Article Text

Abstract
Background/Aims To study the safety and effectiveness of 360° viscodilation and tensioning of Schlemm canal (canaloplasty) in black African patients with primary open-angle glaucoma (POAG).
Methods Sixty randomly selected eyes of 60 consecutive patients with POAG were included in this prospective study. Canaloplasty comprised 360° catheterisation of Schlemm's canal by means of a flexible microcatheter with distension of the canal by a tensioning 10-0 polypropylene suture.
Results The mean preoperative intraocular pressure pressure (IOP) was 45.0±12.1 mm Hg. The mean follow-up time was 30.6±8.4 months. The mean IOP at 12 months was 15.4±5.2 mm Hg (n=54), at 24 months 16.3±4.2 mm Hg (n=51) and at 36 months 13.3±1.7 mm Hg (n=49). For IOP ≤21 mm Hg, complete success rate was 77.5% and qualified success rate was 81.6% at 36 months. Cox regression analysis showed that preoperative IOP (HR=1.003, 95% CI=0.927 to 1.085; p=0.94), age (HR=1.000, CI=0.938 to 1.067; p=0.98) and sex (HR=3.005, CI=0.329 to 27.448; p=0.33) were all not significant predictors of IOP reduction to ≤21 mm Hg. Complication rate was low (Descemet's detachment n=2, elevated IOP n=1, false passage of the catheter n=2).
Conclusion Canaloplasty produced a sustained long-term reduction of IOP in black Africans with POAG independent of preoperative IOP. As a bleb-independent procedure, canaloplasty may be a true alternative to classic filtering surgery, in particular in patients with enhanced wound healing and scar formation.
- Canaloplasty
- collector channel
- microcatheter
- glaucoma surgery
- Schlemm canal
Statistics from Altmetric.com
Introduction
The best proven effective treatment for primary open-angle glaucoma (POAG) to date is the reduction of intraocular pressure (IOP) to a level that reduces the rate of progression. In developed countries, it is current practice to initiate treatment with either topical medication or laser trabeculoplasty. In African countries, there is a great barrier to successful medical management of glaucoma because of the relatively high cost of medications, and logistical and compliance problems. Most important, the reasons in favour of a surgical therapy are medical: the onset of glaucoma at a young age, the late presentation of a more advanced disease and the much higher IOP levels than seen in Caucasians.
Since its introduction by Cairns,1 trabeculectomy has been the most common approach to surgical reduction of IOP. However, the postoperative management is troublesome, and the success rate is less promising in patients from pigmented racial groups for known reasons related to enhanced wound healing and scar formation.2–5 From personal experience, we know that classic filtering surgery has very poor results in the African population, and it was abandoned at our institution many years ago. Alternative techniques such as trabeculotomy or trabeculoviscotomy6 were also not successful due to scar formation, but led to the idea of bleb-independent surgery. In 1995, the principles of viscocanalostomy7 were described by Stegmann, based on the rationale that the physiological outflow drainage system distal to the Schlemm's canal (SC) may not be altered in glaucoma.8–10 The mid-term results of viscocanalostomy of more than 200 eyes were promising.11 However, in following patients over many years, it became evident that most eyes with a failed viscocanalostomy had either a recollapsed SC or closed ostia of the collector channels as observed during revision of viscocanalostomy and determined by the reflux pattern of blood into SC on gonioscopy (personal experience). For these reasons, expansion of SC for a longer distance may increase the chance of keeping the canal patent and of giving aqueous access to collector channels remote from the exposed trabeculo-Descemet's membrane (TDM). This also makes sense for pathophysiological purposes, as the largest number of collector channels are located inferiorly and nasally.12–14 Creation of immediate access to these collector channels had been the aim for a long time, but circumferential dilatation of the canal was not possible due to technical considerations, until the recent development of a flexible microcatheter.15
Canaloplasty is a new bleb-independent (non-penetrating) glaucoma surgery that combines the principles of viscocanalostomy7 with a 360° circumferential distension of SC. A 1-year-long analysis of a multicentre study indicated that canaloplasty effectively reduces IOP in open-angle glaucoma with a low complication rate, whether or not it is combined with phacoemulsification.16 17 Any type of open-angle glaucoma was included in that study, and the great majority of patients were Caucasians (94%).
Here, we present the 3-year results of canaloplasty regarding efficacy and safety in black African patients with POAG, which may differ from glaucoma in Caucasians for the reasons mentioned earlier.
Material and methods
Setting
This prospective single centre study was performed at the Department of Ophthalmology, Medical University of Southern Africa (MEDUNSA), Pretoria, South Africa.
Study population
Sixty black African patients with advanced POAG were enrolled consecutively between July and December 2005. The great majority underwent primary surgical intervention (n=59). One eye was randomly selected in each patient for this study. All patients underwent diurnal curves the day before surgery that included IOP measurements at 08.00, 12.00, 16.00 and 20.00 hours. The mean IOP was used for statistical analysis.
Surgical technique
The procedure has been described in detail earlier.16 In brief, after limbal peritomy, haemostasis was obtained by compression with a sponge or by topical application of ornipressin (5 IU/ml, POR-8; Ferring Ltd, Pretoria, South Africa), if necessary. The superficial and deep scleral flap was dissected as described for viscocanalostomy.11 A temporal paracentesis was performed before SC was unroofed and TDM was exposed. After dilation of the ostia with a specific microcannula (Alcon-Grieshaber, Schaffhausen, Switzerland), a flexible microcatheter (iTrack-250A; iScience Interventional, Menlo Park, California, USA) was positioned in plane and in line to the SC and advanced 360°. The blinking light was observed through the sclera during the catheterisation of SC to identify the location of the distal tip of the catheter (figure 1A, B). During the catheterisation, 5 mg of sodium hyaluronidate (Healon GV, AMO, Abbott Park, IL, USA) was injected every two clock hours to dilate the SC stepwise (total about 30 mg). Following complete circumferential dilation of SC, a 10-0 polypropylene suture (Prolene, Ethicon Inc., Halfway House, South Africa) was tied to the distal tip of the microcatheter and looped through the SC (figure 2). The suture was tightened under tension on a soft eye in order to stretch the SC and trabecular meshwork circumferentially when IOP returned to normal (figure 3A, B). The deep scleral flap was excised and the superficial flap was closed watertight with five, or if necessary seven, interrupted 11-0 nylon sutures. Postoperative treatment was standardised and included three times a day antibiotic drops (ciprofloxacine/gentamicine) for 2 weeks, and steroid and non-steroid eye drops (dexamethasone/ketorolacum trometamolum) for 4 weeks.

The microcatheter has an optical fibre emitting laser light that allows transscleral visualisation of the catheter's tip as it traverses the canal (A). Gonioscopic view of the microcannula (B).

After completing the cannulation of the entire canal length with the microcatheter, and with the distal tip exposed at the surgical cut down, a 10-0 polypropylene suture is tied to the distal tip and looped through the canal.

Suture stenting of SC to maintain canal patency over 360° and to prevent collapse. (A) Schematic illustration shows the stretched inner wall of SC. (B) Slit-lamp gonioscopy after canaloplasty displays distension of inner wall (red arrow).
Statistical analysis
Descriptive statistics were used to determine continuous variables (demographic data and IOP). In accordance with other authors,18 complete success was defined as an IOP equal or lower than 21 mm Hg without medications, and qualified success with or without medications, respectively. A Kaplan–Meier survival model was used to determine the cumulative probability of an IOP of greater than 21, 18 and 16 mm Hg. Cox regression analysis was chosen to evaluate the factors potentially associated with the failure of IOP reduction, including preoperative IOP, age at surgery and sex. Corresponding HRs with 95% CI were estimated. HRs for continuous factors such as IOP and age were defined as the ratio of an increase in IOP of 1 mm Hg, and an increase in age of 10 years, respectively. Statistical analyses were performed using SPSS software version 13.0 (SPSS Inc, Chicago, IL, USA). A p value of less than 0.05 was considered statistically significant. Values are shown as mean±SD.
Results
The preoperative data are summarised in table 1. The mean preoperative IOP was 45.0±12.1 mm Hg. The mean follow-up time was 30.6±8.4 months. The mean IOP (without medications) at 6 months was 15.4±5.4 mm Hg (n=57), at 12 months 15.4±5.2 mm Hg (n=54), at 24 months 16.3±4.2 mm Hg (n=51), and at 36 months 13.3±1.7 mm Hg (n=49) (figure 4). For IOP ≤21 mm Hg, complete success rate (without medications) was 77.5% (38/49), and qualified success rate (with or without medications) was 81.6% (40/49) at 36 months. Eleven patients were lost to follow-up after 3 years. The complete success rate of an IOP of 21, 18 or 16 mm Hg or less after 36 months was 81%, 67.8% and 47.2%, respectively (figure 5). Cox regression analysis showed that preoperative IOP (HR=1.003, 95% CI=0.927 to 1.085; p=0.94), age (HR=1.000, CI=0.938 to 1.067; p=0.98) and sex (HR=3.005, CI=0.339 to 27.448; p=0.33) were all not significant predictors of IOP reduction below 21 mm Hg. In three eyes, IOP increased above 21 mm Hg within 6 months (early failure). There were no particular findings after surgery. The best corrected visual acuity (BCVA; Snellen's chart at 6 m distance) did not deteriorate in the majority of patients (57 eyes; 95%) during the 3-year study period (preoperative 0.61±0.42 vs postoperative 0.58 ±0.31; p=0.42). Initially, there was a temporary decline in BCVA in 34 eyes (56.6%) to 0.42±0.26, which returned to preoperative level by the first month in 16 eyes (26.6%) and by the second month in a further 18 eyes (30%). The difference in number of medications before and after surgery was two as the great majority of patients underwent primary canaloplasty (98%), and three patients were on betaxolol eye drops following surgery.
Preoperative data
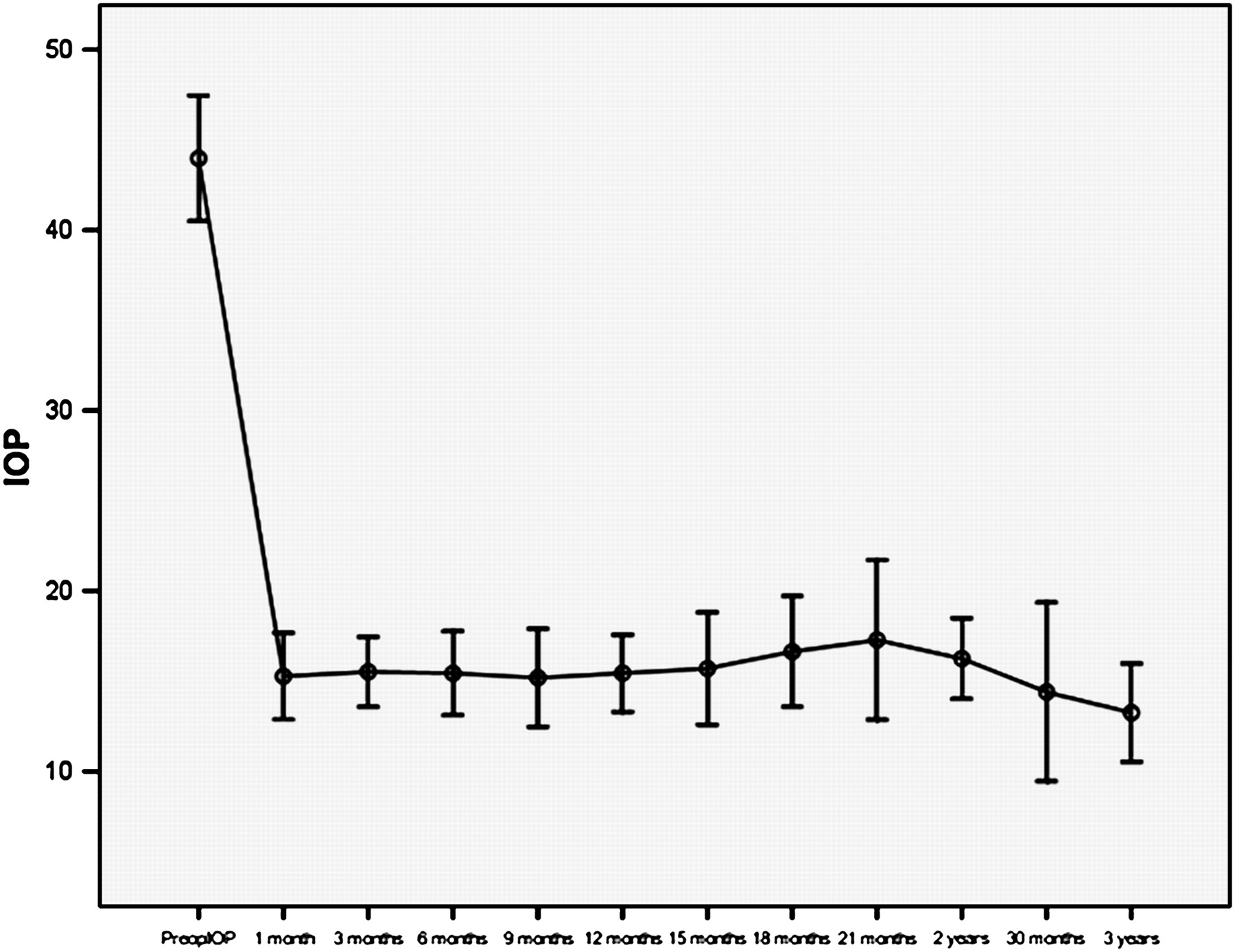
Mean postoperative pressure over 3 years (complete success).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis for IOP.
Intra- and postoperative complications are summarised in table 2. Detachment of the Descemet's membrane (two eyes) was reversible after 2 weeks. Passage of the microcatheter into the anterior chamber/suprachoroidal space happened each in one eye during the cannulation. In one eye with suprachoroidal passage, the IOP was low—between 10 and 12 mm Hg during the first week. The eye with trans-trabecular passage had an IOP spike at day 1 (32 mm Hg), possibly related to some viscoelastic material in the anterior chamber. The IOP was lowered with acetazolamide 250 mg twice a day for 2 days. At day 7, the IOP was 18 mm Hg without therapy. Both eyes had a comparable IOP to the mean of the uncomplicated cases during the observation time. Microhyphaema of less than 2 mm was very common but did not require additional therapy. After 3–7 days the blood was washed out from the anterior chamber. There were no severe complications in this series, namely, no hypotony-related flat anterior chamber, choroidal detachment or effusion syndrome, and no surgery-induced cataract. Further, no filtering bleb and associated problems were found.
Intra- and postoperative complications
Discussion
Canaloplasty produced a sustained long-term reduction of IOP in black Africans with POAG without significant complications. The principle IOP reduction with a mean drop of 28.9 mm Hg (65.8%) occurred early after surgery. One week after surgery, the mean IOP of all 60 eyes was 15.2 mm Hg, which remained stable during the 3-year study observation period. There was an additional late drop in mean IOP of 3 mm Hg of the 49 eyes followed over 3 years without any further intervention or medication, beginning 21 months after surgery. IOP before surgery, age and sex were not predictive for postoperative IOP below 21 mm Hg.
To date, there are two interim reports on the efficacy and safety of canaloplasty.16 17 In one study, canaloplasty was performed as a single procedure,16 and in the other one, in combination with phacoemulsification.17 In regard to mean IOP after surgery, the pressures in our study were comparable to the pressures in cases of canaloplasty alone at 6 months (15.4 vs 15.6 mm Hg) and at 12 months (15.4 vs 15.3 mm Hg),16 but the IOP reduction was much greater in the present study (28.5 vs 8.6 mm Hg). Although it is difficult to compare absolute IOP reduction in different studies that have different patient populations and surgeons, it is interesting that the level of the preoperative IOP (mean IOP 43.9 vs 24.7 mm Hg), also confirmed here by the Cox regression analysis, seems not to be predictive of the outcome in canaloplasty; rather, the postoperative IOP may be determined by the limitation of canaloplasty in its ability to lower IOP by the resistance of the distal outflow system and by the pressure of the episcleral vasculature. This may explain why IOP levels below 12 mm Hg are less likely to be achieved even after successful canaloplasty,16 17 in contrast to bleb-dependent glaucoma surgery with external filtration.
Further, we found a late drop in mean IOP of about 3 mm Hg without any additional intervention or medication at about 2 years after surgery. As this long-term report is the first of its kind and no cofactors were found, the reason for such late IOP reduction can only be speculated. A late restoration of some of the collector channels could be possible. Alternatively, persistent distension of the inner wall region may lead to tissue remodelling of the trabecular meshwork (TM) or even to atrophy of the TM. It has been recently been found that TM cells can sense mechanical stretching19 20 and respond by increasing matrix metalloproteinase (MMP) activities or levels (eg, MMP-2 and -14), while dramatically reducing levels of their primary inhibitor, tissue inhibitor of MMP (TIMP-2).19 21–23 Pathophysiologically, increased MMP activity in the TM with structural alterations of the juxtacanalicular region, the site of maximal resistance to aqueous outflow in POAG, results in reduced outflow resistance leading to IOP reduction.24 25
The present findings further show that preoperative IOP, age and sex did not have a significant impact on IOP reduction. At first, it might be astonishing that eyes with very high IOP levels did not have a poorer surgical outcome than eyes with a lower IOP before surgery, as one might assume that the higher the IOP, the greater the resistance to aqueous outflow and the more severely damaged the TM. However, as the TM and SC are viscodilated and inherent microdisruptions of the inner wall region occur, as demonstrated for viscocanalostomy,26–28 the pathological site of outflow resistance is directly targeted by canaloplasty. Furthermore, a canal which may be much narrowed in eyes with an increased IOP29 30 or even collapsed at an IOP above 40 mm Hg31 would be restored and kept open by the suture stent. In addition, postoperative IOP of about 15 mm Hg suggests patency of the distal outflow system in the patients studied. This is in line with common thoughts that the collector channel–aqueous vein system may not be altered in POAG.8 9 Further, we found that patient's age at surgery was not predictive for IOP reduction. This may hold true for the patients studied who did not have medical treatment over years; however, this needs to be confirmed in eyes with long-term drug applications, as drug-induced changes to the conjunctiva and the episcleral outflow system found in glaucoma patients32–35 may hamper physiological outflow of aqueous after canaloplasty.
One of the major advantages that canaloplasty offers over trabeculectomy is the potential for a low complication rate. There is no direct fistula through the sclera, and hypotony with flat anterior chamber and choroidal detachments are avoided. Further, none of the patients developed significant visual loss or cataract during this study, two known cumbersome complications after filtering surgery, especially in the young patient.
Other intra- and postoperative complications were rare. During surgery, there were eight cases where the microcatheter could not pass at first try. In three of them, a slight counter-pressure over the distal tip of the catheter on the limbus was helpful. In five eyes, passage from the other side was necessary for complete 360° cannulation. Passage of the catheter into the suprachoroidal space and into the anterior chamber occurred in each one eye. Both events can surgically be regarded as adverse as the wall of SC is perforated, but functionally as beneficial in regard to IOP, in case the created passage did not heal up. The first event may act as a microcyclodialysis and the second as a localised trabeculotomy. In the present study, both eyes with such events had an IOP comparable with the mean of the uncomplicated cases after 1 week, suggesting that the passage may have closed off early after surgery. Suture ‘cheese-wiring’ into the anterior chamber during and after surgery was, contrary to our expectations, not encountered even in the first cases in this series. This could be due to underestimating the resistance of the inner wall of the SC to tension, or alternatively, to the relative elasticity of the polypropylene suture,36 or to possible relaxation of the suture knot. Early postoperative complications were mainly related to transient hyphaema, which represents refluxed blood from the venous system through the widely open canal and highly permeable TM. Regurgitation of blood also indicates that the distal outflow system was patent or became re-established by canaloplasty. In agreement with other authors,16 we find that microhyphaema in the early days after canaloplasty may even be a good sign of adequate tension on the TM. Whether it is also prognostic for the surgical outcome remains to be investigated.
In conclusion, canaloplasty may provide sustained IOP reduction in POAG with a low rate of complications. As a bleb-independent procedure, canaloplasty may play an increasing role in the surgical management of glaucoma, as it is the most physiological approach to treatment, in particular in a population of which the eyes are known to be very responsive to surgical interventions.
References
Footnotes
Funding None.
Competing interests RS has received an unrestricted grant from iScience Interventional. None of the other authors have received public or private financial support, nor do any have a proprietary or financial interest in any material or method mentioned.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of institutional ethics committees. The research followed the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance