Article Text

Abstract
Aims: To determine the characteristics of “non-responders” to intravitreal bevacizumab treatment in choroidal neovascularisation (CNV).
Methods: Forty-three patients with visual loss due to neovascular age-related macular disease (ARMD) (44 eyes) underwent intravitreal injections of 1.25 mg (0.05 ml) bevacizumab and were followed up every 4 weeks for 2, 3 or 6 months. Re-injection was performed when persistent leakage of the CNV was determined by fluorescein angiography and retinal oedema was assessed by optical coherence tomography (OCT). Non-responders were defined as those patients having reduced or stable visual acuity at the last follow-up.
Results: 45% of the patients were non-responders. In this group the initial CNV size was significantly larger than in the responders. Initial reading ability was significantly lower in non-responders, but the initial foveal oedema was similar in both groups. Gains in mean visual acuity and reading ability were independent of lesion type. The proportion of non-responders to responders in the different lesion type groups was equally distributed. Only patients with the classic type of CNV seemed to respond better.
Conclusions: In this study initial reasons for non-responders to intravitreal bevacizumab treatment in CNV are given. The efficiency of bevacizumab depends on initial lesion size and initial reading ability, but is independent of the amount of intraretinal and subretinal fluid. There was no general ineffectiveness of bevacizumab with any particular lesion type.
Statistics from Altmetric.com
The tools for the treatment of neovascular lesions of the choroid have changed considerably with the introduction of intravitreal treatment using vascular endothelial growth factor (VEGF) antagonists. In 2004 Gragoudas et al. showed that pegaptanib (Macugen), an RNA aptamer, which binds one isoform of VEGF (VEGF 165), was able to reduce the risk of visual acuity loss while a small percentage of patients gained or remained stable in visual acuity in comparison to the control group with placebo injections.1 More recent reports on VEGF antibodies (ranibizumab, Lucentis) have proven (the PIER and ANCHOR studies) that long-term improvement in visual acuity is possible.2
Initial reports on the intravitreal use of bevacizumab (Avastin), a full-size antibody related to ranibizumab, in patients with neovascular age-related macular disease (ARMD) have demonstrated a beneficial morphological and functional outcome and off-label use of bevacizumab has gained currency.3 4
Compared with previous treatment modalities such as photodynamic therapy (PDT), which allowed for a retardation of the disease process but rarely demonstrated an improvement of visual acuity, VEGF antagonists have raised the standards of treatment and can improve visual acuity. The proportion of patients with improving visual acuity has ranged from 28% to 43%.3 4
So far it is not known why more than half of patients do not improve after bevacizumab therapy and can be considered as non-responders according to the criteria used in this study.
In this prospective interventional case series we investigate the determinants of treatment “failures”, defined as patients who do not ameliorate with respect to visual acuity, compared to the baseline value.
MATERIALS AND METHODS
Forty-three patients with visual loss due to neovascular age-related macular disease (ARMD) (44 eyes) who were referred to the department of vitreoretinal surgery, at the University of Cologne, for treatment of choroidal neovascularisation (CNV) were included in the study. Of the 44 eyes, 16 (36%) had received some prior therapy, consisting of PDT, focal laser treatment or intravitreal triamcinolone injections. Twenty-eight eyes (63%) received intravitreal bevacizumab as primary therapy. All patients were treated at the department of vitreoretinal surgery and signed an informed consent for off-label use of bevacizumab.
The different lesion types consisted of 6 classic lesions, 16 occult or minimally classic lesions, 16 retinal angiomatous proliferation (RAP) lesions, 3 extrafoveal or parapapillary CNV, and 3 drusen with pigment epithelial detachment (PED). Sixteen eyes had PED accompanying their lesion type.
The follow-up period was 6 months in 24 eyes, 3 months in 18 eyes and 2 months in 2 eyes, with a median of 6 months, ranging from 2 to 6 months.
Treatment with bevacizumab (Avastin) and follow-up
Bevacizumab (1.25 mg, 0.05 ml) was injected intravitreally under sterile conditions via the pars plana. At each follow-up, after 4 weeks, 2, 3 or 6 months, re-injection was considered if vascular leakage was still present on angiography or retinal thickness was increased due to intraretinal oedema or subretinal fluid accumulation. After each injection and at each follow-up intraocular pressure was measured and slit-lamp investigation was performed for signs of inflammation.
Visual acuity
Best corrected visual acuity and reading ability at baseline and the last follow-up examination (after 2, 3 or 6 months) were compared. Improvement was considered as any gain in vision.
Non-responders were defined as follows:
reduction in both visual acuity and reading ability at the last follow-up
reduction in either visual acuity or reading ability at the last follow-up
no change in either visual acuity or reading ability at the last follow-up.
As an example, a patient who gained in reading ability but stayed stable in visual acuity was considered a non-responder. If compared to most other studies, this is a very strict criterion as most studies define stabilisation of visual acuity as a successful outcome.
Best corrected visual acuity testing was performed according to the Early Treatment Diabetic Retinopathy Study protocol preoperatively and at each follow-up visit.5
Reading performance was measured by a standardised reading test according to Radner.6 7
Fluorescein and ICG angiography
Fluorescein angiography and indocyanine green angiography were performed using the HRA 2 (Heidelberg Retina Angiograph 2, Heidelberg Engineering GmbH, Dossenheim, Germany) to recognise any recurrent CNV present. Grading of the angiographies was done according to the TAP criteria.8
The size of the lesion (largest diameter) was measured on a frame on the middle phase fluorescein angiogram, thus excluding leakage in later phases. Patients with drusen and PED were excluded from this calculation.
Optical coherence tomography
Optical coherence tomography (OCT) was used to detect macular oedema, subretinal fluid accumulation and pigment epithelial detachment (OCT3, Version 4.0; Zeiss-Humphrey, Oberkochen, Germany). In patients with PED the diagnosis was confirmed both by angiography and OCT.
Data analysis and statistical methods
Statistical analysis was performed using the Wilcoxon and Mann–Whitney tests. Statistical significance was defined as p<0.05. Commercially available software (SPSS, version 12.0) was used for statistical analysis.
RESULTS
No endophthalmitis, increased intraocular pressure, retinal tears or retinal detachment occurred during the observation period. In one patient with previous PED, a retinal pigment epithelium (RPE) rupture was observed. Fifteen eyes were injected once, 19 eyes twice, 9 eyes three times and 1 eye four times. One patient had bevacizumab injected into both eyes. The mean interval between each injection was 4 weeks.
Overall change in mean visual acuity and reading ability
The mean visual acuity of all 44 eyes improved significantly from 0.65 logMAR to 0.60 logMAR (p = 0.023), and the mean reading ability of all 44 eyes improved significantly from 0.70 logRAD to 0.48 logRAD (p = 0.01) (fig 1).

Non-responders
Twenty out of 44 eyes (45%) were considered not to respond to bevacizumab, having a reduction or no change in either visual acuity or reading ability. Eleven eyes (25%) had a reduction in both visual acuity and reading ability, and nine of these eyes (20%) had a reduction or no change in either visual acuity or reading ability at the last follow-up in comparison to the baseline examination. All 11 eyes (25%) with a loss in visual acuity lost more than five letters. The mean reduction was 0.22 logMAR. Three eyes showed a loss of more than 15 letters in visual acuity.
Subgroup analysis
Both groups (responders and non-responders) were similar with respect to the duration of follow-up (4.4–4.6 months), the duration after the last injection (3.6–3.3 months) and the number of total injections (1.9–2.0).
Type of CNV
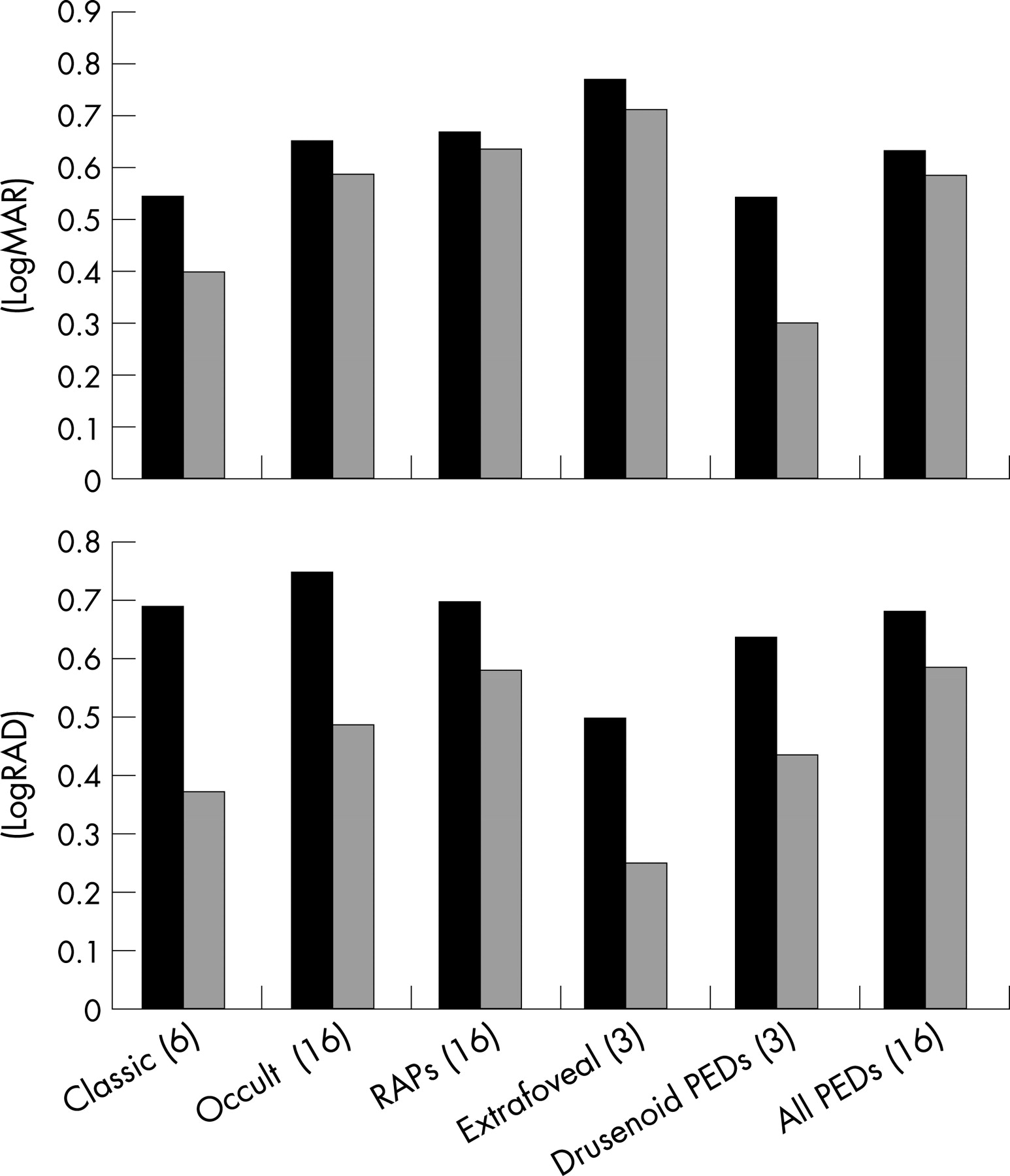
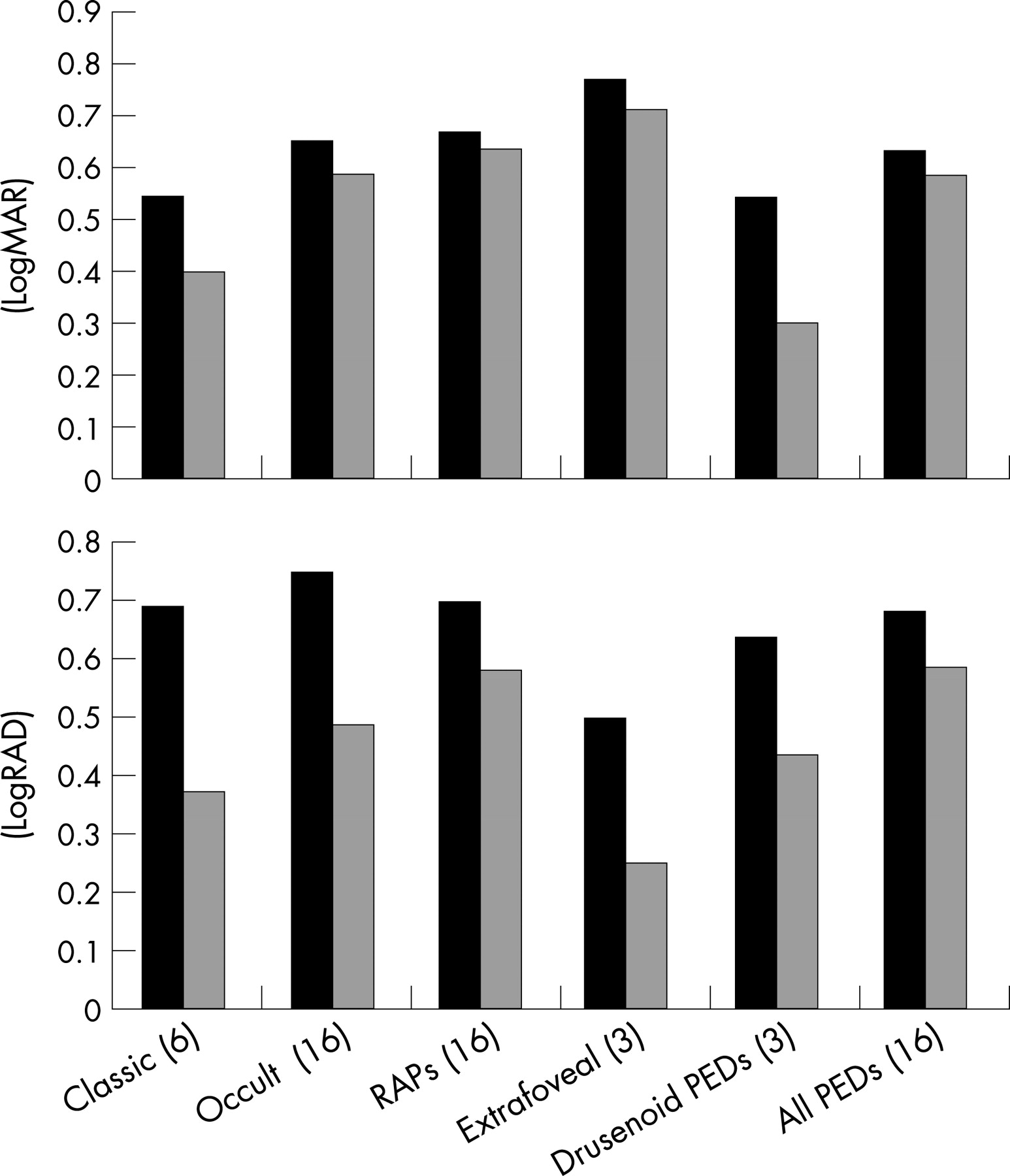
If the different lesion types are looked at, every single group improved in both mean visual acuity and mean reading ability (fig 2). The classic type CNV group improved in mean visual acuity from 0.54 logMAR to 0.4 logMAR; of the six patients in this group, five responded while one did not respond. Except for this group, the proportion of non-responders to responders in the different types of CNV was equally distributed (nearly 1:1) (figs 3 and 4).


Initial CNV size
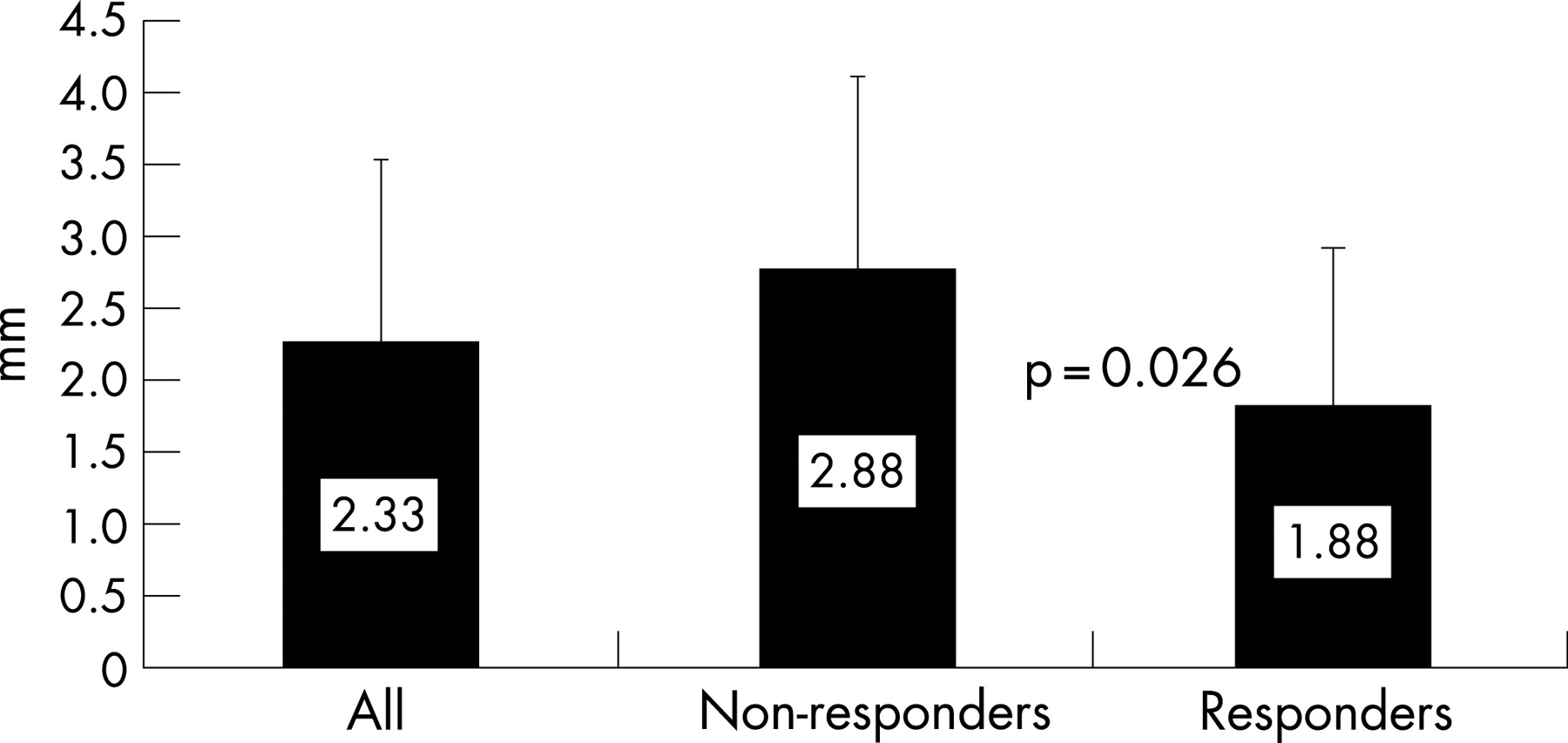
The initial size of the CNV, measured on angiography, was significantly larger in patients who later failed to respond: 2.88 mm in the non-responder group in comparison to 1.88 mm in the responding group (p = 0.016) (fig 5).

Initial reading ability and visual acuity
Initial reading ability was significantly lower in patients who later failed to respond: 0.814 logRAD in the non-responder group compared to 0.604 logRAD in the responding group (p = 0.041) (fig 6). The initial visual acuity was also lower in the non-responder group, though this difference was not statistically significant: 0.71 logMAR vs 0.60 logMAR (p = 0.109) (fig 6).

Initial foveal oedema
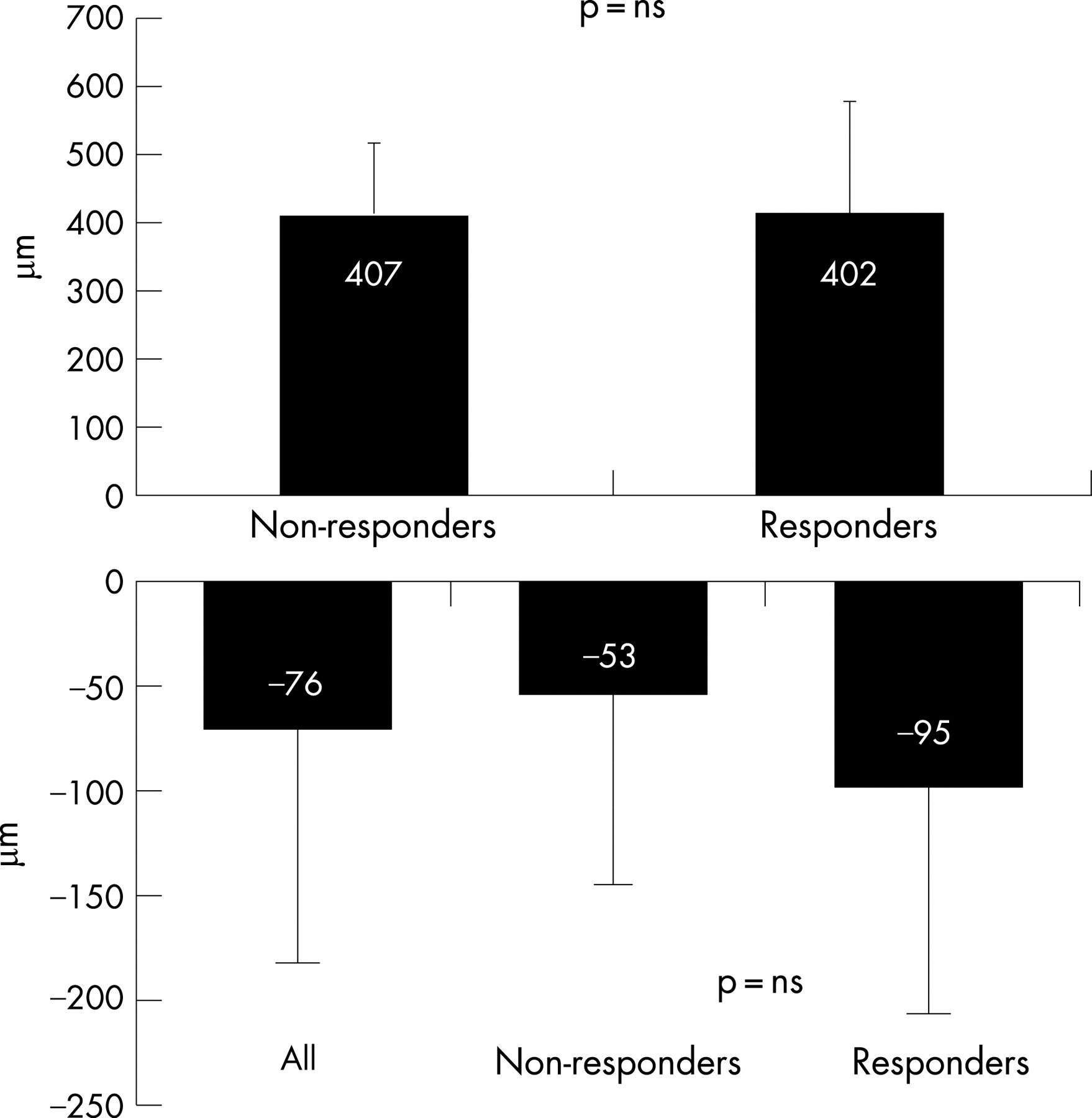
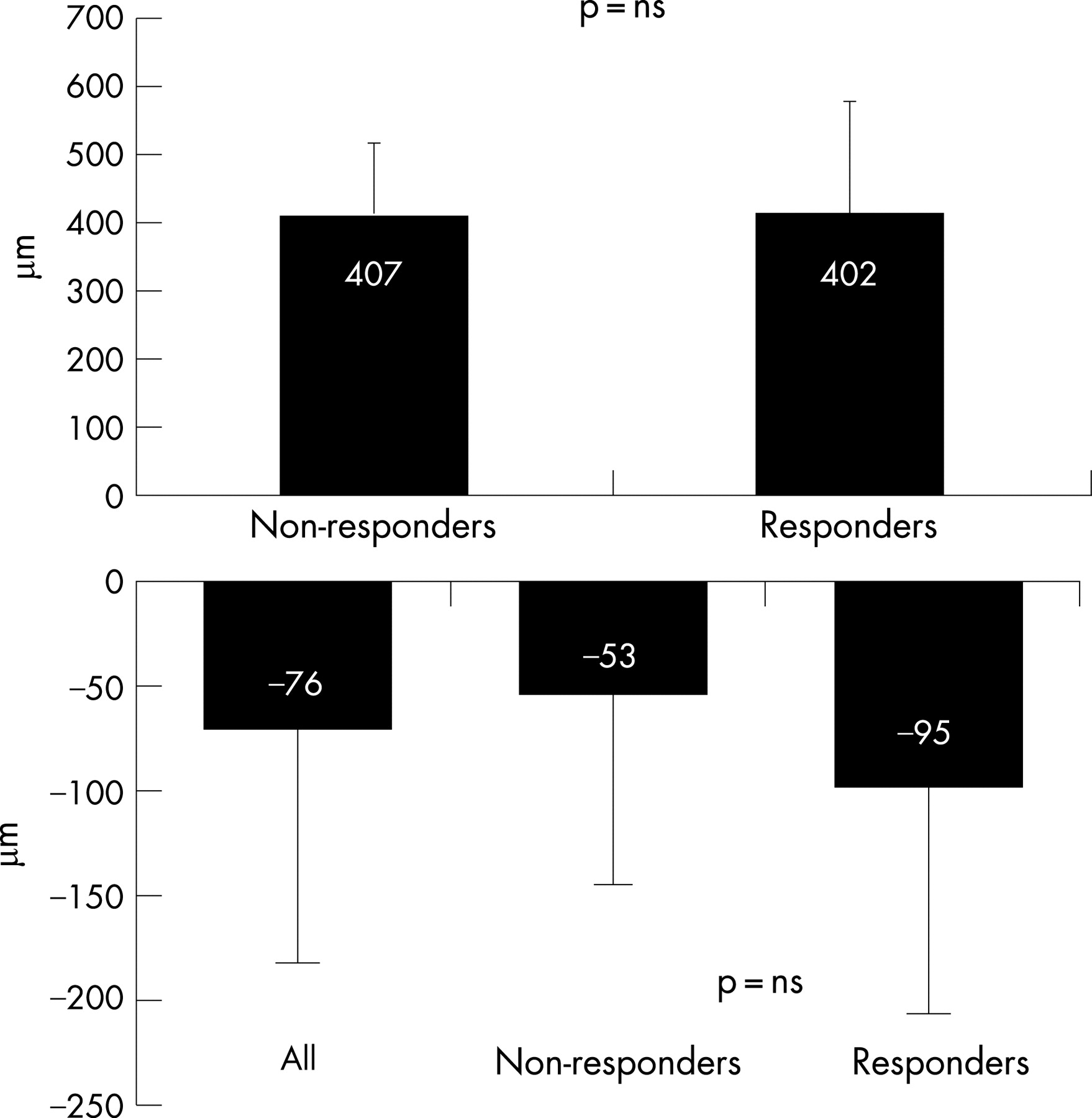
Initial foveal thickness was similar in both groups (407 μm vs 402 μm, p = 0.980), while the reduction of foveal thickness was greater in patients who responded, though the difference was not statistically significant: −53 μm in non-responders compared with −95 μm in responding patients (p = 0.157) (fig 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In this study 45% of the patients were considered non-responders, showing a significantly larger CNV size and a significantly lower initial reading ability. Non-responders to bevacizumab were defined as patients not improving in visual acuity compared to the baseline value. The large-scale studies on VEGF inhibitors (eg, the MARINA and ANCHOR studies) in neovascular ARMD have raised expectations and a successful outcome is now considered an improvement in visual acuity.2 9 This is in contrast to previous studies on PDT, which considered any stabilisation to be a successful outcome in contrast to the deterioration of the non-treated control group (TAP study).8 In response to these raised expectations in the therapy of CNV, we decided to apply the strict criteria as outlined above.
Since the introduction of anti-VEGF in the therapy of CNV in ARMD and its proven ability to ameliorate vision, there have been innumerable reports with promising percentages of responders.10–12 So far no study has focused on the still high proportion of non-responders to anti-VEGF therapy and the possible reasons underlying this. In this study initial reasons for non-responders to intravitreal bevacizumab treatment in CNV are given.
The proportion of non-responders in our study agrees with the findings in recent studies by Ladewig et al. and Rich et al., who reported improvements in 28% and 43% of patients, respectively.3 4 The proportion of non-responders in these studies, if defined according to our criteria, approximates to 50%.
Comparisons with published studies are difficult, as not only is case selection different but so are criteria for positive or negative change in vision. Thus, defining the proportion of non-responders in the MARINA and ANCHOR studies according to our criteria is not completely possible, as they both only report the proportion of responders improving by more than 15 letters. This proportion is 24.8–33.8% (0.3 mg, 0.5 mg ranibizumab) in the MARINA study and 35.7–40.3% (0.3 mg, 0.5 mg ranibizumab) in the ANCHOR study.2 9 Conversely, the proportion of patients with deterioration or stable visual acuity is between 59% and 75%. According to the criteria of the MARINA and ANCHOR studies, we have 14% of patients with a gain of more than 15 letters, and hence 86% deteriorating or stable patients. Comparing the proportion of patients with severe vision loss, defined as a loss of 30 letters or more, the findings of our study with a proportion of 2% are similar to those of the MARINA and ANCHOR studies (0.8–1.2% and 0%). Nevertheless, the proportion of patients in our study losing 15 letters or more is considerably high at 9%.
Our study shows that the efficiency of bevacizumab depends on initial lesion size. In patients with a large initial CNV size the prognosis of a visual improvement is reduced. This agrees with the findings of the TAP study, which showed an efficiency of PDT depending on the lesion size.8 The lower responsiveness to either treatment may be attributable to the fact that these larger lesions either have a greater amount of fibrosis or that less viable RPE is left.
The stage of the disease at the initial presentation can be considered a prognostic factor. Non-responders showed a significantly lower initial reading ability. Thus, a low initial function associated with a lack of recent disease progression, indicating long-standing disease, is a limiting factor on treatment efficacy with bevacizumab.
In contrast, the responsiveness to bevacizumab is shown to be independent of the initial foveal oedema, although its effect seems to be correlated with a reduction of foveal oedema. The initial foveal oedema was similar in both groups, while the responders showed a slightly higher reduction in foveal thickness after bevacizumab therapy. Anti-VEGF is known to reduce the vascular permeability and in this way reduces oedema.13 This may lead to an improvement in visual acuity. In advanced lesions the chronic intraretinal and subretinal fluid has already caused irreversible damage to the cells, so that a resolution of the oedema has no effect on visual acuity.
Bevacizumab efficiency is independent of lesion type. Interestingly, there was no lesion type where bevacizumab was generally ineffective. All the different lesion type groups gained in mean visual acuity and reading ability, with an equally distributed proportion of non-responders to responders. The classic type of CNV was shown to have a good prognosis of visual improvement with bevacizumab therapy. This is in accordance with the phase III reports on ranibizumab and pegaptanib of an effectiveness of VEGF antagonists independent of lesion size, lesion type and initial level of visual acuity (Gragoudas et al., MARINA study, ANCHOR study).1 2 9 Nevertheless, our study results differ with regard to the efficacy of bevacizumab on the lesion size and the initial visual acuity or reading ability.
This study is a prospective, non-randomised case series. Thus, the results cannot be generalised for several reasons. In the study the time period between the last follow-up and the last injection of bevacizumab was different for each patient. It is thus possible that a patient with a long interval between the last injection and the last follow-up will demonstrate a low visual acuity at the last follow-up, despite having had better vision before, while in a patient whose last follow-up is 4 weeks after the last injection bevacizumab is still effective. Similarly, it is still not known at what intervals bevacizumab should be injected. In our study the mean interval between the last injection and the last follow-up evaluated in the study did not differ between the two groups: 3.3 months in the non-responder group vs 3.6 months in the responding patients. The number of total injections was also similar in both groups: 2.0 vs 1.9. This indicates that the reasons for non-responding found in our study are not influenced by different intervals between treatment and last follow-up or by the number of injections.
The question remains what to do with the non-responders. Should we consider a patient who does not improve in visual acuity after the first injection a non-responder? For how long should we re-inject them? Further studies are needed to investigate whether patients who do not respond in visual acuity or retinal thickness after the first injection have a chance to get better with the second or third injection at all and whether there is any scope for ameliorating the result by a combination with PDT.
In this study initial reasons for non-responding to intravitreal bevacizumab in choroidal neovascularisation are given, although this small group and short-term follow-up only allow for cautious conclusions to be drawn. Yet it does not leave clear inclusion or exclusion criteria for the intravitreal injection of anti-VEGF drugs. The prediction of which patient will respond to bevacizumab and which will not is still not possible. So far the only criteria which can be relied on are leakage of the CNV during angiography and retinal oedema in the OCT imaging. Randomised clinical trials with long-term follow-up are required to determine further reasons for bevacizumab non-responding.
Acknowledgments
We would like to thank Mr Manuel M Hermann for his help with the statistical analysis. Erica Menrath and Sandra Joeres helped with the investigation of the patients.
REFERENCES
Footnotes
Funding: This study was supported in part by Deutsche Forschungsgemeinschaft (DFG) grant Jo 324/6–2, the Brunnenbusch-Stein Stiftung, and the RetinoVit Stiftung, Cologne.
Competing interests: None.
- Abbreviations:
- ARMD
age-related macular disease
- CNV
choroidal neovascularisation
- OCT
optical coherence tomography
- PED
pigment epithelial detachment
- PDT
photodynamic therapy
- VEGF
vascular endothelial growth factor