Article Text

Abstract
Aim: To evaluate the long-term efficacy and safety of trabeculectomy with or without low-dosage Mitomycin-C (MMC) in primary open-angle glaucoma (POAG).
Methods: 114 patients affected by POAG, participating in a randomised clinical trial from 1995 to 1998, were re-examined and their chart reviewed. Patients had undergone in one eye a trabeculectomy with intraoperative application (2 min) of MMC (0.2 mg/ml) or balanced saline solution (BSS), and, if indicated, postoperative laser suture lysis, bleb needling and/or digital massage. Intraocular pressure (IOP), medical therapy, visual field, further glaucoma surgery, cataract surgery and complication rate (leakage, cataract progression, hypotony, blebitis, endophthalmitis) were evaluated.
Results: 67 eyes had received MMC and 47 BSS. MMC-treated eyes had a lower mean IOP (13.33±3.35 vs 14.72±2.19 mm Hg, p = 0.014); in this group, an higher percentage of eyes had IOP⩽18 mm Hg (73.1% vs 51.1%, p = 0.027) and IOP⩽14 mm Hg (56.7% vs 31.9%, p = 0.015); a lower rate had further glaucoma surgery (9% vs 25.5%, p = 0.040), and visual-field damage progression (21.1% vs 48.6%, p = 0.009). No difference was seen in the complication rate: one MMC-treated eye developed blebitis.
Conclusions: In POAG low-dose MMC with intensified postoperative management improved the outcome of the trabeculectomy with a low incidence of complications.
Statistics from Altmetric.com
Antiproliferative agents increase the success rate of glaucoma surgery by reducing scarring at the filtration site.1 Mitomycin C (MMC), in particular, is widely used because of its easy intraoperative application (in different concentrations and durations),1 efficacy and good acceptance by patients.2
In trabeculectomy at high risk of failure, the use of MMC is diffuse.3 4 In trabeculectomy for primary open-angle glaucoma (POAG) without adjunctive risk factors, MMC allowed a high success rate,5–9 but since late complications (hypotony, hypotony maculopathy, bleb leakage, blebitis, endophthalmitis)10 12 can occur 3–4 years after the surgery because of late thinning of the bleb, it was concluded that “the routine use of MMC cannot be considered appropriate.”11
However, most studies have been retrospective, and the definition of success has varied, often considerably; different concentrations of MMC (0.1–0.5 mg/ml) and exposure times (1–5 min) have been used, and side effects appear to occur more frequently with higher MMC dosages (0.4–0.5 mg/ml),9 10 than with low dosages and exposure times.8 13 In a previous study, we found that, after 5 years’ follow-up, trabeculectomy with low-dosage MMC has better efficacy and no increased incidence of side effects compared with trabeculectomy without antiproliferative agents.6
In this study we evaluated the efficacy and safety of primary trabeculectomy with low-dosage MMC in POAG, compared with trabeculectomy without antiproliferatives, in a group of subjects followed up for at least 9 years.
MATERIAL AND METHODS
In the Eye Clinic of the University of Catania, Italy, from April to November 2007, we recalled and re-examined a group of patients who, from March 1995 to October 1998, had been included in a randomised clinical study.
Consecutive patients eligible for a trabeculectomy had been enrolled: all were aged over 50 years, were affected by POAG uncontrolled by maximal tolerated therapy (intraocular pressure (IOP) >21 mm Hg), had no advanced glaucomatous damage (Hodapp classification: −6 dB<mean deviation (MD)<−12 dB, without absolute (0 dB) defect in the central 5°),14 and visual acuity >0.4 (refraction between −5 D and +2 D). One eye of each patient was included in the study. Patients with previous ocular inflammation, trauma or surgery, and patients with pigmentary, pseudoexfoliative and normal-tension glaucoma were excluded. Patients with diabetes were also excluded, because of the possible effects of diabetic retinopathy on the visual field.
Trabeculectomy surgery was done by two surgeons (AR, MGU), with the same surgical technique. All patients were randomised to receive trabeculectomy with intraoperative application of 0.2 mg/ml MMC or balanced salt solution (BSS) for 2 min (ratio: three MMC, two BSS). Under retrobulbar or peribulbar anaesthesia, a limbus-based conjunctival flap was prepared superiorly with an incision 10–12 mm posterior to the limbus, and then a half-thickness square scleral flap (approximately 4×4 mm) was dissected. A thin cellulose sponge (approximately 6×4 mm) soaked with MMC (0.2 mg/ml) or BSS was placed over the scleral flap for 2 min, then the area was precisely washed with BSS for 1 min, and trabeculectomy (approximately 2×1 mm) and basal iridectomy were performed. The scleral flap was sutured with five 10-0 nylon sutures. The conjunctiva and Tenon capsule were closed with a continuous suture of 8-0 Vicryl. Finally, a subconjunctival injection of betamethasone and tobramycin was given 180° away from the bleb. After the surgery, patients received topical corticosteroid three times a day and atropine twice a day for 4 weeks, and systemic antibiotic and steroid treatment (betamethasone 4 mg for 3 days and 1.5 mg for 4 days) for 1 week.
For the first 6 months postoperatively, all patients were followed at the Glaucoma Centre. Then, most had follow-up visits at the Centre two or three times a year; the others, referred to other ophthalmologists, were re-examined at the Centre annually. Postoperative management included laser suture lysis (in the first two postoperative weeks, if IOP>16 mm Hg), needling in case of an encapsulated bleb (repeated if necessary) and digital ocular massage (recommended to all the patients, unless the IOP was less than 12 mm Hg or the bleb was thin or leaking).
In eyes that underwent cataract surgery, at least 6 months after trabeculectomy, phacoemulsification with a posterior chamber intraocular lens and a temporal or nasal clear-corneal approach were used, with care to avoid trauma to the bleb.
At the study visit, and retrospectively from the clinical chart, we evaluated: IOP, visual-field damage progression, postoperative procedures, complications (bleb leakage, hypotony, hypotony maculopathy, infective blebitis or endophthalmitis), cataract progression, cataract surgery, hypotonising medical therapy and further glaucoma surgery.
IOP was measured with an applanation Goldmann tonometer. The visual field was tested by automatic computerised perimetry (24-2, full-threshold, HFA-I and HFA-II, Humphrey Field Analyzer; Carl Zeiss, Jena, Germany). Before surgery, all patients had a reliable visual field; the visual fields were performed also during the following years and at the study examination. Visual fields were considered reliable when the rates of fixation loss, false-positive errors and false-negative errors were lower than 20%.
The criteria of the European Glaucoma Society were used to assess the progression of visual-field damage. It was considered as significant if there was:14
-
a new defect in previously normal area: a decrease of 5 dB (or a decline at a p<5% level) compared with baseline in a cluster of three non-edge points, or a decrease of 10 dB in a single point;
-
a deepening of a pre-existing defect: a decrease of 10 dB (or a decline at a p<5% level) compared with baseline in a cluster of three non-edge points;
-
an expansion of a pre-existing scotoma in contiguous points: a decrease of 10 dB (or a depression at a p<5% level) compared with baseline in two previously normal points within the central 15°, or three points outside the central 15°.
-
a generalised depression: a decline in MD at p<1% level (or of 3 dB in all points) not explained by media opacities or pupil size, or a corrected pattern standard deviation (CPSD) showing an obvious trend (this latter based on at least five consecutive visual fields).
Cataract progression was determined from the descriptions in the clinical chart. Bleb leakage was determined at the slit lamp, with fluorescein and blue cobalt filter, without ocular massage (spontaneous leakage). Hypotony was defined as IOP<6 mm Hg. Hypotony maculopathy was defined as loss of visual acuity with macular folds, without vascular leakage.
Ophthalmologists performing physical examination, IOP measurements or evaluating the visual fields were masked as to the treatment used.
STATISTICAL ANALYSIS
The IOP value, the number of eyes treated by medical therapy or that had further glaucoma surgery, postoperative procedures and long-term complications were considered. For statistical analysis, the t test and χ2 test were used. Kaplan–Meier survival analyses were applied to assess the long-term outcomes in the two groups, and survival curves were compared by the logrank test. Cox proportional-hazards regression analysis was used to determine whether any factor predicted failure (age, refraction, baseline IOP, number of baseline medicines, previous argon laser trabeculoplasty (ALT), laser suture lysis, needling, and cataract surgery). p Values <0.05 were considered significant.
RESULTS
One hundred and thirty-three patients who had trabeculectomy were included in the study (77 treated with MMC and 56 with BSS). Nineteen patients (14%), 10 treated by MMC-TE (13%) and nine by BSS-TE (16%) were lost to follow-up. The main reasons were: death (n = 6), severe systemic disease (n = 3) and change of address (other town) (n = 5); we were not able to find five patients.
We re-examined 114 patients (114 eyes), 67 treated with MMC and 47 treated with BSS. The mean (SD) follow-up was, respectively, 127 (12) months (range 148 to 108) and 125 (13) months (range 148 to 108) in the two groups. No significant difference was seen between the two groups in preoperative age, IOP, number of medicines or the rate of eyes previously treated with ALT (table 1).
At the study visit, mean IOP was lower in eyes treated with MMC (t test p = 0.014). A higher percentage of eyes treated with MMC had IOP⩽18 mm Hg (χ2 p = 0.027), IOP⩽16 mm Hg (χ2 p = 0.019) and IOP⩽14 mm Hg (χ2 p = 0.015). No difference was seen in the percentage of eyes treated with antiglaucoma topical therapy. In the MMC group, a lower rate of eyes with visual-field worsening (χ2 p = 0.009) or that underwent further glaucoma surgery (MMC-TE 0.4% for 4 min) (χ2 p = 0.040) was found (table 2).
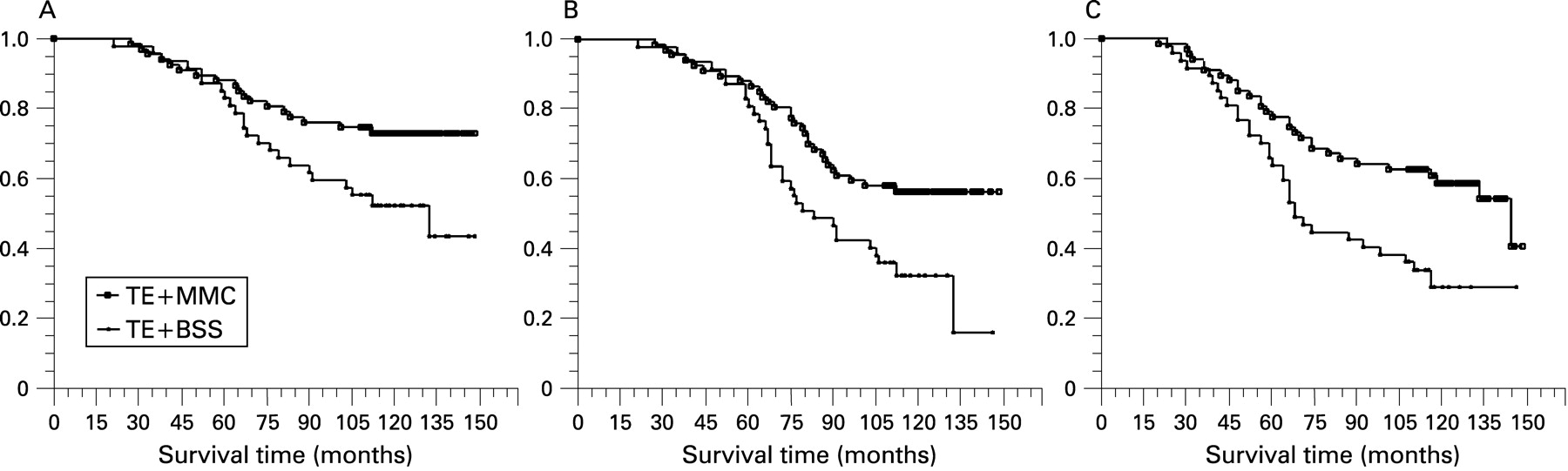
Figure 1 shows the results of Kaplan–Meier survival analyses for eyes treated with MMC and BSS. The success rates (SE, with 95% CI) estimated were respectively:

{kind=link}
-
74.63 (5.32)% (CI 0.63 to 0.83) and 55.32 (7.25)% (CI 0.41 to 0.69) for IOP<18 mm Hg without medication;
-
58.21 (6.03)% (CI 0.46 to 0.69) and 36.17 (7.01)% (CI 0.24 to 0.50) for IOP<14 mm Hg;
-
62.69 (5.91)% (CI 0.51 to 0.73) and 36.17 (7.01)% (CI 0.24 to 0.50) for visual-field stability.
The logrank test showed significant differences between the two groups in all the three parameters investigated (p = 0.019, p = 0.007 and p = 0.003, respectively).
No significant difference was found in the rate of eyes that received postoperative procedures (table 3) and in the incidence of late complications (table 4).
In the MMC group, one eye had blebitis (1.5%), and two other eyes had leakage (3%) (in one eye with hypotony) that resolved with subconjunctival autologous bleb injection laterally to the bleb, ointment and eye patching. No eye developed endophthalmitis. The Cox proportional-hazards model failed to show predictive factors for failure.
DISCUSSION
In this study we evaluated the long-term outcome of MMC-TE compared with BSS-TE; we found, in MMC-treated eyes, higher percentages of eyes with lower IOP, and lower rates of visual-field worsening and of further glaucoma surgery, without any significant difference in the incidence of late complications.
The aim of glaucoma therapy is to stop (ideally) or reduce the progression of glaucomatous damage. Large decreases in IOP and low IOP levels are required: the Collaborative Initial Glaucoma Treatment Study showed, in eyes with initial damage, that an IOP decrease ⩾30% reduces the visual-field worsening after 5 years;15 the Advanced Glaucoma Intervention Study (AGIS) investigators showed less worsening of the visual field (over 6 years) in eyes with a lower early average IOP (<14 mm Hg vs >17.5 mm Hg), and in eyes with a more stable IOP (IOP<18 mm Hg at 100% of the visits vs IOP<18 mm Hg at 50% of the visits).16 Moreover, the IOP target should be lower when the glaucomatous damage is more advanced.14
The use of MMC has led to a high long-term success rate for trabeculectomy: in juvenile glaucoma, success (IOP⩽21 mm Hg without or with therapy) was reported at 5 years in 73–91% of eyes treated with MMC 0.5 mg/ml for 2 min vs 54–73% for trabeculectomy without antiproliferative agents.17 In POAG, success (IOP<15 mm Hg) was obtained in 60% of eyes (treated with MMC 0.2 mg/ml for 3 min) at 6 years;7 at 8 years, cumulative survival rates of 67% and 44.5%, respectively, were reported for IOP<18 mm Hg and IOP<16 mm Hg, in a group of 123 eyes treated with MMC 0.4 mg/ml for 3 min.9 Also, in 292 eyes treated with MMC 0.3 mg/ml for 1–3 min, 3-year success rates of 64%, 56% and 46% were found, respectively, for three criteria (IOP⩽18 mm Hg and IOP reduction ⩾20%; IOP⩽15 mm Hg and IOP reduction ⩾25%; IOP⩽12 mm Hg and IOP reduction ⩾30%).8
With regard to the visual field, worsening was found in 27% of eyes with advanced damage treated with MMC.7 In trabeculectomy without antiproliferative agents, Parc et al reported that 47% of eyes had gone blind after 10 years;18 others found a VF worsening in 41%19 and 46% of eyes;20 and in a large series (700 trabeculectomies), long-term success (IOP<21 mm Hg, no worsening of the visual field and no loss of visual acuity) was found in 44.4%.21
In spite of the results obtained with MMC, its use in trabeculectomy for POAG is not always advised, because of concern about late complications. MMC reduces the proliferative phase of wound healing by inhibiting fibroblast and endothelial cell growth and replication.1 Eyes treated with MMC have a thinner bleb, with a greater risk of late-onset leakage, blebitis or endophthalmitis.22
In long-term studies, Beckers et al reported blebitis in two eyes (3.3% of 60 eyes treated with MMC 0.2 mg/ml for 3 min), and bleb reconstruction in five eyes (two with leakage, two with bleb-related complaints and one with hypotony);7 DeBry et al, in 225 eyes, treated with MMC 0.5 mg/ml for 0.5–5 min, with a mean follow-up 2.7 years, found bleb leakage in 20 eyes (8%), of which 15 cases resolved with office-based methods; five eyes (2%) had an episode of blebitis, and eight eyes (3%) an episode of endophthalmitis.12
Higher rates of complications were reported by Blindish et al (123 eyes): hypotony (IOP<6 mm Hg) in 42.2% of the eyes, hypotony maculopathy in 8.9%, bleb leakage in 14.6%, blebitis in 5.7%, and endophthalmitis in 0.8%. Most of these complications occurred between 27 and 33 months after operation.10 These results led to the conclusion that the incidence of complications could have been seriously under-reported, and, since standard trabeculectomy usually gives an IOP around 15 mm Hg, in primary trabeculectomy “the routine use of MMC cannot be considered appropriate.”11 Most patients were treated with a high MMC concentration (0.5 mg/ml in 88 patients) and exposure time (0.75–5 min), but hypotony occurred in one of eight patients (12.5%) treated with MMC 0.2 mg/ml for 2 min as in our study.
More recently, with the use of MMC 0.3 mg/ml for 1–3 min, Fontana et al reported thin cystic blebs in 10 eyes (3%), of which five required surgical bleb revision, and one case (0.4%) of bleb-related endophthalmitis that occurred 2 years after limbus-based surgery.8 With the use of MMC 0.4 mg/ml for 3 min, Shigeeda et al found bleb leakage in nine eyes (7.3%), hypotonic maculopathy in one eye (0.8%), blebitis in five eyes (4.1%), endophthalmitis in one eye (0.8%) and worsening of the visual field with severe visual-acuity reduction (⩾3 lines) in nine eyes (7.3%).9
These data suggest a higher incidence of side-effects with the use of higher concentrations or longer exposures to MMC. Our results show that a low MMC dose and short exposure time do not increase the incidence of side-effects, compared with trabeculectomy without antiproliferative agents. Bleb leakage occurred in a few eyes (3%). Leakage can develop asymptomatically and regress spontaneously,12 24 and its incidence could have been underestimated. However, most of the patients were followed up at the same centre, with two or three visits a year, with standardised examination aiming to detect thin or leaking blebs. In such cases, ointment was prescribed. This could have led to a low incidence of infective complications. Postoperative therapy and management were the same, and no difference was found in the rate of postoperative procedures. Also, the two groups had about the same percentage of patients who were lost to follow-up. We found a high incidence of cataract progression, as expected in view of the age of patients (50–70 years at surgery) and the long-term follow-up. However, no grading system of lens opacity was used. No specific data on intraoperative complications (conjunctival buttonholes or tears, scleral tears or disinsertions, vitreous prolapse, bleeding) were collected. These complications can influence the outcome of trabeculectomy,25 but the incidence of most of them is reduced by a standardised and accurate surgery.
Risk-factor analysis failed to show any significant association with failure: only a few eyes had had ALT; the two groups had a similar incidence of failure after cataract surgery, but the long-term survival after cataract surgery needs to be further investigated. Other risk factors (older age, advanced perimetric damage, large IOP fluctuations) had a limited effect because of the inclusion criteria of the study. Diabetes is a significant risk factor for trabeculectomy failure,26 27 and patients with diabetes could have an increased risk of glaucoma.28 29 In this study, patients with diabetes were excluded, which could have improved the outcome of trabeculectomy in both groups.
In conclusion, trabeculectomy with low-dosage MMC and careful postoperative and long-term management improved the outcome of trabeculectomy with a low incidence of complications. As has been stated, “meticulous surgical technique, judicious use of these agents, close bleb surveillance, early intervention, and multimodal therapy with long-term plans for suppression of fibroblastic activity may augment bleb survival rates.”1 Information for the patient about the symptoms of late complications and long-term monitoring of the bleb to identify the conditions predisposing a case to complication are mandatory.30 The long-term incidence of more rare complications such as endophthalmitis needs to be investigated in larger studies.
REFERENCES
Footnotes
-
Competing interests: None.
-
Ethics approval: Ethics approval was provided by the Ethics Committee of the Azienda Policlinico “G. Rodolico,” Catania, Italy.
-
Patient consent: Obtained.
Linked Articles
- At a glance