorefractive keratectomy (PRK), using the slit scanning confocal microscope.
METHODS Patients were selected from a larger cohort of individuals on the basis of full corneal clarity (haze grading 0 to +1; mean 0.3) and their willingness to participate in the study. 15 eyes of 10 patients with myopic PRK (−4 to −11 D; mean 6.7) and an uneventful postoperative interval of 8–43 months (mean 26) were examined. Contact lenses had been worn by eight of the 10 patients for 4–11 years (mean 6.7) before surgery. Controls included the five untreated fellow eyes of PRK patients, 10 healthy, age matched volunteers without a history of ocular inflammation or contact lens wear, and 20 patients who had worn rigid gas permeable (n=10) or soft contact lenses (n=10) for 2–11 years. Subjects were examined with a real time flying slit, scanning confocal microscope using ×25 and ×50 objectives.
RESULTS In PRK treated patients and contact lens wearers, basal layer epithelial cells sporadically displayed enhanced reflectivity. The subepithelial nerve plexus was observed in all individuals, but was usually less well contrasted in the PRK group, owing to the presence of a very discrete layer of subepithelial scar tissue, which patchily enhanced background reflectivity. Within all layers of the stroma, two distinct types of abnormal reflective bodies were observed in all PRK treated eyes, but in none of the controls. One had the appearance of long (>= 50 μm), slender (2–8 μm in diameter) dimly reflective rods, which sometimes contained bright, punctate, crystal-like inclusions, arranged linearly and at irregular intervals. The other was shorter (<25 μm), more slender in form (<1 μm in diameter), and highly reflective; these so called needles were composed of crystal-like granules in linear array, with an individual appearance similar to the bright punctate inclusions seen in rods, but densely packed. Both of these unusual structures were confined, laterally, to the ablated area, but were otherwise distributed throughout all stromal layers, with a clear predominance in the anterior ones. These rods and needles were observed in all PRK treated corneas, irrespective of previous contact lens wear. On the basis of qualitative inspection, the incidence of rods and needles did not appear to correlate with either the volume of tissue ablated or the length of the postoperative interval. In contact lens wearing controls, highly reflective granules, reminiscent of those from which the needles were composed, were found scattered as isolated entities throughout the entire depth and lateral extent of the corneal stroma, but rods and needles were never encountered. The corneal endothelium exhibited no obvious abnormalities.
CONCLUSION Confocal microscopy 8–43 months after PRK revealed belated changes in the corneal stroma. These were manifested as two distinct types of abnormal reflective bodies, which had persisted beyond the stage when acute wound healing would have been expected to be complete. The clinical significance of these findings in the context of contrast visual acuity and long term status of the cornea is, as yet, unknown.
- photorefractive keratectomy
- excimer laser
- confocal microscopy
- stromal pathology
Statistics from Altmetric.com
In recent years, the excimer laser has gained considerable acceptance as a means of effecting corneal ablation in refractive surgery.1-4 With its narrow emission band of ultraviolet radiation, ablation and hence reshaping of the central cornea with this instrument can be expected to attain a high degree of precision. And, in clinical terms, this has proved to be the case.5 To date, several tens of thousands of patients worldwide have received excimer laser photorefractive keratectomy (PRK) for myopic correction. Albeit, some concern has been expressed regarding the mutagenic potential of this ultraviolet radiation source and the possibility of its inducing other, as yet unknown, long term damage.6-8Furthermore, postoperative enhancement of stromal keratocyte activity beneath the ablation zone may lead to transient haze, a frequent consequence of PRK. Although this manifestation may be only transient, it is none the less disturbing, since it is located within the visual axis; as such, it represents a major disadvantage of the technique. Persistent haze, on the other hand, usually reflects the subepithelial deposition of scar tissue—a wound healing response. The severity of this latter condition appears to be a function of excision dimensions (including depth), the duration over which the epithelial defect persists, and, questionably, postoperative steroid treatment.9-12
Histological data pertaining to wound healing after PRK have been gleaned principally from experiments with rabbits or other experimental animals, and these may not be pertinent to the human situation in all respects. Morphological observations bearing on the late corneal response in uncomplicated human PRK cases have not been reported thus far.
The advent of in vivo confocal microscopy has furnished us with the means of improving imaging in the living cornea.13-16This facility has been used to study wound healing in rabbits after PRK, thereby revealing stromal changes in the ablated area17 including the presence of activated keratocytes and some subepithelial scarring.18 Recent observations in human PRK patients have linked the development of clinical haze to the existence of “subepithelial deposits”,19 which regress during the first 6 months after surgery. Another study using tandem scanning confocal microscopy has revealed a correlation between clinical haze and anterior stroma reflectivity.20
In the present study, we report on observations made in a group of PRK patients with perfectly clear corneas, several years after surgery, using an in vivo confocal microscope with on line imaging and improved optical resolution.
Subjects, materials, and methods
SUBJECTS
From a cohort of PRK patients previously reported on,21 10 men (28–48 years of age) were willing to participate in this study, at a mean time of 26 months (range 8–43) after surgery (Table 1). Selection criteria included a clear cornea, as viewed with the slit lamp, and a haze grading between “0” (none) and “+” (trace) (mean 0.3; range 0–1), as revealed upon oblique illumination. Among these 10 patients, 15 eyes had been treated for a myopic correction with a mean of 6.7 dioptres (range 4.0–11.0); one had undergone a second PRK, and one an additional astigmatic keratotomy 2 and 24 months, respectively, before the present evaluation. Eight of the 10 patients had a history of contact lens wear spanning a period of 3–11 years. Uncorrected visual acuity (UCVA) in the 15 PRK treated eyes was less than 10/20 in two cases and equal to or better than 10/20 in the other 13. Best spectacle corrected visual acuity (BCVA) was 16/20 in one eye and equal to or better than 20/20 in the other 14. Biomicroscopic examination revealed no signs of pathology in any of the eyes. In the five patients who had received unilateral PRK, the fellow eye served as a control. Additional control groups included:
Data pertaining to the 15 eyes of 10 PRK patients
(i) 10 age matched subjects with normal slit lamp findings and no history of contact lens wear or ocular disease
(ii) 10 myopic patients who had worn rigid gas permeable contact lenses for 3–10 years
(iii) 10 myopic patients with a 2–11 year history of soft contact lens wear.
INSTRUMENT
The instrument employed in this study was a custom built, real time, flying slit, scanning confocal microscope, described in detail elsewhere.14-16 The major advantage of this instrument that it embodies a scanning slit rather than the pinholes of a Nipkov disc. With its high throughput of light and truly real time video display, further image sampling or processing is not required. For in vivo imaging of the cornea, the microscope objective was positioned 1.5–1.0 mm in front of the patient’s eye, and brought into optical contact with the latter via the medium of a viscous acrylic ocular gel (Lacrinorm, Novopharma, Switzerland). Optical en face sections of the cornea were obtained in real time for all corneal layers and were recorded on a S-VHS videotape. The position of the optical plane in the Z axis was controlled by a manual micrometre drive; Bowman’s layer and the corneal endothelium also served as reference structures for the Z axis position.
Water immersion microscope lenses, ×25 (NA 0.65) and ×50 (NA 1.0) (Leitz, Germany), were used, the calculated lateral resolution of the former being 1.4 μm and that of the latter at least 0.8 μm; optical section thickness obtainable in each case were calculated to be 16 μm and 10 μm, respectively. Lens surface diameters were 5 mm and 4 mm for the 25× and 50× objectives, respectively.
The projected confocal slit width was 10 μm, at which setting an optimal balance between resolution, illumination intensity, and contrast was achieved. The slit scanning frequency was 12.5 Hz, thereby yielding 25 video frames per second. Under these conditions, exposure time for a given point in the focal plane was 0.7 ms. Since the slit scan is synchronised with the video chip read out, more than 95% of the collected images were without motion blur or image distortion (both of which could be easily identified when extant).
For a detailed analysis, the recorded video sequences were reviewed in single frames on a high quality monitor. A printout for the patient’s file was made using the video printer. Images presented in this report were digitised from the videotape and then exposed to photographic film.
For each eye/objective combination, minimally 1500 sharp video frames, obtained during a recording time of 1–3 minutes (depending on patient cooperation and image quality), by a single investigator (MB), were reviewed. At least two thirds of these displayed information pertaining to stromal layers; the remainder yielded details of the epithelium and endothelium.
METHODS
Before confocal microscopy of the cornea, patients were informed as to the purpose of, and (remote) potential risks associated with, the scanning procedure.
After conjunctival instillation of topical 0.4% Novesine, and positioning of the patient’s head on an adjustable support, the ×50 objective was centred over the apex of the cornea. The patient was requested to focus his gaze on the light, the centre of the cornea being thereby positioned with a lateral accuracy of about 1 mm. One drop of eye gel was applied to the microscope lens, which was then brought into optical contact with, but not pressed upon, the cornea. Repeated manual imaging was then undertaken at the centre of the tissue (in all individuals) and at its temporal periphery (in all PRK patients and contact lens wearers), approximately 5 seconds being required for each scan. The entire procedure was then repeated using the ×25 objective. In a given scan series, ablated zones could be readily identified by the absence of Bowman’s layer.
Video sequences were reviewed (at least twice) and evaluated according to a standardised protocol, in a non-masked fashion, by a single observer (MB). Images were assigned to one of the following locations:
- (1)
epithelium (including surface, intermediate, and basal cells)
- (2)
subepithelial nerve plexus
- (3)
most anterior keratocyte layers (contained within the 2–5 video frames collected after passage through the epithelium)
- (4)
anterior stroma (initial 100 μm)
- (5)
mid stroma (spanning a focal depth of 150–400 μm)
- (6)
posterior stroma (final 100 μm)
- (7)
most posterior keratocytes (contained within the final 1–3 layers of stromal tissue, immediately above Descemet’s membrane)
- (8)
endothelium.
Observations pertaining to such variables as subepithelial nerve plexus visibility, subepithelial scarring, and stromal abnormalities were classified merely according to absence or presence of the respective phenomenon.
Results
Each corneal layer was visualised with clarity (high contrast and resolution) in all eyes examined. A discrete, punctate keratopathy was observed in all subjects at the end of the scanning procedure, but no discomfort was experienced, and neither corneal erosions nor other sequelae were manifested.
EPITHELIUM
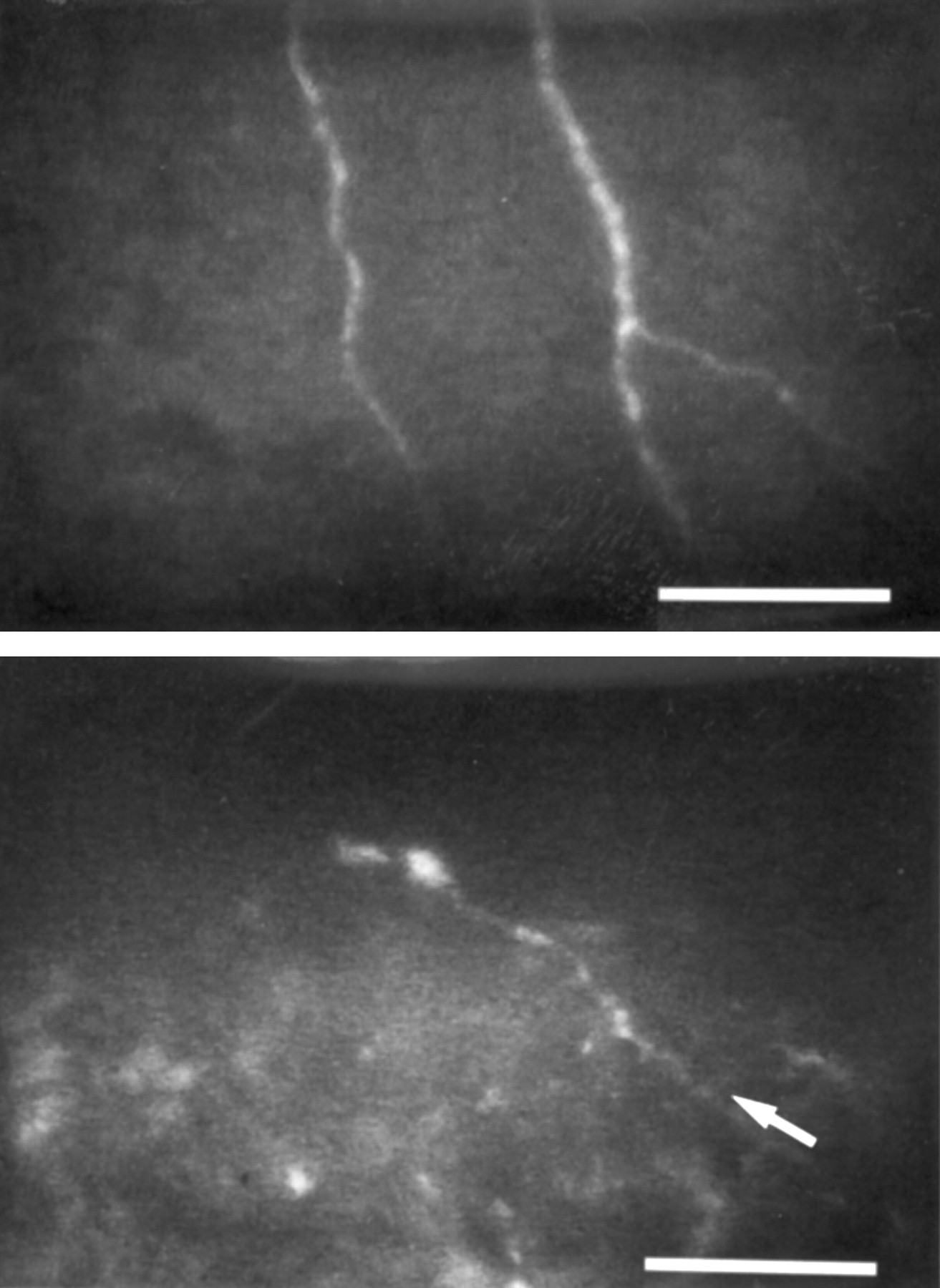
Non-reflective cells comprising the basal epithelial layer were clearly demarcated from one another by their dimly reflective borders, in all eyes examined. In each of the PRK treated ones, entire cells occasionally appeared highly reflective (Fig 1); these were distributed randomly as isolated entities, and were found not only within the ablated zone, but also in the unoperated more peripheral cornea. In 10 of the 15 PRK treated eyes, such reflective cells (but of larger size) were sometimes observed also within the basal to intermediate epithelial layers. These manifestations were not encountered in normal controls, but both were sporadically observed in contact lens wearing ones.

Basal layer of corneal epithelium. Top: normal control eye, depicting non-reflective cells delimited by dimly reflective borders. Bottom: PRK patient 1 year after surgery, illustrating the scattered occurrence of individual cells with increased reflectivity (arrows), a phenomenon which may be indicative of mitotic cell division. ×50 objective; bar= 50 μm.
SUBEPITHELIAL NERVE PLEXUS
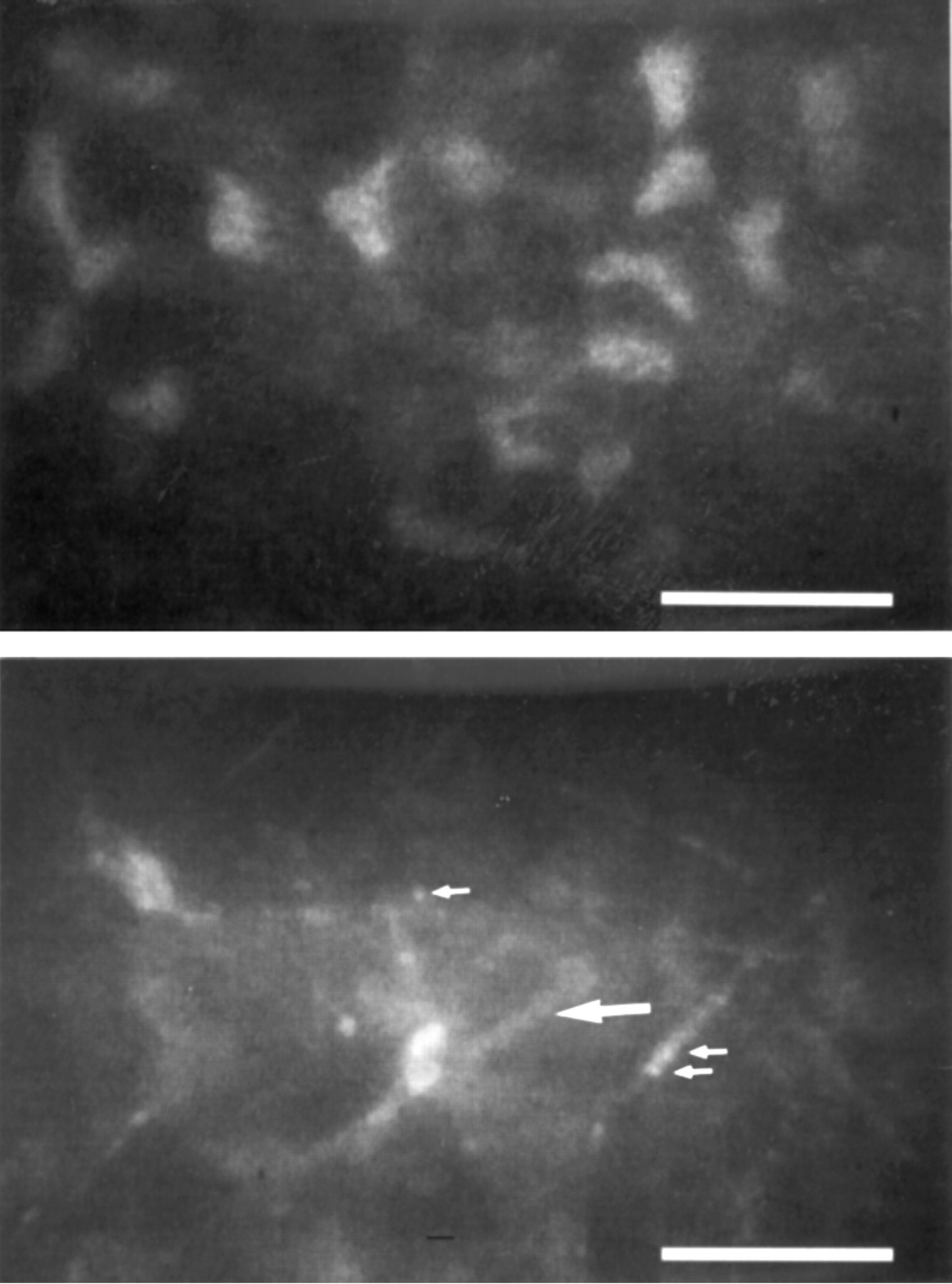
The subepithelial nerve plexus was observed in all eyes examined (Fig 2, top). In normal eyes, it was well contrasted against the non-reflective (dark) Bowman’s layer. In PRK treated ones, it was poorly contrasted (Fig 2, bottom), owing to the absence of Bowman’s layer and to the presence of a very discrete subepithelial layer of scar tissue. The latter was manifested as irregularly shaped patches of material with increased reflectivity, which occasionally even masked completely the subepithelial nerve plexus. Such discrete scarring, which was visible only in the confocal microscope, occurred to a variable, though always low, degree in all PRK treated eyes, albeit that each had a clinical haze score between “0” and “1”. In contrast with the regular branching pattern exhibited by the subepithelial nerve plexus in controls, that manifested in PRK treated eyes was more bizarre.
Subepithelial nerve plexus. Top: normal control eye, depicting beaded nerve fibres enhanced by an optically unstructured, and hence non-reflective, Bowman’s layer. Bottom: PRK patient 1 year after surgery. This subepithelial nerve fibre (arrow) is less well contrasted than those in controls owing to the presence of a discrete layer of scar tissue, which increases background reflectivity. ×50 objective; bar=50 μm.
STROMA
Distribution pattern of reflective keratocyte nuclei
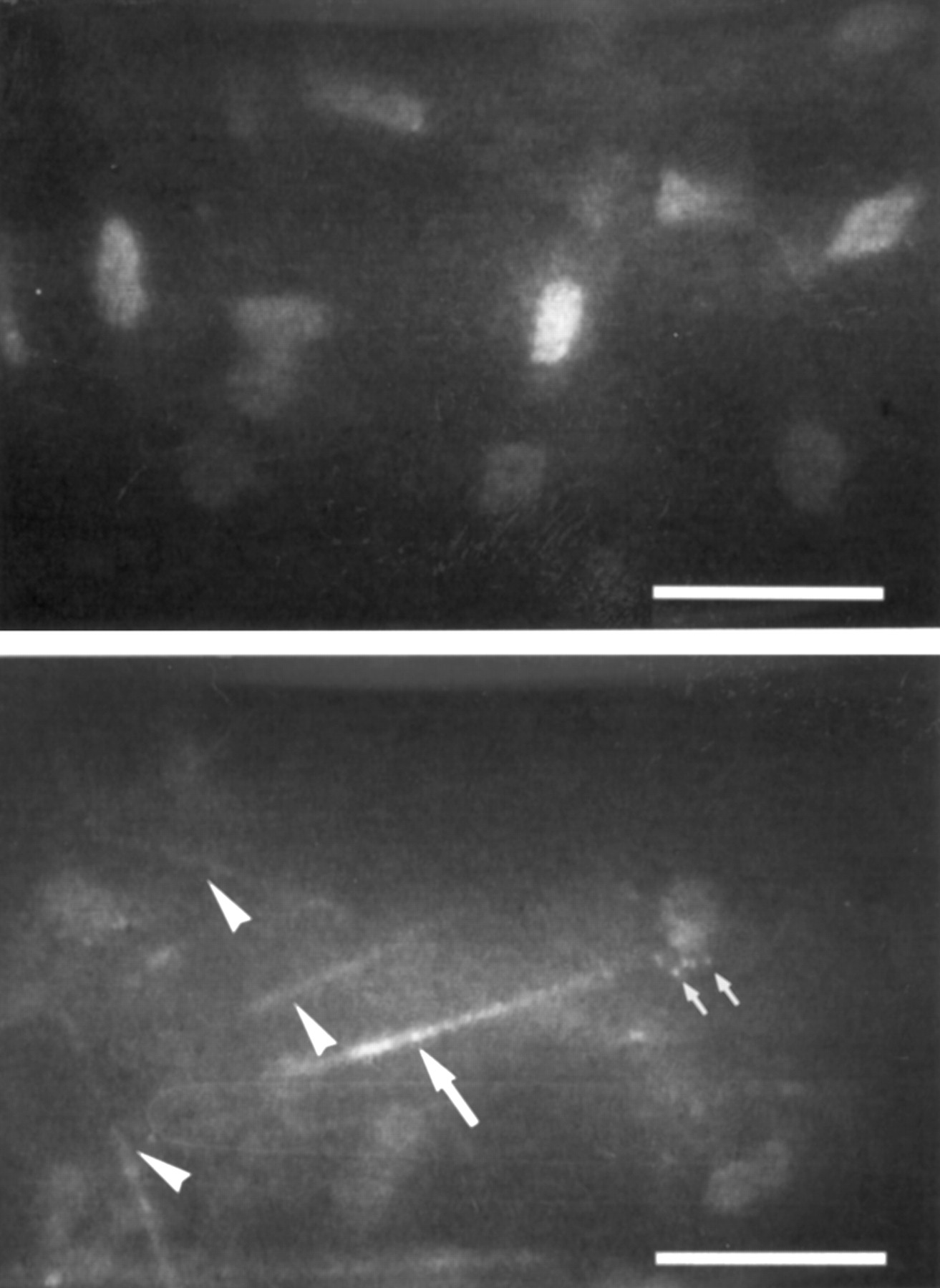
In control eyes, reflective keratocyte nuclei within the most anterior (subepithelial) stromal layer exhibited the polygonal shape characteristic of this zone (Fig 3, top), and these were regularly spaced. In PRK treated ones, keratocyte nuclei in the corresponding position were more oval in form and less regularly arranged (Fig 3, bottom). This finding was perhaps not surprising given that these keratocytes had assumed this pseudoanterior position only by virtue of the truly anterior ones having been ablated; hence their similarity in form to the oval or rhomboid typically found within the more distal anterior and mid stromal layers of all eyes (Figs 4, 5, 6). In posterior (deep) layers of the stroma, keratocyte nuclei were oval to elongated in shape, irrespective of eye group.
Keratocyte nuclei in the most anterior stromal layer. Top: normal control eye. Keratocyte nuclei manifest a characteristic polygonal shape; they are regularly spaced. Bottom: PRK patient 2 years after surgery. The most anteriorly located keratocytes have assumed this pseudoanterior position owing to ablation of the superficial stroma. Cell nuclei are partially masked by the subepithelial scar tissue which increases background reflectivity. Dimly reflective rods (arrow), approximately 2–8 μm in diameter and >50 μm in length are visible (large arrow), some of which contain highly reflective punctate inclusions (small arrows). ×50 objective; bar=50 μm.
Abnormal reflective bodies
Within the corneal stroma of control eyes, only keratocyte nuclei (Fig 3, top) and nerve fibres were reflective, these being well contrasted against a dark background. In the stroma of contact lens wearers, highly reflective solitary microdots were observed (Fig 4top), as previously described.22 In PRK treated eyes, the images manifested were much more complex, and a number of other reflective structures were additionally observed. These were of two basic types (see below), both of which had a slender, linear form and were oriented parallel to the longitudinal axes of corneal collagen fibres. They were encountered within all stromal layers, but were most abundant in the anterior (seen in 15/15 PRK treated eyes) and least so in the posterior ones (seen in 9/15 PRK treated eyes); laterally, they were restricted to the ablated area. Since the edges of the ablated zone could not be clearly defined in the non-fixed patients’ eyes, the peripheral unablated cornea was examined instead. Here, the abnormal linear structures were only rarely encountered, whereas the microdots observed in the contact lens wearers occurred in all stromal layers and at all locations.

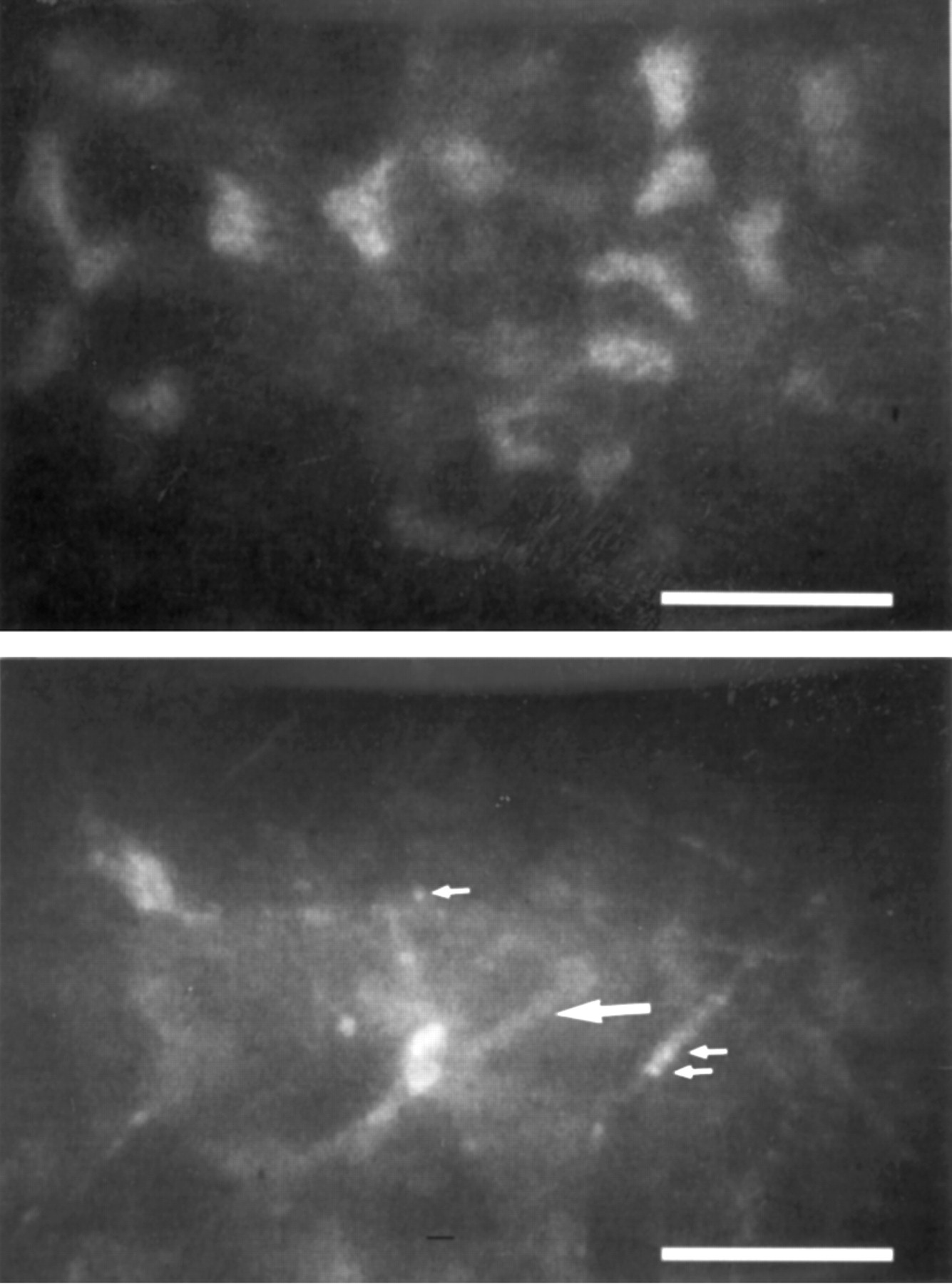
Mid stroma (about 250 μm below the basal epithelial cell layer). Top: control cornea from a patient with an 8 year history of soft contact lens wear. Note the presence of scattered highly reflective spots (arrows) less than 1 μm in diameter. Bottom: PRK patient with a 7 year history of soft contact lens wear, 1 year after surgery. The distribution pattern of keratocyte nuclei appears normal. This micrograph illustrates dimly reflective rods (small arrow) with brilliant, punctate inclusions, and a group of highly reflective needles composed of linearly arranged, densely packed granules (large arrow). ×50 objective; bar=50 μm.
(i) Rods—The most frequently observed of these reflective bodies had a rod-like form, with diameters ranging from 2 μm to 8 μm (Figs 3, 4, 5, 6), and with lengths of 50 μm minimally. They always appeared perfectly straight, were oriented parallel to the surface, and were of similar dimension in all corneal layers; hence, they could not be confused with stromal nerve fibres, which followed a different course and were, moreover, frequently branched. Bright punctate inclusions were sometimes observed to occur at irregular intervals along the length of these rods (Fig 3, bottom; Fig 4, bottom; Fig 5, top; Fig 6, bottom).

Anterior to mid stroma. Top: anterior to mid stroma (about 150 μm beneath the basal epithelial cell layer), 2 years after PRK. The broad, long, and tapering body running diagonally across the centre of the picture (large arrow) is probably a cell process classified as a dimly reflective rod, which contains highly reflective granules (small arrows). Bottom: mid stroma (about 200 μm beneath the basal epithelial cell layer), 1 year after PRK, illustrating rods (arrowhead) and needles (arrow) oriented predominantly parallel to the corneal surface. ×50 objective; bar=50 μm.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Posterior stroma (less than 50 μm above Descemet’s membrane). Top: normal control eye, illustrating the oval or rhomboid form of nuclei characteristic of keratocytes within this layer. Bottom: PRK patient 2 years after surgery, illustrating dimly reflective rods some with bright, punctate inclusions (arrowheads), and a needle (large arrow). Some punctate inclusions in association with a keratocyte nucleus are also visible (small arrows). ×50 objective; bar=50 μm.
Rods were never encountered in any of the 65 control eyes.
(ii) Needles
The second type of reflective body appeared as brilliant shaft-like structures approximately 1 μm in diameter and usually no longer than about 25 μm (Fig 4; and Fig 6, bottom). Owing to their high reflectivity these needles probably appeared larger than they were in actuality. They were observed less frequently than rods, but were more obvious, owing to their highly reflective nature; when videotapes were run in slow motion, they appeared as glistening flashes. With the ×25 objective, needles were resolved in only 9/15 PRK treated eyes, but with the ×50 lens, they were seen in all 15 cases. In many instances these needles appeared as continuous structures, but in others, they were seen to be composed of closely packed, linearly arranged, minute granules, which were not always embraced by a structure of lower reflectivity. In contact lens wearing PRK patients, these crystal-like granular components were sometimes encountered individually in the vicinity of keratocyte nuclei (Fig 6, bottom). The solitary granules, but not the rods or needles, were also observed in soft contact lens wearing controls22 with a history of daily wear extending over a period of more than 6 years (Fig4, top). In these instances, they were homogeneously distributed among all stromal layers and across the entire lateral extent of the cornea. The needles observed in PRK treated eyes were encountered in all stromal layers, but they were not homogeneously distributed (highest incidence in anterior regions); laterally, they were restricted to the ablated area.
Reflective bodies intermediate in form were occasionally observed; this finding suggests the existence of a structural relation between the two entities.
Needles were encountered in none of the 65 control corneas.
ENDOTHELIUM
In all PRK treated eyes and their fellow controls, the corneal endothelium appeared normal, with some irregularities in cell form (which were not further quantified). Endothelial cell counts (per mm2) in the 15 PRK treated eyes and the five fellow controls were 2290 (range 1680–2960) and 2223 (range 1750–2250), respectively. Such counts were not determined in the other control groups, but qualitative inspection revealed no signs of abnormality. Rods, needles, or microdots were not observed within the endothelium of any of the eyes. But in some PRK patients and controls small, highly reflective granules were occasionally encountered intracellularly (not illustrated). Inspection with the slit lamp revealed these to be pigment granule inclusions, the presence of which bore no relation to PRK treatment or contact lens wear.
Discussion
Our investigation demonstrates that PRK elicits possibly late manifested, but in any case persisting, changes in the microstructure of the human corneal stroma. These findings must necessarily be viewed within the broader scope of the wound healing response to refractive surgery, in general, since all procedures currently adopted influence the anatomy, physiology, and mechanical stability of the cornea, not to mention the refractive result.23-25 Although available data are gleaned from a fairly limited repertoire of experimental and clinical studies, this wound healing variable must needs be an important determinant guiding the surgeon’s choice of procedure.
With respect to efficacy, safety, and predictability PRK has many points in its favour, not least among which must be counted the very low anatomical and visual complication rates over a broad spectrum of myopic corrections.26-28 Loss of best corrected visual acuity after PRK has been attributed to decentration of, or irregularities within, optical zones, and to subepithelial scarring.29 Epithelial changes precipitated by PRK have been found to be significant during the early postoperative phase, but these are believed to resolve with time.30 And the corneal endothelium, in particular, manifests no obvious signs of chronic damage.31 Given these assets, it is therefore not surprising that PRK is being increasingly adopted as the method of choice for the surgical correction of low to medium myopia.
With respect to subepithelial scarring, the situation may be far more complex than was hitherto supposed. Short term clinical and histopathological studies involving PRK treated animals and humans have shown disorganised arrays of subepithelial collagen fibrils, activated keratocytes, and the expression of fetal antigens.32-38
Data pertaining to the long term histological changes in human corneas after PRK are scant, and restricted to cases complicated by significant scarring during the postoperative course. Material derived from uncomplicated cases with full vision and no haze has not been forthcoming for histological analysis.
The confocal microscope furnishes us with an invaluable tool for observing the living cornea in PRK treated patients, and thereby with an opportunity for assessing the wound healing response. Several short term studies have already been undertaken in PRK treated rabbits. These revealed an acute loss of keratocytes from the anterior stromal layers, which were replaced by cells resembling fibroblasts in appearance; an accumulation of extracellular matrix material, presumed to be fibrillar in nature, was also reported.32 The overall consequence of these changes was an increase in reflectivity.39 40 In humans, tandem scanning confocal microscopy has been employed for the inspection of corneas up to 1 year after PRK.19 20 These studies revealed that the haze visible upon examination with the slit lamp was correlated with the existence of subepithelial deposits, which possibly consisted of diffusely reflecting scar tissue. At the early stage (1 month), condensed keratocyte nuclei and cell processes were occasionally observed within the stroma, but details respecting pathological changes at the cellular or subcellular level were not furnished in either of these two reports.
In a recent study33 we reported on the presence of abnormal reflective bodies within the corneal stroma of four myopic patients, 1–3 years after unilateral myopic PRK, as observed with real time slit scanning confocal microscopy. In the present investigation, these manifestations designated as rods and needles were detected in all 15 PRK eyes 8–43 months after surgery. In addition to these structures, highly reflective microdots were also observed in PRK patients with a history of soft contact lens wear, as well as in contact lens wearing controls (see also Böhnke and Masters22); but rods and needles were never encountered within this latter group.
Since the manifestations of these phenomena occurred in response to the phototoxic and inflammatory challenge of PRK, they may bear a relation to lipofuscin deposits built up more gradually in response to less overt stimuli during the passage of years.34 Studies are currently under way to simulate these changes in the rabbit model and also to identify the chemical nature of the reflective bodies.
Given that animal and human corneal tissue has been previously examined with the confocal microscope after PRK, there must be a reason why these rods and needles have not been observed before. One explanation may lie in our instrument’s having a higher contrast and resolution potential than those generally available at the time of these earlier investigations; and the mode of collecting real time images, without any manipulation during processing, may also greatly improve the visibility of minute and unexpected structures. Indeed, even with our instrument needles were consistently observed only when using the ×50 objective. An additional factor facilitating visualisation of the reflective structures described in this report may have lain in the criteria adopted for selecting patients: only those with zero to minimal haze were included. Haze reduces contrast by scattering light, and this increases background reflectivity in the confocal microscope. Structures located posterior to corneal haze emit a considerably attenuated signal, thereby diminishing the likelihood of distinguishing small, reflective, stromal bodies. That our background reflectivity was indeed low is well exemplified by our having been able to distinguish subepithelial nerve fibres in all PRK treated patients; these were not always resolved with the confocal microscope in earlier studies.18-20
Another possibility is that the rods and needles are first manifested only some months after surgery; not during the immediate postoperative phase. Moreover, the presence of these structures in histological preparations may have been previously overlooked. Corneal tissue utilised for such purposes is usually cut in a sagittal plane; in such sections, rods and needles would be seen as minute punctate entities, easily mistaken for artefacts and not further accounted for. They would be readily apparent only in sections cut parallel to the corneal surface.
Some patients included in our study had required a fairly high myopic correction and hence a rather high dose of ultraviolet radiation, which may have elicited an unusually strong stromal reaction. However, since we have as yet no means of quantifying rods and needles, it was not possible to ascertain whether there was indeed an association between these structures and the amount of tissue ablated.
Neither rods nor needles bore any resemblance to the reflectivity pattern manifested by rabbit fibroblast processes after PRK,18 32 which were broader, longer, and tapering in form. It may be speculated that the dimly reflective rods represent the processes of keratocytes which have undergone some chronic change during corneal wound healing, whereby their light scattering properties are enhanced. Such a modification could be attributable to an augmented synthetic activity, which would indicate that stromal wound healing is unremitting even up to the time when our observations were made (3½ years).
The highly reflective, crystal-like granules encountered sporadically within these rods could well be lipofuscin pigment. During the course of keratocyte degeneration and necrosis, these dimly reflective “cell processes” (rods) may shrivel, shrink back towards the perikaryon, and eventually disappear, during which sequence of events the granules may be shunted against one another and thereby condensed into a shorter length. This explanation would account for the existence and morphological characteristics of the needle, which were only rarely embraced by a dimly reflective “process”. Generally speaking then, rods and needles could be indicative of apoptotic activity.
Alternatively, the rods could represent pathological collagen synthesised in response to corneal inflammation after surgery. Since collagen is known to have a very slow rate of turnover, the presence of such material at this stage of observation would not be an exceptional finding. However, the morphological characteristics of these rods argue against such a postulate.
A third possibility is that these rods and needles represent accumulations of some reflective material deposited within the corneal matrix along the surfaces of collagen fibres. The possibility of their being regenerating nerve fibres can be excluded, since this process would have been completed long before the time when our observations were made. Moreover, corneal nerves have an appearance quite different from that of either rods or needles.
Owing to the cross sectional nature of this study, our patients were not examined before PRK. In order to establish an unequivocal link between PRK and the presence of rods and needles within the corneal stroma, and to separate contact lens induced changes from those attributable to the effects of excimer laser surgery, further prospective studies are required.
The clinical significance of these stromal changes is currently unknown. But since they were observed up to 3½ after PRK, they probably persist for an even longer period and may even be irreversible. PRK thus leaves the cornea in a permanent state of change. Since the visual result was satisfactory in all patients, the described changes may not interfere with this function. But we cannot at present exclude the possibility that the situation becomes exacerbated with time, such that it reaches the level of clinical relevance.
Acknowledgments
The authors have no commercial interest in the device featured.