Article Text

Abstract
AIM To determine whether the addition of systemic corticosteroid to local intensive corticosteroid therapy of endothelial corneal allograft rejection improves outcome.
METHODS A prospective randomised treatment trial was carried out at a tertiary referral centre. 36 consecutive corneal graft recipients, presenting with a first episode of endothelial graft rejection, received either (i) one intravenous pulse of methylprednisolone 500 mg in addition to local corticosteroid treatment, or (ii) local treatment only. The regimen of local treatment standardised in all cases for the first 24 hours consisted of one subconjunctival betamethasone 2 mg injection and dexamethasone 0.1% drops in the affected eye every hour for 24 hours.
RESULTS Failure to reverse the graft rejection episode was found in 3/36 (8%) patients. Each of these had been treated with local steroid only. Graft failure from any cause occurred in 9/36 (25%) within 2 years of follow up. No statistically significant difference was found between the two groups with regard to reversal of the graft rejection episode, later recurrence of graft rejection, or graft failure.
CONCLUSIONS In treatment of graft rejection, additional systemic treatment with 500 mg methylprednisolone yields no significant benefit over intensive local corticosteroid alone. Graft survival following treatment of a rejection episode with local corticosteroid treatment alone is good in those patients without other risk factors for graft failure and much higher than reported previously.
- corticosteroids
- corneal allograft rejection
Statistics from Altmetric.com
Five year actuarial corneal graft survival in the largest reported cohort is 74%.1 In this and most other reported series, allograft rejection is the most common cause of graft failure. Since earliest reports, corticosteroid therapy has remained the mainstay of immunosuppression for prevention and also treatment of rejection.2 This is despite the fact that steroid therapy fails to reverse all episodes. Reported rates of treatment failure are 24%,3 and 50%4 in the largest reported series. In three other published studies, rather than specifically the proportion successfully reversed by therapy, the proportion of rejection episodes which led to rejection induced graft failure during the follow up period are reported: 38%,548%,6 and 64%.7 In addition to the significant proportion of graft recipients in whom the rejection episode is not reversed by therapy, there is little clinical evidence on the optimum route of administration and regimen of steroid. On an empirical basis, some advocate treatment of the more severe endothelial rejection episodes with systemic steroid in addition to local steroid. Use of the following have been reported: oral prednisolone 80 mg daily for 5–7 days, then tapering doses,3 pulse intravenous methylprednisolone 125 mg with oral prednisolone 1 mg/kg,8 intravenous methylprednisolone 250 mg9 and 500 mg.10 A survey published in 1992 of the graft rejection treatment preferences of 137 members of the Castroviejo Society showed surprisingly wide variation.11One prospective treatment trial on corneal graft rejection by Hillet al compared (a) a single intravenous dose of methylprednisolone 500 mg with (b) 60–80 mg/day oral prednisolone, both given in addition to hourly topical prednisolone acetate 1%. It was found that those graft recipients treated with pulse steroid had (compared with those treated with oral steroid) superior graft survival and less chance of a further rejection only if they presented within 8 days of symptom onset. No difference in outcome was found in those who presented later than day 8, or in the overall study population.12 Accordingly, the question addressed in this study was whether in addition to local steroid treatment alone, systemic steroid immunosuppression yielded superior outcome in terms of reversal of the rejection episode and/or subsequent rejection free graft survival. On account of its marginally increased efficacy compared with oral prednisolone in the above study,12 the regimen of systemic steroid treatment administered was intravenous methylprednisolone 500 mg.
Patients and methods
STUDY POPULATION
Consecutive patients attending Moorfields Eye Hospital with a first episode of endothelial graft rejection at any time after corneal transplantation were considered for recruitment. Donor cornea had been stored in chondroitin sulphate based medium at 4°C before transplantation in all cases. The trial protocol was approved by the hospital ethics committee and all recruited patients gave informed written consent to participate. The diagnostic criteria for endothelial graft rejection were stromal oedema and aqueous cells associated with (i) an endothelial rejection line, and/or (ii) graft keratic precipitates in previously clear graft. Excluded were patients who presented only with epithelial or stromal rejection, recipients of HLA matched or tectonic grafts, and patients under 18 years. To avoid possible complications of the intravenous steroid treatment, patients with a history of hypertension, cardiac or renal disease, or ECG abnormalities were also excluded. Finally, in order to obviate difficulties in the clinical differentiation of graft rejection from recurrent viral keratitis, patients with a primary corneal diagnosis of herpes simplex keratitis were excluded. Clinical variables including previous failed grafts in the affected eye, previous rejection episodes in the affected graft, and slit lamp observations by different clinicians were documented on a standard data recording sheet. The study was terminated 12 months after recruitment of the last patient.
TREATMENT INTERVENTIONS
After eligibility was verified at presentation and written consent given, graft recipients were randomised into two groups based on computer generated binary numbers and assignment was communicated by an administrator independent of the trial team. Patients received either no systemic treatment (group 1) or an intravenous infusion of 500 mg methylprednisolone in 250 ml saline or dextrose over at least 30 minutes (group 2). As no placebo intravenous treatment was given to the control group, the trial was unmasked. All patients in group 2 were monitored for signs of anaphylaxis for the duration of infusion. Local steroid management was identical in both treatment groups for the first 24 hours. All patients were admitted to hospital for inpatient treatment and received one subconjunctival betamethasone 2 mg injection and dexamethasone 0.1% drops in the affected eye every hour for 24 hours. After the initial 24 hours, further topical dexamethasone treatment was continued according to clinical response, being reduced in frequency to 2 hourly and tapered to the dose before onset of the rejection episode.
EVALUATION OF OUTCOME
Patients were first examined 24 hours after initiation of treatment and thereafter daily until observed improvement in graft function or graft failure. Scheduled follow up examinations were undertaken after 1 week, 3 months, and at additional intervals considered necessary according to clinical status. The primary outcome measure was reversal of the rejection episode. This was determined by slit lamp examination as the time at which at least the axial donor cornea was transparent and free of oedema. The interval to any clinical evidence of improvement such as reduction of graft thickness, endothelial rejection line, number of keratic precipitates, or anterior uveitis was documented. The secondary outcome measures were the interval to any subsequent rejection episode or graft failure. Any adverse effects of treatment were recorded at each examination.
STATISTICAL ANALYSES
Statistical analysis of the observations was performed using Fisher's exact test and Cox proportional hazards regression. Actuarial graft survival curves were generated using the Kaplan–Meier survival analysis method and groups compared using the log rank test.
Results
RANDOMISATION AND FOLLOW UP
The trial profile is illustrated in Figure 1, summarising participant flow, numbers and timing of randomisation assignment, interventions, and measurements for each group. Recruitment commenced in November 1994 and ended in May 1997. During this time, 39 graft recipients were eligible to enter the trial. Three patients did not consent to participation. All remaining 36 patients were prospectively enrolled. Follow up ranged from 12 to 40 months, mean 25 (group 1) and 27.8 (group 2). Two patients were lost to follow up after an examination 12 months after recruitment and one patient died after 19 months' follow up. In these patients corneal grafts were transparent at the last visit: they were included in the survival analysis and censored just after the last completed examination. Clinical details of the patients when entering the study are summarised in Table 1. Patients in both treatment groups were similar with respect to demographic characteristics and risk factors for graft rejection. No adverse effects of intravenous methylprednisolone or topical dexamethasone were observed in any patient.

Flow diagram of patient recruitment and follow up. One patient (*) randomised to intravenous steroid received local treatment only in error. Data on this patient were analysed on an intention to treat basis, in the intravenous steroid group.
Baseline patient characteristics in the two treatment groups. Group 1 received local steroid treatment only. Group 2 received 500 mg intravenous methylprednisolone in addition to local treatment
REVERSAL OF REJECTION EPISODE
Clinical outcome data are presented in Table 2. In group 1, local corticosteroid failed to reverse the rejection episode in 3/19 (16%) patients, compared with 0/17 in group 2 (intravenous and local steroid). This difference was not statistically significant (Fisher's exact test, p = 0.23). All three patients in whom graft rejection was not reversed presented within 3 days of symptom onset; two had previous failed ipsilateral grafts and the other was aphakic. While two of these patients presented with an endothelial rejection line, this feature is unlikely to be of prognostic significance as it was found in 26 patients, distributed in equal proportions in the two treatment groups. Finally, the interval to observed clinical improvement following initiation of treatment was similar in both groups.
Clinical outcome in the two treatment groups. Group 1 received local steroid treatment only. Group 2 received 500 mg intravenous methylprednisolone in addition to local treatment
GRAFT FAILURE SUBSEQUENT TO INITIAL REJECTION EPISODE
In each treatment group, three of the grafts surviving the rejection episode failed during follow up; thus in total 6/19 (32%) of the grafts failed in group 1 and 3/17 (18%) in group 2. In none of the grafts that failed during follow up was recurrence of rejection identified as the cause of failure. Details of these six patients with graft failure during follow up are given in Table 3. Actuarial survival curves are shown in Figure 2. Cumulative survival at 12 and 24 months was 68% in group 1 and 82% in group 2. The log rank test comparing the survival in the two groups indicated no statistically significant difference (p = 0.36).
Clinical details of six grafts which survived the treated rejection episode but failed during follow up

Kaplan–Meier analysis of graft survival in treatment groups. Cumulative survival at 12 and 24 months was 68% in group 1 and 82% in group 2. The difference was not significant; log rank test (p = 0.36).
SUBSEQUENT GRAFT REJECTION EPISODES
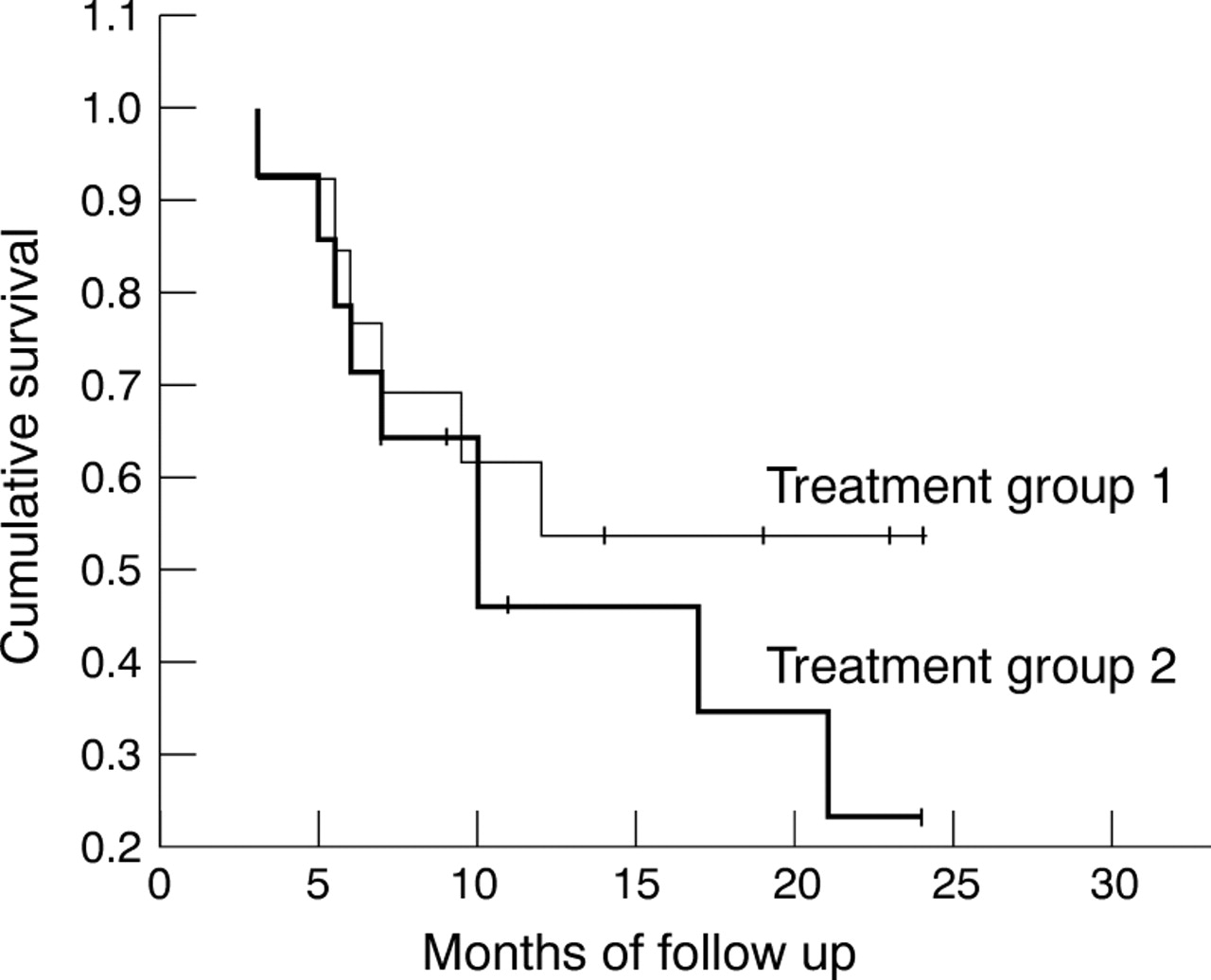
Actuarial survival curves of rejection free survival are shown in Figure 3. Slightly more patients in group 2 (9/14, 64%) had a recurrent rejection episode during follow up than in group 1 (6/13, 46%), at a similar range of intervals following reversal of the presenting episode. These differences were not statistically significant (log rank test, p = 0.30). Recurrence of a rejection episode is conditional on reversal of the presenting episode, and it may be misleading to analyse this outcome in isolation. The cumulative survival for group 1 was 54% (SE 13.8) after 1 and 2 years. For group 2, cumulative survival was 46% (14.3) after 1 and 23% (13.5) after 2 years.

Kaplan–Meier analysis of endothelial graft rejection free survival in treatment groups. Cumulative survival at 12 and 24 months was 53.9% in group 1, 45.9% and 23% respectively in group 2. The difference was not significant; log rank test (p = 0.3).
If either graft failure or recurrence of graft rejection were considered as treatment failure, the survival curve in Figure 4resulted and there was no statistically significant difference (log rank test, p = 0.84). The cumulative survival for group 1 was 37% (SE 11.0) after 1 and 2 years, and for group 2, 41% (12.0) after 1 and 26% (11.5) after 2 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis of combined graft and endothelial graft rejection free survival in treatment groups. Cumulative survival at 12 and 24 months was 36.8% in group 1, 41.2% and 25.7% respectively in group 2. The difference was not significant; log rank test (p = 0.84).
In none of the three survival analyses was there a material change in the findings after further analysis by the Cox proportional hazards regression, with adjustment for effects of age, sex, previous graft, or primary diagnosis (subdivided into endothelial or non-endothelial corneal disease). Further adjustment for the duration of symptoms did not materially alter these findings.
Discussion
The previous prospective studies of graft rejection treatment compared regimens of systemic steroid, without addressing the question as to whether systemic steroid conferred any advantage over local treatment in outcomes. As intravenous methylprednisolone had been shown to be the optimum regimen of systemic corticosteroid12 and a second pulse had been shown to confer no additional advantage,13 we infer from the results of the study reported here that systemic steroid confers no significant advantage over local steroid alone. Moreover, in contrast with the results of these studies, we did not find that intravenous systemic steroid significantly delayed recurrence of a subsequent rejection episode. Although no adverse effects of intravenous methylprednisolone were observed in those subjects treated in this trial, these are a recognised problem with this route of administration—indeed, we excluded from participation any graft recipients with renal or cardiac disease. For all of these reasons we consider that systemic steroid treatment is not justified in treatment of corneal graft rejection.
The proportion of treated patients in this study in whom rejection was reversed (33/36, 92%) is much higher than in previous reports. Earlier publications report success rates of only 50%,476%,3 and 78.9%.13 This might be explained by the high frequency of administration of topical steroid in the first 24 hours, inpatient treatment allowing us to ensure hourly application of steroid drops. A less likely reason is comparatively earlier attendance by patients following onset of symptoms of rejection. Rejection treatment commenced at a mean of 4.3 days following symptom onset, compared with 8 days reported by Hill and co-authors.12 However, we found no significant correlation between duration of symptoms and failure to reverse the rejection episode, recurrence of rejection or failure from any cause during follow up. One further factor which is likely to influence the success of rejection episode therapy is the risk profile of the graft recipients under study. In the study reported here, recipients were a mixed group of those at low and high risk of rejection, whereas in one previous study of patients at high risk of rejection (randomised to receive antigen matched corneas rather than to a treatment regimen), 38% of grafts were found to fail because of rejection.5One final factor which might contribute to the superior treatment outcomes compared with previous reports is a comparatively long interval between surgery and randomisation. The mean interval in this group was 19.5 months, longer than that in treatment groups reported by Pleyer et al 14 and Alldredgeet al 3 in which the mean interval was 8 months. We cannot exclude the possibility that endothelial rejection episodes commencing earlier following surgery are more resistant to therapy.
Because human corneal endothelial cells do not replicate to any clinically meaningful extent it is endothelial graft rejection, rather than forms of rejection involving as targets the more superficial graft cell layers, that has greatest impact on graft survival.3 15 Musch et alfound that graft rejection increased the endothelial cell loss in patients with keratoconus followed up following the rejection episode.16 Injury to the graft endothelium by allogeneic effector cells eventually leads to endothelial decompensation and irreversible graft opacification—graft failure. The likelihood of a rejection episode resulting in graft failure, either in the acute phase or after a variable interval following initial deturgescence on therapy, depends critically on (i) how early the rejection episode can be reversed, and (ii) the graft endothelial cell density before rejection onset. Even if there is a high density of endothelial cells, untreated or undertreated rejection is likely to reduce the endothelial cell density to below threshold levels necessary for maintenance of corneal clarity. If the endothelial cell density is low, even a successfully treated and reversed rejection episode may lead to graft failure, possibly after transparency is initially recovered. Although in this study we do not have information on donor endothelial cell density before rejection onset, we have shown that rejection was reversed in most patients in both treatment groups. Later graft failure in the absence of recurrent rejection episodes may be due to eventual decompensation following allogeneic endothelial injury in the initial episode. Continued graft endothelial cell loss in the absence of evident causes has been shown by Bourne and colleagues to continue for up to 10 years post-keratoplasty.17 18 It is of interest that of the six grafts which survived the rejection episode but subsequently failed, four recipient eyes had undergone intraocular surgery before corneal transplantation. This is a finding previously discussed by Harper and colleagues, one possible explanation for the association being that low endothelial cell density in the host peripheral cornea induces migration of donor endothelial cells to host cornea.19
This study had a reasonable chance (>80% statistical power) of detecting a difference in outcome proportions in the order of 40%. The study would have even more power to detect larger differences in treatment outcome, but the sample size limits the power to detect smaller differences. However, there was no evidence of a major beneficial effect with respect to either reversal of the rejection episode, reduction in later recurrence of rejection, or graft failure. We conclude that (i) endothelial rejection treatment outcomes are much more successful than previously reported and (ii) systemic steroid treatment in addition to intensive local steroid does not yield a significant improvement in outcome.
Acknowledgments
We thank our colleagues in the Corneal and External Diseases Service at Moorfields Eye Hospital who recruited patients for the trial. TH was supported by Deutsche Forschungsgemeinschaft (grant Hu 761/1–1).