Article Text

Abstract
Aims: To compare selective laser trabeculoplasty (SLT) and argon laser trabeculoplasty (ALT), in terms of intraocular pressure (IOP) lowering, in patients with open-angle glaucoma.
Methods: 176 eyes of 152 patients were enrolled in this study, 89 in the SLT and 87 in the ALT groups. Patients were randomised to receive either SLT or ALT treatment to 180° of the trabecular meshwork. Patients were followed up to 12 months after treatment. The main outcome measured was IOP lowering at 12 months after treatment, compared between the SLT and ALT groups.
Results: No significant difference (p = 0.846) was found in mean decrease in IOP between the SLT (5.86 mm Hg) and ALT (6.04 mm Hg) groups at 1 year or at any other time points, nor were there any significant differences in the rate of early or late complications between the two groups.
Conclusions: SLT is equivalent to ALT in terms of IOP lowering at 1 year, and is a safe and effective procedure for patients with open-angle glaucoma.
- ALT, argon laser trabeculoplasty
- IOP, intraocular pressure
- OAG, open-angle glaucoma
- PXG, pseudoexfoliation glaucoma
- SLT, selective laser trabeculoplasty
Statistics from Altmetric.com
- ALT, argon laser trabeculoplasty
- IOP, intraocular pressure
- OAG, open-angle glaucoma
- PXG, pseudoexfoliation glaucoma
- SLT, selective laser trabeculoplasty
Argon laser trabeculoplasty (ALT) has been used for intraocular pressure (IOP) lowering in patients with glaucoma for over 25 years. ALT was first described by Wise and Witter in 1979,1 and its effectiveness is well established.2
More recently, in 1995, a frequency-doubled, Q-switched, neodymium:yttrium aluminium garnet (Nd:YAG) laser was developed to lower IOP in patients with glaucoma.3 It has the benefit of using 80–100 times less energy than ALT, preserving the trabecular meshwork architecture in animal models, and being potentially repeatable.4 Selective laser trabeculoplasty (SLT) selectively targets melanin in trabecular meshwork cells.5
In relatively small trials published to date, ALT and SLT seem to have similar efficacy in terms of IOP lowering.6,7,8,9,10,11,12 The objective of this study was to compare SLT and ALT, in terms of IOP lowering, in patients with open-angle glaucoma (OAG), in an adequately powered, randomised, clinical trial.
METHODS
Inclusion and exclusion criteria
Approval was obtained from the Ottawa Hospital Research Ethics Board (Ottawa, Ontario, Canada), and all patients signed a consent form before enrolment. The protocol committee for this trial decided a priori to maximise the generalisability of this trial to the greatest extent possible. To this end, inclusion criteria were broad.
Patients included in this study were those referred to the glaucoma clinic at the University of Ottawa Eye Institute (Ottawa, Ontario, Canada). Patients were included if they had OAG (those with pseudoexfoliation glaucoma (PXG), pigmentary glaucoma or combined mechanism glaucoma were included as long as angles were open), uncontrolled IOP (⩾16 mm Hg) on maximum medical treatment or had failed previous 180/360 ALT (>6 months previously), were aged >18 years and had two sighted eyes. Maximum medical treatment was defined as all the drugs the patient was able to tolerate before consenting to have laser trabeculoplasty.
People with an advanced visual field defect within 10° of fixation; those who had previous glaucoma surgery, except for previous ALT or peripheral iridotomy; those with corneal disease where applanation would be inaccurate or the trabecular meshwork would not be adequately visible for gonioscopy or those using systemic steroids were excluded from the study.
Randomisation
Patients were randomised to receive either SLT or ALT treatment to 180° of the trabecular meshwork using standard treatment parameters.6,9 Randomisation was carried out in blocks of six to force reasonably equal numbers in each arm, using a computer-generated random number list to receive either ALT or SLT. A sequential opaque envelope technique was used. The continuous α-spending function of DeMets and Lans13 was used for the purpose of interim analysis; formal interim analysis was carried out after recruitment of every 25% of the patients.
Variables measured, treatment parameters and follow-up
Details of baseline data collected, treatment parameters for ALT and SLT, and follow-up visits were provided in earlier publications.6,9 All patients had IOP measurements recorded on at least two visits before the study. The IOP on the visit immediately preceding the SLT treatment was the one used in our analysis. IOP was measured by a certified ophthalmic medical technologist or a qualified ophthalmologist, using a calibrated Goldmann applanation tonometer. One IOP reading was taken and noted by the same person.
Laser treatment was carried out to the inferior 180° of the meshwork, unless the patient had received previous ALT to this area, in which case the superior portion of the meshwork was treated. All patients were pretreated with one drop of apraclonidine or brimonidine immediately before the laser treatment to prevent a postoperative IOP spike (defined as a rise in IOP of ⩾6 mm Hg 1 h after laser treatment). One hour after treatment the IOP was checked, and the anterior chamber reaction was noted (cells and flare were each graded on a scale of 0 to 4+).
All patients received prednisolone acetate four times a day for 5 days after treatment. Patients were maintained on the same drugs for glaucoma before and after laser treatment, to the extent that the treating doctor believed it was ethically possible.
Patients were followed up at 1 week, and 1, 3, 6 and 12 months after treatment. Visits occurred around the same time of day, whenever possible, to account for diurnal fluctuation in IOP.
In this paper, we have used the term enhancement of treatment to mean an eye that had previously been treated with 180° ALT and then received a further 180° of treatment during the study. Retreatment refers to an eye that had previously been treated with ⩾360° treatment of ALT and then received 180° of treatment to a previously treated area of trabecular meshwork.
Study administration
A protocol committee prepared all aspects of the study design; any changes of the protocol that occurred during the study were subject to this committee’s approval. An executive committee monitored all aspects of study execution, study reporting to scientific meetings and study summaries that have been given to regulatory agencies. The data safety and monitoring committee worked closely with, and was overseen by The University of Ottawa Research Ethics Board.
Outcomes and statistical methods
The primary outcome of this study was the IOP-lowering effect of SLT compared with ALT, at 12 months. The IOP measured at other time points was a secondary outcome. Other secondary outcomes included visual acuity, anterior chamber reaction, trabecular meshwork pigmentation grade and number of drugs used, which were recorded at all visits. Another secondary analysis was the “success” of the laser treatment. Successful laser treatment was defined as meeting all of the following criteria: (1) a reduction of ⩾20% of pretreatment IOP at 1 year after treatment; (2) no additional drugs needed over baseline; (3) no additional surgical treatment for glaucoma needed. This analysis was carried out to take into account patients who have needed additional drugs or further surgery beyond randomisation. They would be a failure even if IOP control was obtained.
For calculating the sample size, a clinically significant effect size difference was assumed to be 2 mm Hg. Variances for the sample size calculation were obtained from our pilot SLT versus ALT randomised clinical trial, published in the British Journal of Ophthalmology.6 α was assumed to be two tailed and 0.05. For a clinically relevant difference of 2 mm Hg and an assumed 10% withdrawal rate, 80% power required 135 eyes to be enrolled and 90% power required 184 eyes to be enrolled. The IOP measurements were compared at various time points after treatment.
The distribution of baseline characteristics was compared between the ALT and SLT groups. For normal continuous variables, appropriate Student’s t tests were used to detect statistical significance; for categorical variables, χ2 tests were used. Among exposure variables and covariates, values of p⩽0.10 or >25% difference between SLT and ALT groups were used in a multivariate generalised linear model with 1-year IOP difference between groups as the primary outcome. Both simple and clustered multivariate analyses were carried out and correlation between eyes was accounted for. Because results were so similar between univariate and multivariate analyses, only the univariate analysis is presented in this paper. All analyses carried out were intention-to-treat analyses—namely, once randomised to SLT or ALT, patients were analysed as randomised regardless of subsequent treatment changes or protocol deviations.
For patients lost to follow-up, IOP measurements were included only during the time they were still in the study. For binary outcomes (eg, laser success or failure), patients who failed were analysed to the point of failure, and successes were analysed to the end of follow-up. Patients who withdrew were censored at the time of withdrawal, as is standard for Kaplan–Meier survival analysis. All statistical analyses were carried out using the STATA V.7.0 software.
RESULTS
In all, 176 eyes of 152 patients were enrolled into the study and were randomised into the ALT and SLT groups. There were 0 of 89 patients with SLT and 2 of 87 patients with ALT who died during the first year of the study, and 11 of 89 patients with SLT and 10 of 87 patients with ALT lost to follow-up (fig 1). When comparing patients who were lost to follow-up with those who remained for the entire study, demographic and outcome variables were not statistically different between the two groups when compared in each arm of the study.

Outcome of randomisation and follow-up up to 1 year after treatment. ALT, argon laser trabeculoplasty; IOP, intraocular pressure; SLT, selective laser trabeculoplasty.
Nearly all baseline characteristics were similar between groups (table 1). We found a baseline difference in previous ALT treatments; however, multivariate results using previous ALT as a covariate showed results similar to our univariate analysis. We found no significant difference in mean IOP between the SLT (17.97 mm Hg) and ALT (17.88 mm Hg) groups at 1 year. Nor was there any difference at any other time points between the two groups (table 2).
Baseline characteristics
Mean intraocular pressure at various time points up to 1 year
The mean decrease in IOP at various time points was also similar between the two groups (table 3). Specifically at 1 year, the mean decrease in IOP in the SLT group was 5.86 v 6.04 mm Hg in the ALT group. The percentage of eyes that achieved at least 20% IOP lowering up to 1 year was similar between the two groups (table 4).
Decrease in intraocular pressure from baseline at various time points
Percentage of eyes that achieved ⩾20% decrease in intraocular pressure
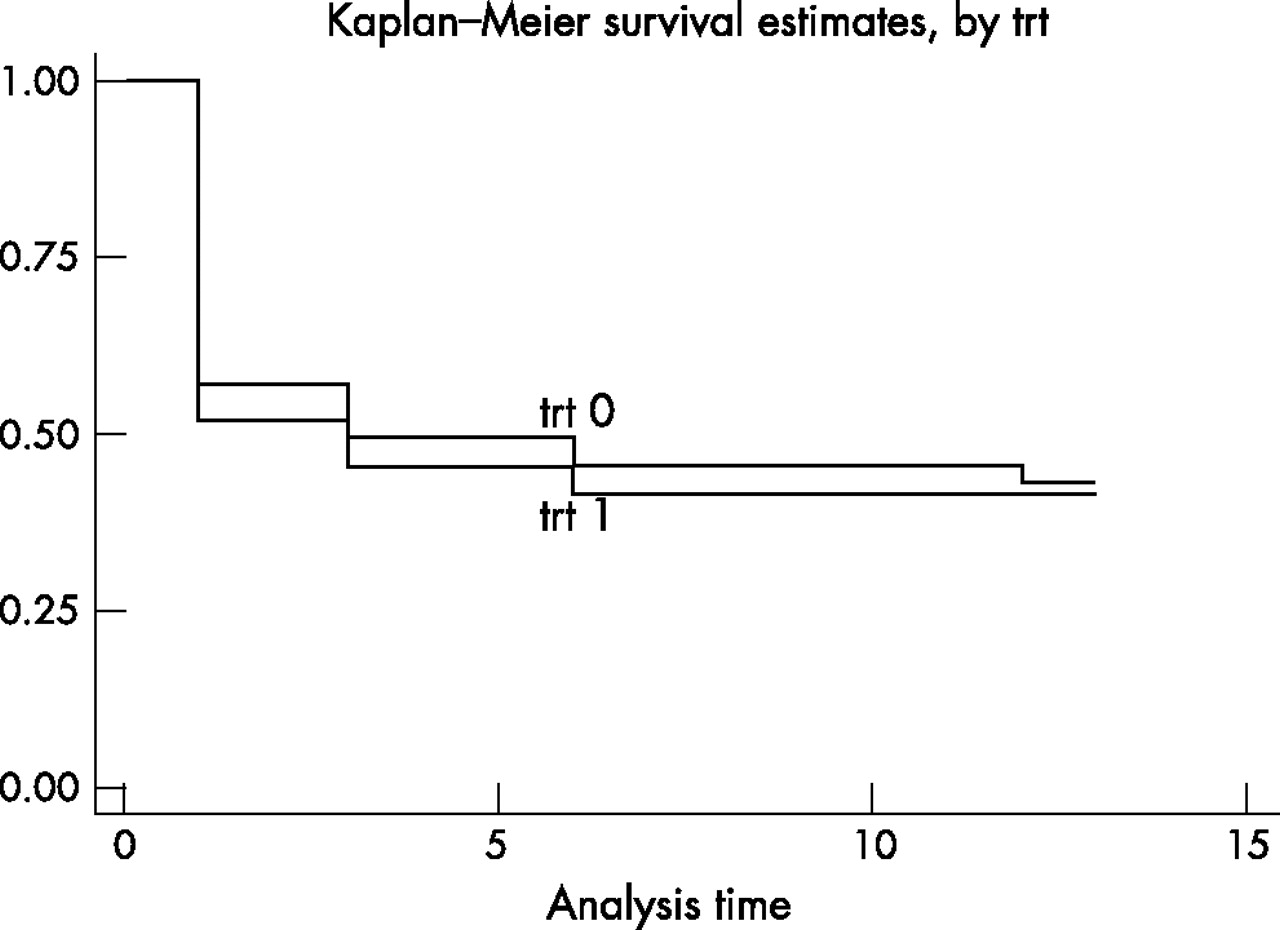
Using our definition of “success”, Kaplan–Meier survival curves (fig 2) also showed no significant difference between the two groups (p = 0.907).
{kind=link}
{kind=link}
Survival analysis Kaplan-Meier curve, analysis time = month. TRT, treatment; trt0, ALT; trt1, SLT.
We also carried out several smaller subanalyses. In PXG, the IOP decreased by 5.4 mm Hg in the ALT (n = 23) and by 5.7 mm Hg in the SLT (n = 16) groups on average, at 12 months after treatment, which is similar to what was seen in the overall group. In patients with pigmentary glaucoma, the IOP decreased by 3.4 mm Hg in the ALT (n = 3) and by 5.6 mm Hg in the SLT (n = 5) groups on average at 12 months. Baseline IOP was 24.3 mm Hg in the PXG group and 21.8 mm Hg in the pigmentary glaucoma group. No statistical analysis was carried out because the numbers in these groups were too small.
Table 5 presents the results of SLT and ALT in previously treated patients with ALT.
Reduction in intraocular pressure from baseline (mm Hg)
In the SLT group, those eyes that were retreated (previous 360° ALT treatment) seemed to have greater IOP lowering at 12 months than those who had enhancement (previous 180° ALT), or those who were naive to laser. In the ALT-treated group, those who were retreated had a slightly worse outcome compared with those who had enhancement, or who were naive to laser. Notably, the second columns of table 5A and B compared with each other show the results of SLT versus ALT in patients who were naive to laser (no previous ALT). We found no significant difference between SLT and ALT at any time point in the patients who were naive to laser.There were few adverse events in either group (table 6). During the course of the study, several changes were made in glaucoma medications to deal with adverse reactions to them or to keep IOP within the target range. At 1 year after treatment, 82% of eyes in the SLT group were maintained on the same number of drugs, and 18% had one additional drug. In the ALT group, 69% of eyes remained on the same number of drugs and 29% required one additional drug.
Number of eyes that incurred adverse events
DISCUSSION
In this study, we compared the IOP-lowering efficacy of ALT with SLT in a randomised clinical trial over 12 months, with a power of almost 90% for detecting a difference of 2 mm Hg between groups. We found no significant difference in mean IOP between the two groups at any time point, up to 1 year.
Few studies in the literature compare SLT with ALT, and no randomised, clinical trials have been published to the best of our knowledge, except for the early data from our current study, which was reported in the British Journal of Ophthalmology in 1999 and yielded similar results at 6 months for a sample of 36 eyes.6 One prospective study by Hollo et al,14 comparing ALT with SLT, compared decrease in IOP in 14 eyes, where one eye was treated with ALT and the other with SLT. This study showed equivalence between the two lasers, but the number of eyes studied was small. Another prospective study by Martinez-de-la-Casa et al7 treated consecutive patients with SLT (20 eyes) and ALT (20 eyes). They followed up these patients up to 6 months and found that reduction in IOP was similar. The only other comparative study published, to our knowledge, is a retrospective chart review by Juzych et al,15 which looked at 154 eyes treated with ALT and compared them with 41 eyes that underwent SLT. The result was a similar IOP-lowering response with both lasers.
When success was defined as a reduction in IOP of >20% at 1 year after treatment, SLT and ALT were equally effective in attaining this goal. In a separate paper, we examined various factors that may predict successful SLT response. Baseline IOP strongly predicted SLT success, whereas angle pigmentation did not.16
To increase the generalisability of our trial, we included a broad group of patients, including those with PXG and pigmentary glaucoma. Although larger studies are needed, it seems that SLT and ALT have similar IOP-lowering effects in both these types of OAG.
In both the enhancement and retreatment groups (patients with previous 180° or 360° ALT, respectively), there was a reasonable reduction in IOP noted with both ALT and SLT (range 19–29%). However, our numbers are too small to draw any definitive conclusions in this subgroup of patients, and thus these results should be considered exploratory and not definitive.
The amount of “cellular” reaction was significantly higher in the SLT group 1 h after treatment. These cells or particles were not present at 1 week or 1 month after treatment. One of our patients experienced a significant IOP spike after SLT and had underlying pigmentary glaucoma. Details of this case and other cases of patients (unrelated to this study) with heavy trabecular meshwork pigmentation, who developed intractable IOP spikes, are presented in a separate publication.17 Caution is thus recommended when considering SLT in a patient with a heavily pigmented trabecular meshwork. In this situation, if SLT is used, it may be worth reducing the power or treating less trabecular meshwork.
We found a limited number of changes in drugs, and in surgical and repeat laser interventions in the study patients. Such interventions are common in glaucoma trials, typical of clinical practice. We do not think these have affected our outcome, as the frequency of medical switches or additional interventions did not differ between the two groups, Moreover, a separate analysis looking at successful outcome in the absence of such interventions did not show a difference in either group (fig 2).
In summary, SLT is equivalent to ALT in terms of IOP lowering at 1 year, and is a safe and effective procedure for patients with OAG. Future studies with SLT will need to shed light on other important questions such as whether it is repeatable, whether it can be used effectively as a preferred treatment (instead of a drug), the optimum amount of angle to treat and whether it is as effective as ALT in pigmentary and PXG-related glaucomas.
Acknowledgments
Mr Harkaran Bains provided assistance in the early phases of this clinical trial.
REFERENCES
Footnotes
-
Published Online First 9 August 2006
-
Funding: Lumenis provided financial support for this study.
-
Competing interests: The authors have no proprietary interest in the Selecta 7000 laser or in Lumenis