Article Text

Abstract
Background/aims: Past studies have explored some of the associations between particular motor and sensory characteristics and specific categories of non-neurological infantile nystagmus. The purpose of this case study is to extend this body of work significantly by describing the trends and associations found in a database of 224 subjects who have undergone extensive clinical and psychophysical evaluations.
Methods: The records of 224 subjects with infantile nystagmus were examined, where 62% were idiopaths, 28% albinos, and 10% exhibited ocular anomalies. Recorded variables included age, mode of inheritance, birth history, nystagmus presentation, direction of the nystagmus, waveform types, spatial and temporal null zones, head postures and nodding, convergence, foveation, ocular alignment, refractive error, visual acuity, stereoacuity, and oscillopsia.
Results: The age distribution of the 224 patients was between 1 month and 71 years, with the mean age and mode being 23 (SD 16) years and 16–20 years respectively. By far the most common pattern of inheritance was found to be autosomal dominant (n = 40), with the nystagmus being observed by the age of 6 months in 87% of the sample (n = 128). 139 (62%) of the 224 subjects were classified as idiopaths, 63 (28%) as albinos, and 22 (10%) exhibited ocular anomalies. Conjugate uniplanar horizontal oscillations were found in 174 (77.7%) of the sample. 32 (14.3%) had a torsional component to their nystagmus. 182 (81.2%) were classed as congenital nystagmus (CN), 32 (14.3%) as manifest latent nystagmus (MLN), and 10 (4.5%) as a CN/MLN hybrid. Neither CN nor MLN waveforms were related to any of the three subject groups (idiopaths, albinos, and ocular anomalies) MLN was found in idiopaths and albinos, but most frequently in the ocular anomaly group. The most common oscillation was a horizontal jerk with extended foveation (n = 49; 27%). The amplitudes and frequencies of the nystagmus ranged between 0.3–15.7° and 0.5–8 Hz, respectively. Periodic alternating nystagmus is commonly found in albinos. Albino subjects did not show a statistically significantly higher nystagmus intensity when compared with the idiopaths (p>0.01). 105 of 143 subjects (73%) had spatial nulls within plus or minus 10° of the primary position although 98 subjects (69%) employed a compensatory head posture. Subjects with spatial null zones at or beyond plus or minus 20° always adopted constant head postures. Head nodding was found in 38 subjects (27% of the sample). Horizontal tropias were very common (133 out of 213; 62.4%) and all but one of the 32 subjects with MLN exhibited a squint. Adult visual acuity is strongly related to the duration and accuracy of the foveation period. Visual acuity and stereoacuity were significantly better (p<0.01) in the idiopaths compared to the albino and ocular anomaly groups. 66 subjects out of a sample of 168 (39%) indicated that they had experienced oscillopsia at some time.
Conclusions: There are strong ocular motor and sensory patterns and associations that can help define an infantile nystagmus. These include the nystagmus being bilateral, conjugate, horizontal uniplanar, and having an accelerating slow phase (that is, CN). Decelerating slow phases (that is, MLN) are frequently associated with strabismus and early form deprivation. Waveform shape (CN or MLN) is not pathognomonic of any of the three subject groups (idiopaths, albinos, or ocular anomalies). There is no one single stand alone ocular motor characteristic that can differentiate a benign form of infantile nystagmus (CN, MLN) from a neurological one. Rather, the clinician must consider a host of clinical features.
- infantile nystagmus
- congenital nystagmus
- manifest latent nystagmus
- albino
- visual acuity
Statistics from Altmetric.com
Infantile nystagmus is an involuntary, bilateral, conjugate oscillation of the eyes which is present at birth or develops within the first 6 months of life.1–4 Frequently, the oscillation is in the horizontal plane. It may be associated with an afferent visual defect such as albinism, congenital cataract or optic atrophy, or may appear where no visual or neurological impairment is detected, when it is termed idiopathic5–7 (Fig 1). The methods of diagnosis by which subjects are classified are well established. None the less, congenital idiopathic nystagmus can sometimes be diagnosed only by exclusion.

A schematic classification for infantile nystagmus based on the possible association with one of two nystagmus waveforms (congenital nystagmus (CN) and manifest-latent nystagmus (MLN)) and various associated anomalies.
Estimates of the prevalence of infantile nystagmus range from 1 in 1000 to 1 in 6000.8–12 Oculocutaneous albinism and ocular albinism are almost invariably linked to infantile nystagmus and have a prevalence of 1 in 20 000 and 1 in 50 000, respectively.13 Such differences in the recorded estimates of prevalences often reflect sampling bias, misclassification, and ethnic differences. Infantile nystagmus accounts for between 6% and 10% of children who are registered partially sighted or blind in the developed countries.14–17 Estimates from low vision clinics and schools suggest percentages ranging from 2–8%.17–20
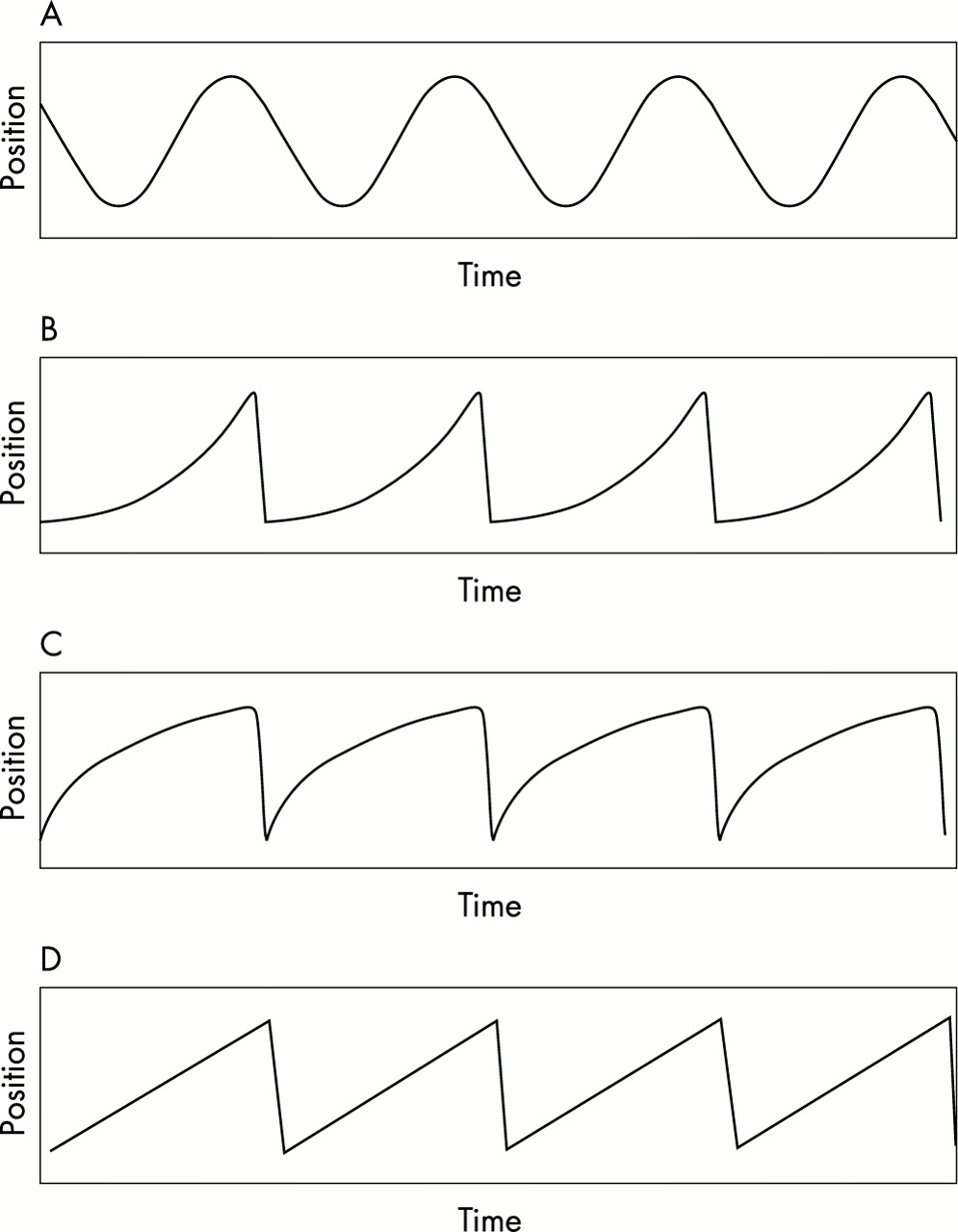
There are three major manifestations of infantile nystagmus: congenital nystagmus (CN), manifest latent nystagmus (MLN), and latent nystagmus (LN).1–7 Their principal differences lie in the form of their slow phases.1,21–27 CN has a slow phase with an increasing exponential velocity form (Fig 2B), while in MLN and LN the slow phase velocity is decreasing (Fig 2C) or linear (Fig 2D). Additional distinguishing features relate to the fast phase (that is, the beat direction), which in MLN and LN always beats towards the viewing eye, and in the manner in which the oscillation is driven during binocular and monocular viewing.24–27 The low velocity portion of the slow phase (during which the image of the object of regard rests close to, or on, the fovea) is referred to as the foveation period.21–23,28 The position of gaze where the intensity of the oscillation is minimal is called the null zone.5,29,30 As well as null zones fixed in space, some patients exhibit temporal shifts in the gaze angle at which the null occurs. The oscillation is then called a periodic alternating nystagmus.5,6,31–34
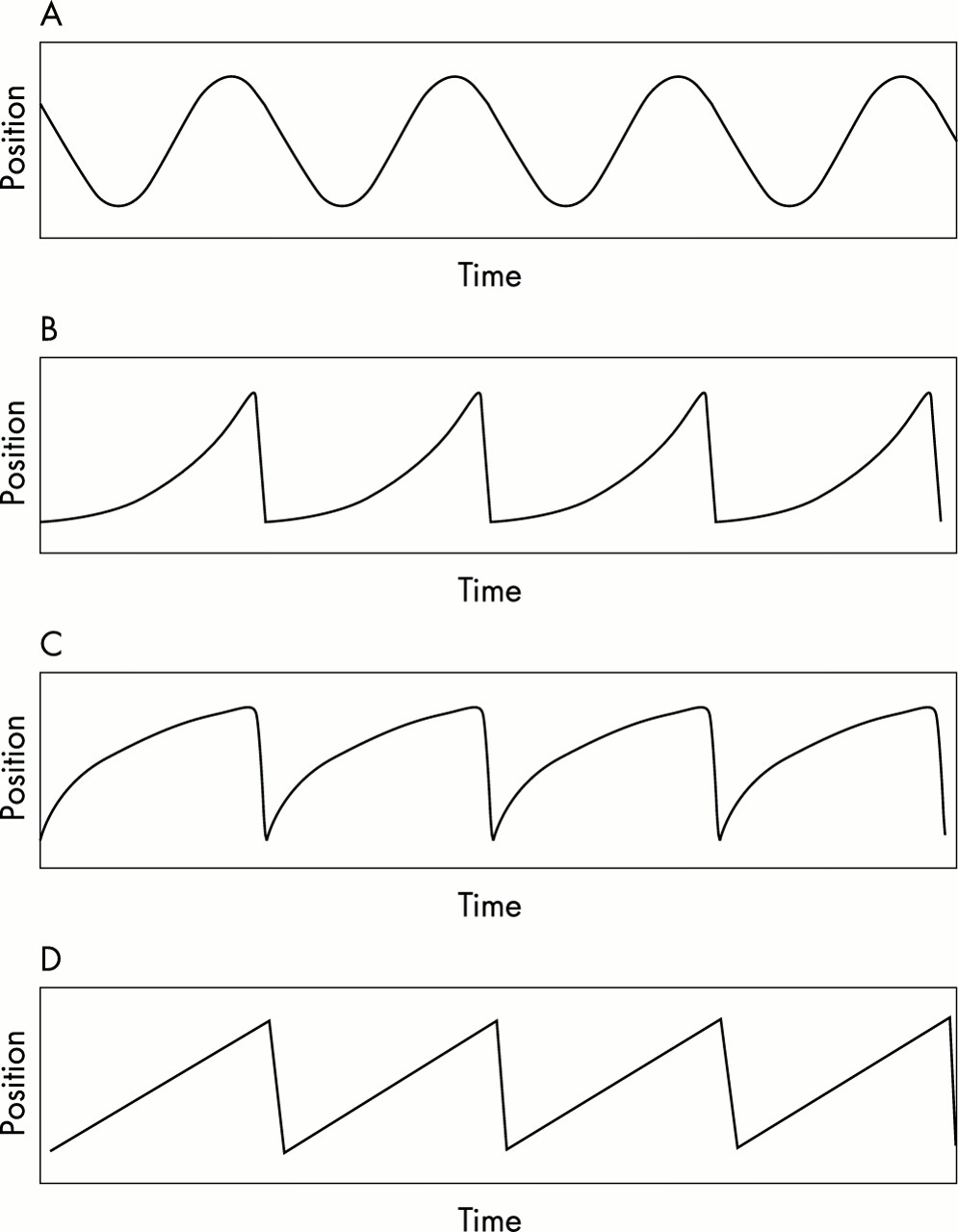
A schematic illustration of nystagmus waveforms (A) pendular nystagmus, (B) an accelerating velocity exponential slow phase jerk nystagmus (CN), (C) a decelerating exponential slow phase jerk nystagmus (MLN), (D) a linear or constant velocity slow phase jerk nystagmus (MLN). In (A) a slow phase is followed by a slow phase while in (B)–(D) a slow phase is followed by a fast phase.
Infantile nystagmus waveform shapes can be jerk, pendular, or a combination of the two. At least 12 different CN waveforms23 and six different MLN waveforms27 have been described. An important feature of infantile oscillations is that they can be greatly modified by a number of factors including, fixation attempt, fatigue, stress, and attention.2–6,22,26,27
CASE STUDIES
Case studies can provide useful and detailed information about the sensory and motor characteristics of a group of patients with similar diagnoses.35–37 To date, there has only been one in-depth retrospective study on a large population of patients with CN, LN, and MLN.1 Its principal objective was to describe the clinical and ocular motor characteristics that define and separate CN from LN and MLN. To this end, the author, Dell’Osso, was singularly successful. The purpose of this present communication is to greatly extend his study by analysing both the ocular motor and the perceptual behaviour of 224 subjects with infantile nystagmus. All subjects had undergone a battery of clinical and psychophysical investigations which included many tests of sensory and motor performance. By describing the trends and associations it is hoped to advance our understanding of infantile nystagmus and assist the clinician in practice.
METHODS
Subjects
The case records of over 250 subjects with infantile nystagmus were examined. The subjects had been involved in clinical and psychophysical investigations at the University of Manchester Institute of Science and Technology (UMIST) Oculomotor Research Laboratory over the past 23 years. A number of subjects were omitted from the study because their records were incomplete, leaving a total of 224 to be included in the case study. Data collection sheets were designed to record pertinent motor and sensory details. Categorisation into one or other of the two groups, idiopath or associated sensory defect, was done on the basis of a battery of biochemical (for example, hair bulb test) and clinical tests (for example, slit lamp, ophthalmoscopy, and electrodiagnosis). On many occasions the oculomotor characteristics of the nystagmus were checked and reanalysed from the original paper traces or computer files. The majority of the subjects had attended our laboratory on more than one occasion and many had visited on more than four occasions. These multiple visits made it more likely that the subject’s habitual nystagmus was being recorded. Informed consent was obtained according to the tenets of the Declaration of Helsinki.
The age of our subject group (n = 224) ranged from between 1 month and 71 years, with a mode of 16–20 years and mean of 23 (SD 16) years (Fig 3). The age of each subject refers to the age at which the investigation took place. The distribution had a positive skew.
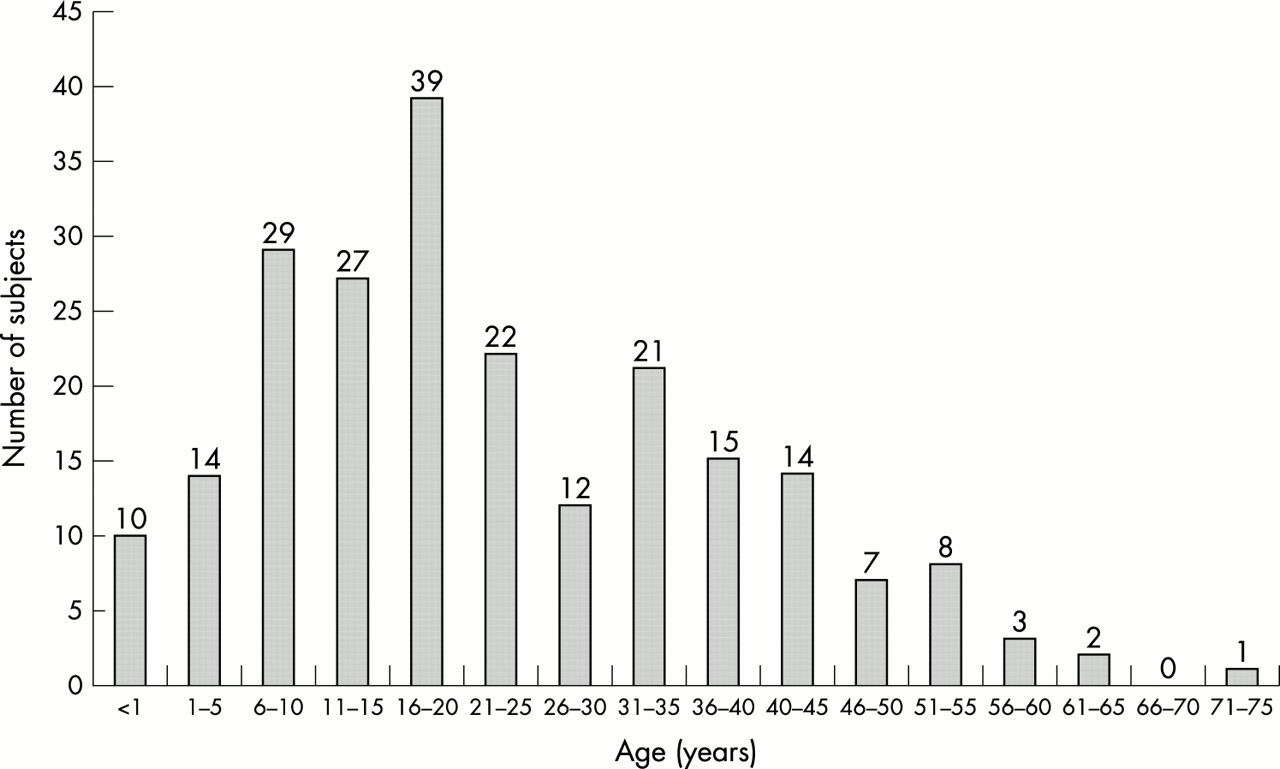
The age distribution of the 224 subjects who were involved in the case study. Mode = 16–20 years and mean 23 (SD 16) years.
Eye movement recording
Infrared limbal reflection recording systems (ACS Applied Research Developments, Manchester, UK and Skalar Medical, Delft, Netherlands) were used on all but the very youngest subjects (that is, <1 year) where bitemporal DC electro-oculography22 was used. The binocular eye movement recordings were either sent directly to a four channel chart recorder or relayed to a computer for offline analysis.5,27 Eye velocity information was retrieved by differentiating the position signal. The nystagmus was measured when the subjects viewed a stationary target in the straight ahead position and at subsequent 10° gaze position shifts up to plus or minus 40°. Eye movements were generally calibrated by presenting a pursuit stimulus that moved horizontally over a range of plus or minus 10° in a sinusoidal or triangular manner. Vertical eye movements were calibrated by subjects making plus or minus 5° volitional saccades. Infant eye movements were calibrated by encouraging reflex saccades to toys, bells, and/or light sources mounted in the primary position and plus or minus 10° either side of the primary position. Chin rests with supplementary cheek supports were used to stabilise head position. Fundus video recordings (VEB Carl Zeiss Jena) were also made on a number of subjects to assess the vertical and torsional components of any oscillations and to examine the degree of foveation.5,38
Data refer to the eye movements recorded during binocular and monocular viewing of a stationary target in the primary position situated 114 cm from the subject.
Ocular motor characteristics
The amplitude and the frequency of the nystagmus were defined as the peak to peak excursion of the oscillation and the number of cycles per second, respectively. Waveforms were characterised on the basis of studies conducted by Dell’Osso and Daroff23 and Abadi and Scallan.27 Null zones, head postures, and head nodding were examined in the laboratory using techniques described in Abadi and Whittle.30 Vergence was assessed using a dynamic near target, and ocular alignment was examined at 6 metres and ⅓ metre.5,6,39
We defined the waveform exhibited for more than 85% of the recording time as the primary waveform shape.
Sensory characteristics
Visual acuity was assessed using either a high contrast Snellen or Bailey-Lovie chart at 6 or 3 metres. The refractive state was determined using a combination of retinoscopy and subjective techniques40 and stereo vision was examined using either the TNO or Wirt stereoplates.
RESULTS
Inheritance and classification
In all, 152 of the 224 subjects (67.8%) had no family history of infantile nystagmus and the mode of inheritance was uncertain in 15 (6.7%). Of the remaining 57, the most common pattern of inheritance was found to be autosomal dominant (n = 40, 70.2%) followed by X linked (n = 15; 26.3%) and autosomal recessive (n = 2; 3.5%). Only 85 (38%) of the 224 subjects provided reliable information about their birth history; of these, 72 (85%) were classified as full term normal delivery and 13 (15%) as premature. The presence of a nystagmus was recorded during the first 6 months in 128 out of 147 subjects (87%), in 12 subjects between 6 and 12 months, and for seven subjects the nystagmus was not noticed until at least 12 months had lapsed.
A total of 139 (62%) of the 224 subjects were classified as idiopaths, 63 (28%) as albinos, and 22 (10%) exhibited ocular anomalies such as infantile cataract, optic nerve hypoplasia, and retinal dystrophy.
The direction of the nystagmus
The distribution of the plane of the nystagmus motion recorded during binocular viewing for all 224 subjects is shown in Table 1. A total of 174 out of 224 subjects exhibited a uniplanar horizontal oscillation. The next largest group were 27 subjects with combined horizontal and torsional oscillations. Indeed, in all, a total of 32 displayed a torsional component to their nystagmus. Six subjects had both a horizontal and vertical component to their oscillations. Interestingly, there were four subjects—three idiopaths and one ocular anomaly—with uniplanar vertical (albeit small amplitude ≤1°) oscillations. Multiplanar oscillations (horizontal, vertical, and torsional) accounted for eight of the total. There was no statistically significant difference in the plane of oscillation during binocular and monocular viewing for the CN subjects (p>0.01).
The direction of the nystagmus plane in 224 subjects
The nystagmus waveforms
A breakdown of the oscillation types based on whether the slow phase had either an accelerating (CN), or decelerating/linear velocity (MLN) profile is given in Table 2. By far the greatest proportion of the 224 subjects exhibited a CN waveform (that is, an increasing velocity slow phase; n = 182; 81.2%), followed by an MLN waveform (that is, linear or decreasing velocity slow phase; n = 32; 14.3%), while 10 (4.5%) had a mixture of CN and MLN waveforms. Figure 4 shows how these waveform types were distributed among the three subject classes (idiopaths, albinos, and ocular anomalies). No one waveform type was specific to any of the three subject classes.
The distribution of waveform types seen among the idiopath, albino, and ocular anomaly groups (n=224)
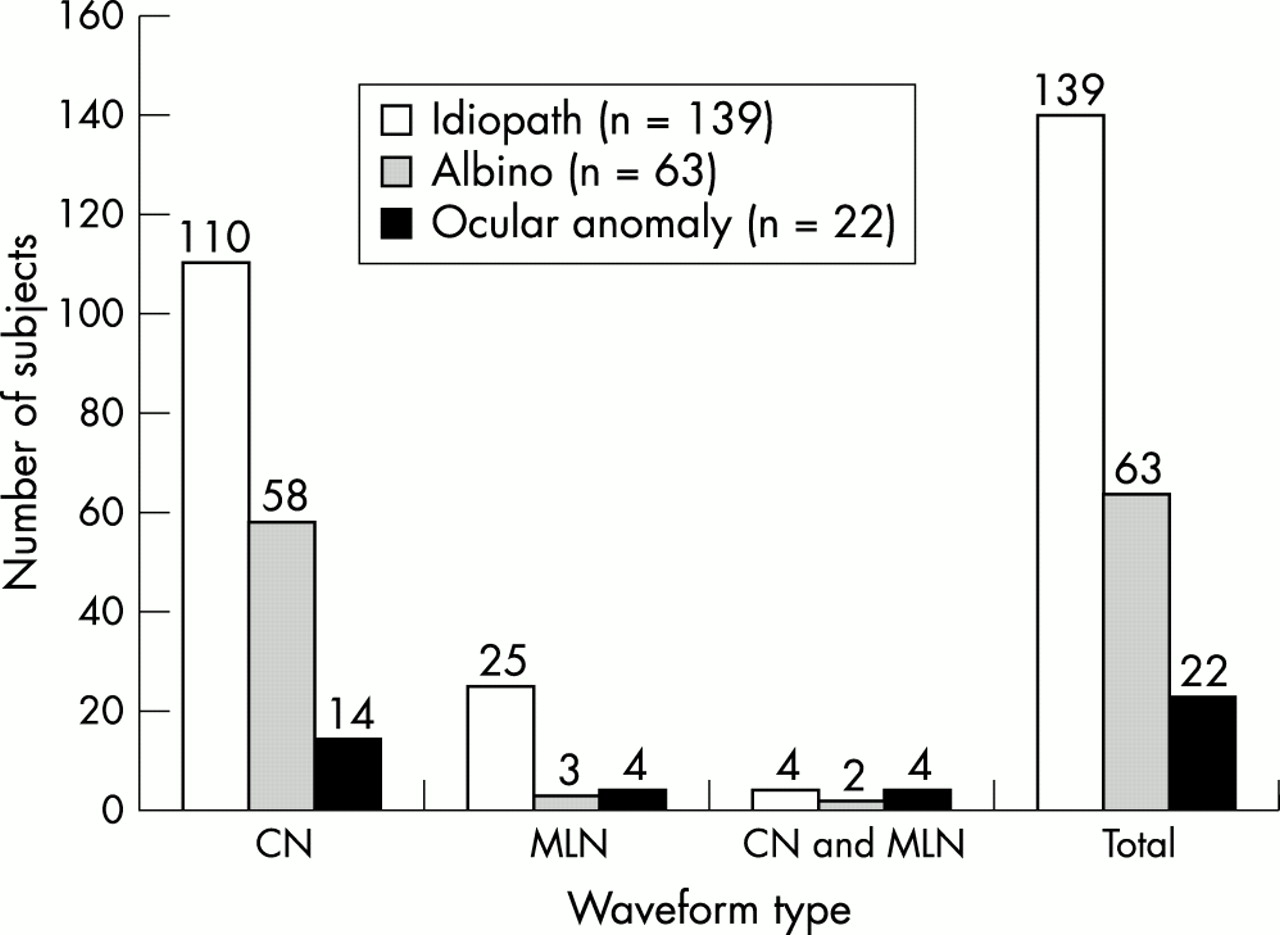
The distribution of waveform types seen among the idiopath (n = 139), albino (n = 63), and ocular anomaly (n = 22) subject groups for all 224 subjects.
For 182 subjects, the CN waveform was further subdivided into at least 12 distinct classes of oscillations, the distribution of which can be seen in Figure 5. The six most commonly encountered CN oscillations were found to be the jerk with extended foveation (Jef) (n = 49; 27%), the pendular/asymmetrical pendular (P/AP) (n = 33; 18%), the jerk, (J) (n = 24; 13%), the pseudocycloid (PC) (n = 21; 12%), the pendular with foveating saccades (Pfs) (n = 15; 8%), and the bidirectional jerk (Bdj) (n = 12; 7%). Five subjects (3%) had a sustained mixture of two different CN oscillations (hybrids) and 16 subjects (9%) exhibited greater than 2 CN classes of oscillations (that is, multiple).

The distribution of the 12 classes of waveforms seen in 182 subjects who exhibited a CN. P/AP = pendular/asymmetrically pendular, Pfs = pendular with foveating saccades, J = pure jerk, Jef = jerk with extended foveation, PC = pseudocycloid, DJ = dual jerk, Bdj = bidirectional jerk, J and DJ = jerk and dual jerk hybrid, Pfs and PC = pendular with foveating saccades and pseudocycloid hybrid, P/AP and PC = pendular/asymmetrical pendular and pseudocycloid hybrid, PC and DJ = pseudocycloid and dual jerk hybrid, Multiple = more than two different CN oscillations.
Recently Abadi and Scallan27 have proposed that four distinct types of MLN can be distinguished (see Fig 6). These four types represent a spectrum from latent nystagmus (type 1 MLN) to the classic (type 4 MLN). Their differences are based on the state of fixation during binocular viewing: type 1 MLN (steady), type 2 MLN (square wave jerks), type 3 MLN (torsional nystagmus only), and type 4 MLN (horizontal jerk nystagmus). Three of four types exhibit uniplanar oscillations on monocular viewing. Of the MLN types found among the 32 subjects, by far the largest group was type 4 MLN (n = 17; 53%), followed by type 3 MLN (n = 10; 31%) and type 2 MLN (n = 2; 6%). Three subjects showed a combination or hybrid of two of the MLN types. There were no type 1 MLN subjects in our sample.
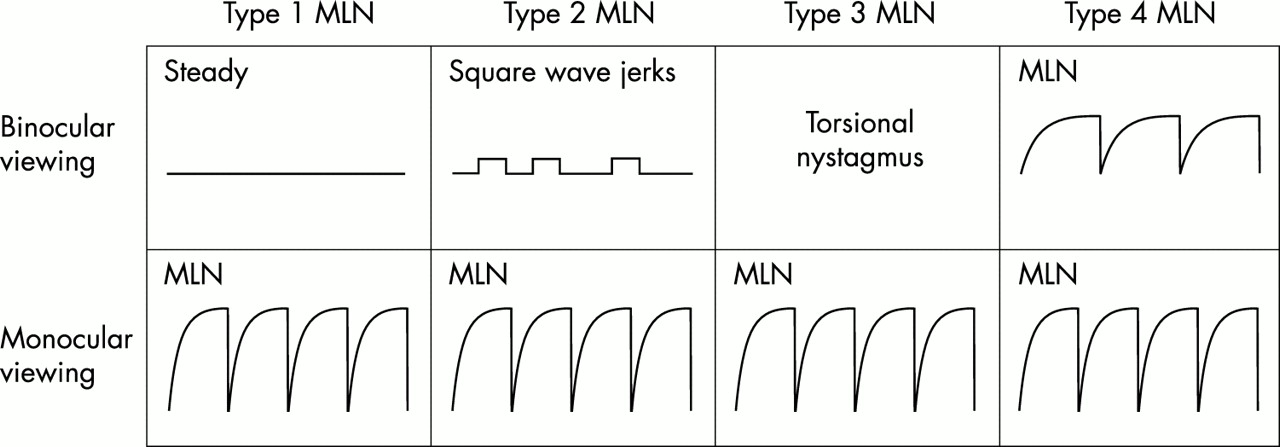
A schematic illustration of the four types of manifest latent nystagmus (MLN). During binocular viewing the eyes exhibit one of four states: stability (type 1 MLN), square wave jerks (type 2 MLN), torsional nystagmus (type 3 MLN), or a horizontal MLN (type 4 MLN). All four types show a typical MLN during monocular viewing with the fast phase beating toward the viewing eye.
Amplitude and frequency of the nystagmus
The ranges and means of the nystagmus amplitudes, and frequencies encountered in the 224 subjects showed that while frequencies tended to remain within tight limits (0.5–8 Hz; mode 2–3 Hz), the amplitude was found to have a greater variance (0.3–15.7°). The adult albino subjects did not show a statistically significant higher nystagmus amplitude compared with the adult idiopath group (p>0.01).
Null zones and head postures
In all, 195 of the 224 subjects had the position and extent of their null zones investigated. Of these, 27 had MLN and eight had a CN/MLN oscillation. Both the MLN and CN/MLN groups were excluded from the analysis because the switching of the viewing eye or the use of their adducting eye to fixate could strongly influence the position of the null zone. The 17 subjects who exhibited a dynamic null (that is, a periodic alternating nystagmus) were also excluded. The distribution of the null zones of the remaining (143) are illustrated in Figure 7. A total of 105 of 143 subjects (73%) had spatial null zones within plus or minus 10° of the primary position. All of the subjects (n = 38) with null zones at, or beyond, plus or minus 20°, adopted a constant compensatory head posture; 98 of the 143 subjects (69%) employed abnormal head postures at some time during the day.

The distribution of the position of the null zone for 143 of the subjects with CN. Note: subjects with manifest latent nystagmus (n = 27), periodic alternating nystagmus (n = 17), and hybrid oscillations (n = 8) were excluded from the original pool of 195 subjects.
Head nodding was found to be present in 38 out of 143 subjects (27%) in the group, 29 of whom also adopted an abnormal head posture. Interestingly, of the 17 subjects with a dynamic null only four head nodded. The adoption of a head posture or head nodding did not appear to be linked to any one particular classification group of subjects (that is, idiopath, albino, or ocular anomaly).
Convergence
The effect of convergence on the intensity of the nystagmus was examined in 117 of 224 subjects, of which, 52 (44%) elicited a decrease in the nystagmus intensity during near fixation (⅓ metre) compared with distance fixation (6 metres). Vergences closer than 25 cm (>24 prism dioptres) invariably gave rise to much greater attenuations in the nystagmus intensity. The subjects were evenly distributed among the idiopath, albino, and ocular anomaly groups.
Ocular alignment
A total of 213 of the 224 subjects were examined for ocular alignment. Of these, 136 (64%) exhibited a strabismus, 57 of whom were albinos. Horizontal tropias accounted for over 98% of the squints with a roughly equal division between eso and exo deviations. Only one of the 32 subjects with an MLN waveform did not exhibit a strabismus.
Sensory performance
Visual acuity and foveation
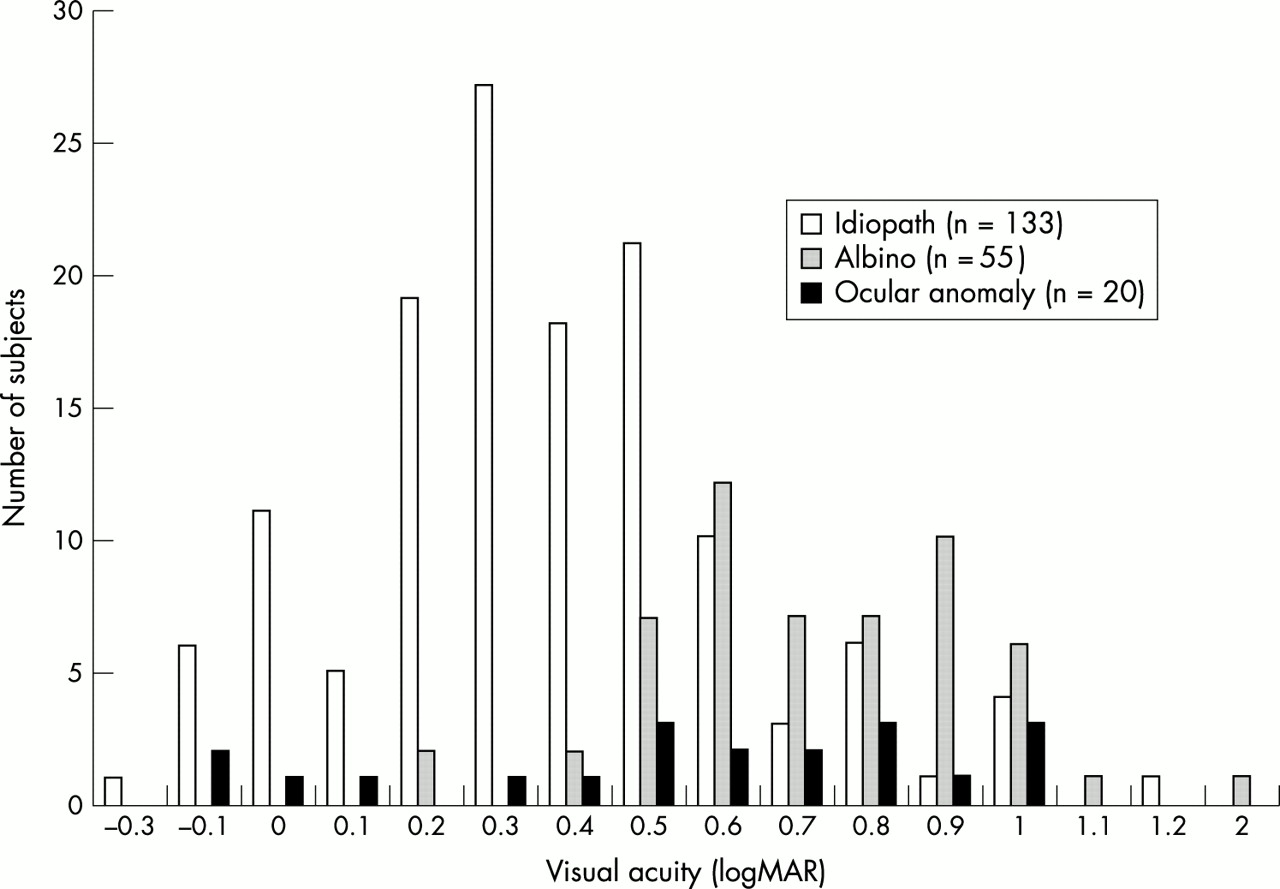
The range of distant (that is, 6 metres) visual acuities for the idiopath (n = 133), albino (n = 55), and ocular anomaly (n = 20) subjects recorded during binocular viewing is shown in Figure 8. The mean visual acuity level for the idiopaths (+0.35 (SD 0.26) logMAR) was significantly higher (p<0.01) than the albino (+ 0.67 (0.28) logMAR) and ocular anomaly groups (0.55 (0.36) logMAR).

The distribution of binocular logMAR visual acuities for the idiopath (n = 133), albino (n = 55), and ocular anomaly (n = 20) groups.
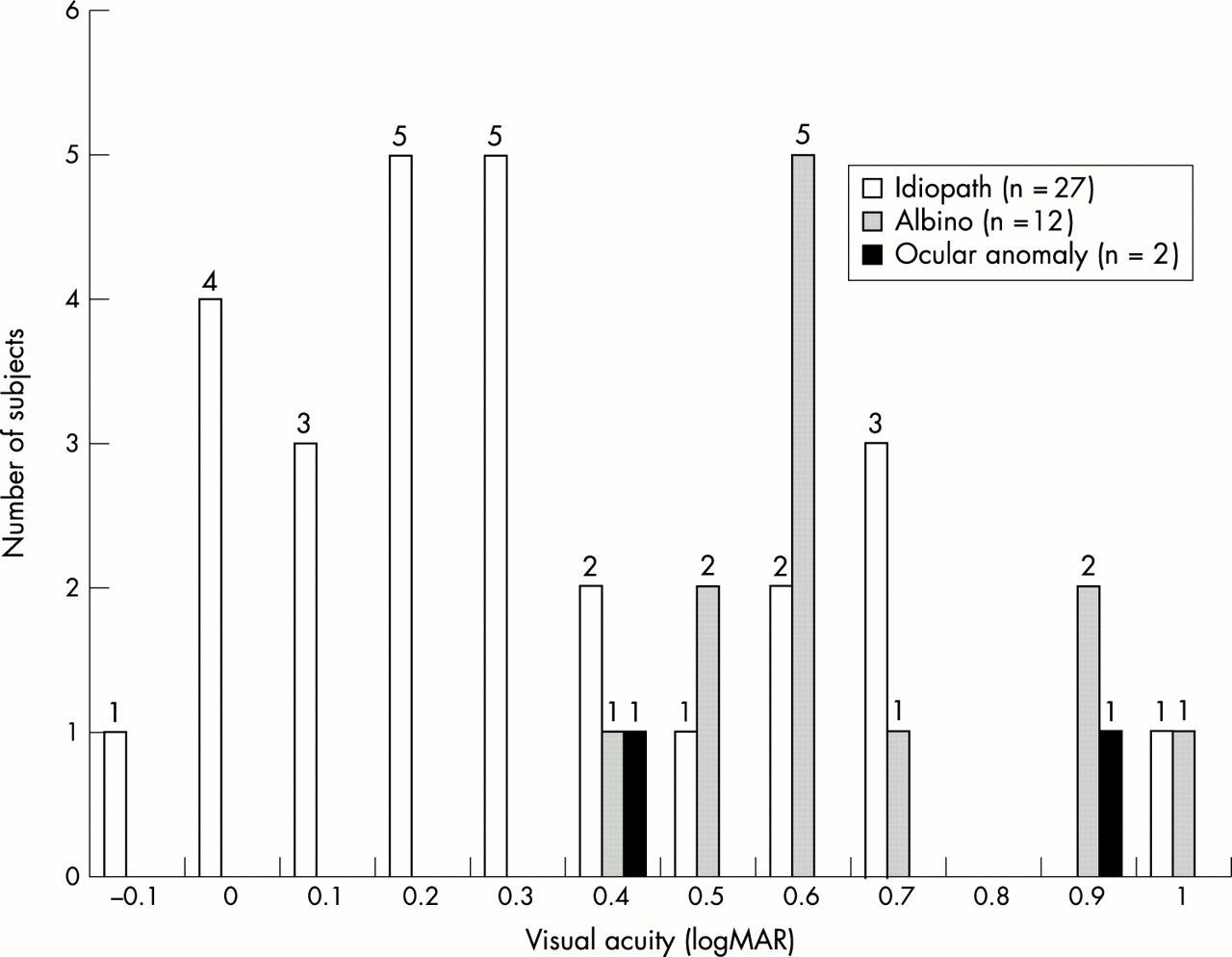
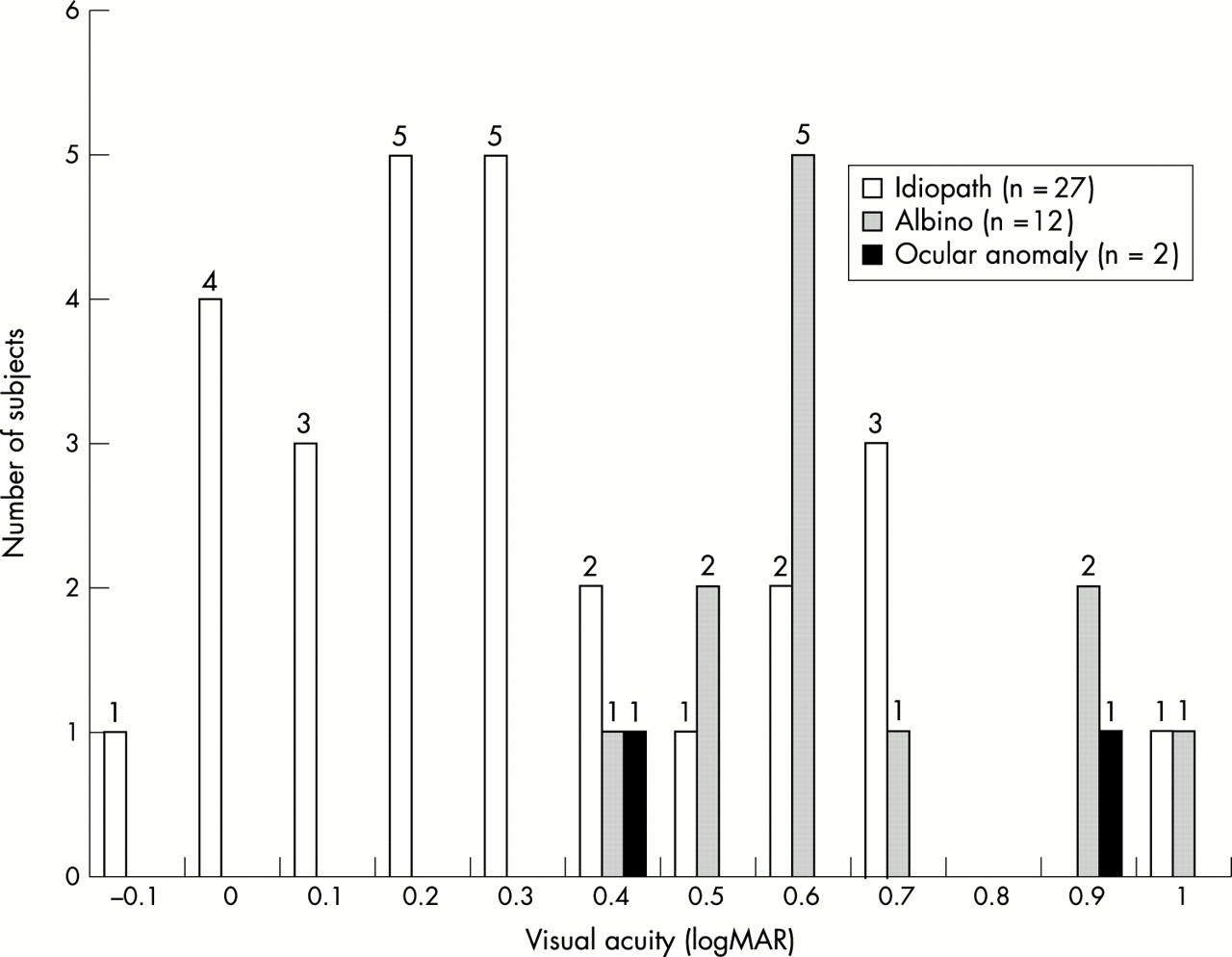
The ability to foveate was carefully assessed in 74 (33%) of the 224 subjects using fundus video oculography. Forty one of the 74 subjects (55%) exhibited foveation: 27 idiopaths, 12 albinos, and two with ocular anomalies. The distribution of visual acuities (logMAR) during binocular viewing in subjects who exhibited foveation is illustrated in Figure 9. Note that foveation does not necessarily guarantee high levels of visual acuity. Thirty three subjects were classed as CN, four as MLN, and four with CN and MLN. Two of the CN subjects also had a periodic alternating nystagmus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The distribution of logMAR visual acuity levels in the 41 subjects who exhibited foveation. All acuity measures were recorded during binocular viewing of a 6 metre distant acuity chart.
Refractive error
A notable feature of the refractive state of the 122 subjects (70 idiopaths, 44 albinos, and eight ocular anomalies) who were examined, was the high incidence of with the rule astigmatism. Of the 69 (57%) who had astigmatic errors greater than 2.0D, there were 30 idiopaths, 34 albinos, and five with ocular anomalies.
Stereoacuity
Stereoacuity was assessed in 176 of the 224 subjects. The majority (n = 116, 66%) displayed either no stereoacuity or very gross acuity levels (that is, 3000 seconds of arc). The idiopathic group (n = 111) showed significantly better stereoacuity levels than either the albino (n = 50) or ocular anomaly groups (n = 15). 16 of 111 subjects had stereoacuity levels of 60 seconds of arc or better. There were only two albinos out of 50 and one ocular anomaly subject out of a sample of 15 who had stereoacuity levels better than 3000 seconds of arc. Only one out of 23 subjects with MLN exhibited a stereoacuity level better than 3000 seconds of arc.
Oscillopsia
Of the 168 questioned about spatial constancy, 66 (39%) reported that they had experienced oscillopsia under binocular viewing conditions; 53 of the 66 had CN, 10 had MLN, and three were a CN/MLN hybrid and indicated that they had experienced intermittent oscillopsia when they were stressed, tired, excited, or were concentrating on a task (that is, “the effort to see”). Nine of the 66 subjects had a periodic alternating nystagmus. Some subjects also reported that under monocular viewing conditions they experienced some degree of oscillopsia. They invariably had an MLN.
DISCUSSION
The potential for bias
Past case studies on infantile nystagmus have been limited to smaller numbers of patients and restricted variables. The 224 subjects who took part in this study were part of a larger database of individuals seen by the UMIST Eye Movement Group and were all volunteers for a number of research programmes. Over the years the UMIST group has concentrated its studies on albinos and idiopaths rather than subjects who had ocular anomalies. Subjects with ocular anomalies were not actively sought because the frequent multiplanar oscillations made psychophysical experiments difficult to interpret and control. Our case study numbers clearly reflect a bias because of this selection process.
Although the age of the subjects in this case study ranged from 1 week to 71 years of age, the vast majority of the subjects (>93%) were of an age where higher resolution infrared (as opposed to electro-oculography) techniques could be used. In addition, older subjects were more able to cooperate during the eye movement calibration and test procedures as well as being more capable of carrying out psychophysical tasks. These factors meant that infants were under-represented in the nystagmus data collection section of the case study.
Only 57 out of 224 subjects were able to indicate a possible family history of nystagmus. Our difficulty in establishing a clear mode of inheritance is not a unique problem. The socioeconomic changes in the past 40 years including families becoming smaller, greater dispersion of family members, adoption, and the more frequent change of partners, has meant that mapping family trees has become somewhat more difficult than in the past. These factors are less problematic in the close knit Scandinavian communities, where there is also compulsory registration of the blind and visually impaired. Forty out of our pool of 57 subjects appeared to show an autosomal dominant inheritance pattern. Such a large percentage is at odds with previous reports8–11 and may reflect the factors mentioned earlier. In addition, an autosomal dominant pattern of inheritance is easier for family members to report.
We categorised birth history into one of four groups: full term normal delivery, premature, trauma during pregnancy or delivery, and others. The first two categories refer directly to the delivery time. Once again, our sample (n = 86) was potentially limited by the reliability of the information and recall bias. None the less, of the 86 subjects, 13 (15%) were classified as premature births, which is twice the reported UK average of between 6–7%.41
Presentation time of infantile nystagmus
Infantile nystagmus is generally defined as presenting before 6 months of age.42 This study found that out of a sample of 147 subjects, nystagmus was detected at birth in 30% (n = 44) and that this figure increased to 66% (n = 97) by 3 months and to 87% (n = 128) by 6 months postnatally. The detection of infantile nystagmus is dependent on a number of factors: sample size, the care and attention of the attendant clinician, the express desire of the family to examine the eyes of their child, the nature and timing of the postnatal support services, and the intensity of the nystagmus. These detection factors may explain why Reinecke and his colleagues43 reported that not one of their 35 subjects with infantile nystagmus exhibited a nystagmus at birth.
Not surprisingly, a critical factor in recognising the presence of infantile nystagmus is the nature of the nystagmus itself. In young infants the oscillations can consist of a large amplitude (∼ 30°), low frequency (∼ 1 Hz) and asymmetrical pendular movement.5,43,44 In these cases ocular movements are often missed or mistaken as volitional following eye movements rather than judged to be an involuntary nystagmus. A recent study of the fixational eye movements of infants with infantile cataracts45 supports the need for quantitative measures of fixation. A number of sustained and intermittent oscillations with amplitudes between 20 seconds and 80 seconds of arc were quantitatively recorded with infrared oculography, most of which would certainly have been missed if the device had not been used. The use of such devices to detect microfixation instabilities is also supported by longitudinal studies carried out by Hertle and his colleagues45,46 and Gottlob.47
Infants with MLN can often exhibit low intensity oscillations during binocular viewing, particularly if they have a type II or type III MLN (see Fig 6), whereas the oscillation becomes more noticeable during monocular viewing. The importance of the infant’s state of attention and arousal also needs to be borne in mind, since nystagmus is invariably more obvious when the infant is alert, upset, or tired.5 This leads us and others to promote the use of the term infantile nystagmus rather than congenital nystagmus as a more appropriate description of the presentation time2,42,43,48 although Dell’Osso49 has used the term “congenital” to denote that there exists a congenital predisposition for this particular instability of the ocular motor system.
Oculomotor behaviour
Differentiating a benign infantile nystagmus from an acquired nystagmus is often far easier with a cooperative older child or adult, where history and symptoms can be taken into account. An important feature of infantile nystagmus is the distinctive oscillations. They are frequently horizontal, with either accelerating slow phase velocities (CN) or decreasing slow phase velocities (MLN).1–7,22–27
A CN waveform was seen in 79% and 92% of the idiopath and albino groups respectively; 78% of the subjects with an MLN waveform were idiopaths. While there was a trend for the ocular anomaly group to exhibit a CN waveform (n = 14; 64%) they also show MLN or CN/MLN hybrid waveforms. That is, in our sample, MLN waveforms were more likely to be seen in subjects with ocular anomalies than in the other two groups (idiopaths and albinos). This finding has recently been supported by Gage and her colleagues44 in a study on infants with cataracts.
As stated earlier, the adult jerk nystagmus often maturates from a pendular, asymmetrical pendular, or triangular oscillation.5,43,46,47 On occasions subjects will initially exhibit saccadic intrusions or oscillations44–47 and the success of noticing MLN waveforms is dependent on the MLN type, their intensity, and whether one or both eyes are viewing.
Spatial nulls away from the primary or straight ahead position were not unusual. Generally, subjects will adopt a compensatory head posture if it is advantageous. Reasons include a discernable improvement in visual acuity or a minimisation of oscillopsia.30 Surgical intervention can be somewhat problematic, particularly if more than one head posture is used and there is a need to differentiate a subject with CN from one with MLN. Extraocular surgery on MLN patients to overcome an anomalous head posture is always performed on one eye only.29
Dynamic nulls were found in 17 out of 195 subjects (8.7%), 14 of whom were albinos. The large proportion of albinos with a periodic alternating nystagmus (14 out of 17; 82%) supports the finding that shifting nulls are common in this subject group. This view has previously been reported by Abadi and Pascal.32 Interestingly, Shallo-Hoffmann and her colleagues have recently reported that dynamic nulls were found in a group of seven out of 18 subjects who had idiopathic CN,33 a far larger occurrence than the three out of 195 that this case study revealed.
The prevalence of strabismus in our sample was significantly higher than one would expect to find in a non-nystagmus population—64% as opposed to 3.1%.50,51 Ocular misalignment has a clear coupling with MLN1,27,49 and since MLN occurs frequently in individuals who have congenital or uniocular vision loss, as well as those who have experienced visual deprivation, it has been proposed that disturbances of egocentric localisation may be, in part, responsible for these oscillations.24,25 Further evidence for this comes from studies on infants with infantile cataracts where the presence of an MLN appeared to be linked to the emergence of a squint.44
Sensory aspects
Visual performance is, in the main, dependent on three factors: firstly, the retinal image slip velocities, secondly, foveation, and, thirdly, the state of health of the eye and visual pathways. While many psychophysical functions have been measured by Abadi and his colleagues6,25,52–56 and Bedell and his group,57,58 most clinicians are, none the less, keen to know and to measure the resolution limit (that is, visual acuity). Consistent with results from other studies6,52–58 our idiopath group showed limited acuity losses (0.3 log units—that is, 6/12). Not surprisingly the albino and ocular anomaly groups showed greater acuity reductions, in the order of 0.6 log units (that is, 6/24). It is important to note that if subjects were to adopt a head posture in order to make use of an eccentric null then acuity levels can improve. Moreover, contour interaction56,57 and the effort to see can often reduce performance.5,59 In an effort to resolve these factors Dell’Osso has formulated a nystagmus acuity function to predict acuity levels.60
Oscillopsia
Over the years there have been a number of studies attempting to explain spatial constancy in infantile nystagmus. Explanations have included a reduced sensitivity to retinal image motion, adaptation to retinal image motion, information sampled only when the eyes are moving relatively slowly during the foveation periods and, finally, the use of extraretinal information to cancel the effects of eye movements (see Bedell61 for review). Since factors such as the variability of the nystagmus intensity and the absence of a textured background can influence spatial constancy to a large extent,62 care should be taken interpreting the responses and symptoms of patients.
Concluding remarks
Infantile nystagmus is not a common condition and may cause confusion and make interpretation difficult when time is limited in the clinic. Moreover, investigating a neonate or young infant can prove difficult. Objective, quantitative techniques often aid the differential diagnosis between benign forms of infantile nystagmus (CN and MLN) and those secondary to neurological disorders. The purpose of this case study was to describe the range of ocular motor behaviours and visual performances that have been found in 224 subjects with benign infantile nystagmus.
In over three quarters of subjects with infantile nystagmus, the oscillations were found to be conjugate and exclusively horizontal. The most common waveform was the accelerating slow phase jerk (that is, a CN), as opposed to the linear or decelerating slow phase (that is, an MLN). However, the two waveforms are not mutually exclusive since one in 20 subjects exhibited a mixture of the two. Both the CN and MLN waveforms were seen in idiopathic, albino, and ocular anomaly cases. Not one of the 224 subjects exhibited an LN, and it seems very likely that types II and III MLN are often mistaken for an LN (type I MLN). Occasional compensatory head postures are very common and reflect the gaze dependency of the nystagmus intensity. Constant head postures were always found in subjects who had null zones at, or beyond plus or minus 20°. Periodic alternating nystagmus is a usual accompaniment of albinism. The incidence of squints is very high and almost universal in the albinos and those subjects who had MLN. Indeed, MLN occurs frequently in those subjects who have congenital or uniocular visual loss or who have experienced visual deprivation.44 Visual acuity is clearly related to the duration and accuracy of the foveation period and around 40% of the subjects reported that they had experienced oscillopsia at some time.
Patients with ocular anomalies, as opposed to the idiopaths, represent a distinct and separate group and it is essential to search for the underlying sensory defect. While only 10% (n = 22) of our subjects belonged to this group, other hospital based studies suggest a far higher occurrence.63,64 Therefore systematic fundus and electrodiagnostic investigations are recommended to identify such conditions as Leber’s congenital amaurosis, optic nerve hypoplasia, and achromatopsia.2,3,48 Predictions of visual performance and the choice of low vision management are clearly dependent upon the nature of the sensory defect. Most will fall into the partially sighted category.65 On the other hand, the patient with idiopathic infantile nystagmus, because of a favourable waveform shape (that is, duration and accuracy of foveation), will rarely exhibit acuities below 6/15, although reaching the appropriate vision standards for driving can often prove problematical.
Two factors examined produced surprising results. Firstly, infantile nystagmus was not detected in a sizeable minority of our subjects (13%) until at least 6 months postnatally. Interestingly, Gresty and his colleagues have even reported three cases of infantile nystagmus not emerging until adulthood.66 That a nystagmus can present itself within such a broad time window suggests that there are likely to be a number of mechanisms underlying nystagmus.2–4,46,67–72 Secondly, around 40% of our subjects reported that they had experienced oscillopsia at some time. Recently, Abadi et al62 explored oscillopsia and tolerance to retinal image movement in idiopathic CN. They reported that perceptual stability may break down under a number of conditions, including viewing a small light in an otherwise dark room, during periods when the nystagmus intensity had substantially increased, or during a periodic alternating nystagmus. It is likely that observant subjects would be aware of these conditions.
In summary, it is clear that no single ocular motor diagnostic characteristic can differentiate the benign form of infantile nystagmus (CN and MLN) from the neurological. Rather the clinician must consider a host of clinical features. On the other hand, there are definite, strong, ocular motor and sensory patterns and associations that are indicative of an infantile nystagmus.
Acknowledgments
We would like to thank all our colleagues, Christine Dickinson, Jo Gage, Ellen Lee, Mark Lomas, Eric Papas, Eve Pascal, Columba Scallan, Jon Whittle, and Ralph Worfolk, who over the years have helped collect the information described in the text. Our subjects are also warmly thanked for their time, cooperation, and friendship.