Article Text

Abstract
Purpose To propose a novel classification system for polypoidal choroidal vasculopathy (PCV), and compare the clinical outcomes among PCV subtypes.
Methods Consecutive treatment-naive patients with symptomatic PCV were managed over 5 years. PCV subtypes were classified based on indocyanine green angiography (ICGA) and fluorescein angiography (FA) characteristics.
Results Among 107 patients, 3 PCV subtypes were seen: Type A (interconnecting channels on ICGA) –22.4%; Type B (branching vascular network with no leakage) –24.3%; Type C (branching vascular network with late leakage on FA) –53.3%. The proportion of patients with best-corrected visual acuity (BCVA) ≥20/40 was highest in Type A, intermediate in Type B and lowest in Type C at all time points (80% vs 66.7% vs 7.7% at 5 years, p<0.001). The highest rate of moderate visual loss (loss of ≥3 lines) occurred in Type C PCV (57.7% vs 0% for Types B and A at 5 years, p<0.001). Risk factors for poor visual outcomes were PCV subtype (OR 53.7, p<0.001 for Type C and OR 13.7, p=0.023 for Type B compared to Type A) and age (OR 1.06, 95% CI 1.002 to 1.125, p=0.044).
Conclusions The PCV subtype seen on initial presentation affects the long-term visual outcomes over a 5-year period.
- Retina
- Macula
- Imaging
Statistics from Altmetric.com
Introduction
Polypoidal choroidal vasculopathy (PCV) is characterised by abnormal vascular networks with terminal dilatations, which form polyps.1 ,2 PCV occurs more commonly in Asian populations, where it comprises between 23% and 55% of patients presenting with neovascular age-related macular degeneration (AMD).3–5
The visual outcomes of PCV is generally better compared to choroidal neovascularisation (CNV) from AMD.4 ,6 In addition, PCV responds less favourably to antivascular endothelial growth factor (anti-VEGF) monotherapy compared to typical AMD, with incomplete polyp closure in a majority of cases.7–10
PCV lesions are not consistently visualised on fluorescein angiography (FA) due to early leakage of fluorescein from the polyps and vascular network. Using indocyanine green angiography (ICGA), the dye remains largely intraluminal, thereby allowing better visualisation of the polyps and abnormal vasculature, especially in the early phase.11 Confocal scanning laser ophthalmoscopy (CSLO) provides more detailed visualisation of the subretinal pigment epithelium (RPE) vasculature compared to conventional angiograms.12 ,13 The confocal aperture allows light from a specific plane to pass through, thus preventing overlapping images from different layers.
Currently, there is no uniform classification system for PCV based on its angiographic characteristics. While some authors have described classifications based on clinical features,14 the configuration,15–17 location17 or size16 of the polyps, or the associated vascular network,18 there is limited data on the relationship between these groups and clinical outcome.16–18 Classification systems for diseases should show differences in presentation, natural history or clinical outcomes.
In our clinical practice, we identified different characteristics of the branching vascular networks of PCV on ICGA (figure 1), and observed that some patients with symptomatic PCV do not have severe leakage on FA on presentation. These features appeared to influence long-term visual outcome, with significant leakage on FA resulting in worse prognosis. In this exploratory study, we postulate that the vascular subtypes of PCV which are seen on initial clinical presentation are independently associated with the long-term clinical outcome. We aimed to describe a novel classification system for PCV using ICGA and FA characteristics, and to compare the clinical outcomes among the PCV subtypes.

Indocyanine green angiography of interconnecting channels and branching vascular networks (BVN). 1A. Early choroidal phase at 16.2 s, showing early filling of a network of criss-crossing choroidal vessels (outlined). No feeder vessel or specific point of origin is seen for these vessels. 1B. Angiogram at 19.7 s, showing early filling of the polyps and the criss-crossing interconnecting channels adjacent to them. 1C. ICGA at 25.5 s, illustrating complete filling of the polyps and the interconnecting channels, which appear brighter than the background choroidal vessels. 1D. Early choroidal phase (15.4 s) showing dye originating from a feeder vessel (arrow) at the centre of the BVN and starting to radiate outward. 1E. ICGA at 18.6 s, showing more prominent filling of the BVN, with early filling of some polyps. 1F. The BVN and polyps are completely filled at 3 min 13 s.
Methods
We performed a retrospective institution-based cohort study of 107 consecutive treatment-naive patients who presented with symptomatic PCV between July 2003 and June 2005 at the National Healthcare Group Eye Institute, Tan Tock Seng Hospital, Singapore. The patients were managed by fellowship-trained retinal specialists over the subsequent 5 years, with assessment of clinical features on dilated slitlamp biomicroscopy and LogMAR visual acuity (VA) at each visit. This study was approved by the Institutional Review Board of the National Healthcare Group, and conformed to the tenets of the Declaration of Helsinki. Written, informed consent was obtained from patients prior to treatment.
Baseline investigations included CSLO FA and ICGA using the Heidelberg Retinal Angiograph (HRA) II (Heidelberg Engineering, Heidelberg, Germany). The angiograms were graded independently by two Reading Center-certified retinal specialists (THL & CST) for the diagnosis of PCV and, subsequently during the chart review, the classification of the lesions. In cases of disagreement, the two graders met in open adjudication to review the cases.
Angiograms were obtained using a standardised imaging protocol. The early phases (up to 45 s) were imaged using dynamic ICGA and FA. Stereoscopic 30-degree still angiographic images (ICGA and FA) were obtained at 1, 3, 5, 10 and 20 min and reviewed using the Heidelberg Eye Explorer software (V.1.7.0.0) on a wide-screen monitor using a stereo viewer (Screen-Vu Stereoscope; PS Manufacturing, Portland, OR).
PCV was diagnosed using standardised diagnostic criteria, which has previously been described.3 ,7 This consisted of early, focal subretinal hyperfluorescence on ICGA, together with at least one of the following criteria:
-
nodular appearance of the polyp(s) on stereoscopic examination;
-
hypofluorescent halo around the nodule(s);
-
presence of a branching vascular network;
-
pulsation of the polyp(s) on dynamic ICGA;
-
orange, subretinal nodules on colour fundus photography;
-
massive submacular haemorrhage (defined as submacular haemorrhage ≥4 disc areas in size).
Patients who were lost to follow-up before 1 year, or where the diagnosis of PCV was unclear, were excluded from this study.
Macular PCV lesions were treated using photodynamic therapy (PDT) with verteporfin (Visudyne, Novartis International AG, Basel, Switzerland) by the attending retinal specialists (THL and CST) using a standardised treatment protocol, guided by ICGA. Anti-VEGF agents were not commonly used in our institution during the initial 4 years of the study, and PDT was the main treatment option. All patients presented with symptomatic PCV (decrease in VA, metamorphopsia, or other visual symptoms) and either subretinal fluid or retinal thickening on optical coherence tomography (OCT). Treatment was initiated or repeated when there were clinical signs of disease activity, such as a drop in best-corrected VA of ≥5 letters, subretinal haemorrhage or macular oedema, or evidence of PCV activity on ICGA and FA. Full-duration PDT was performed on all patients and the treatment zone included all visible polyps and the associated branching vascular network.
Review of PCV classification and clinical outcomes
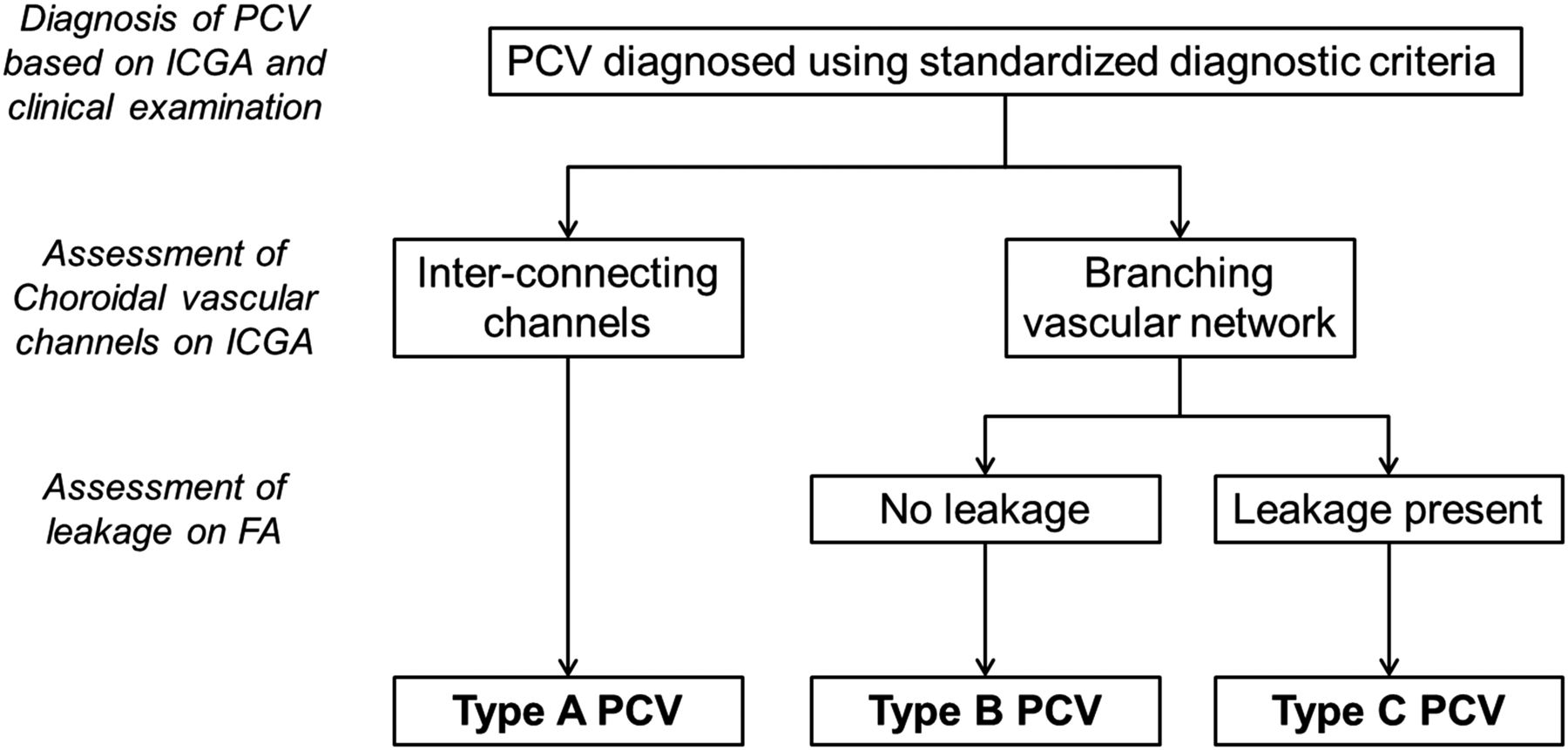
We devised a classification system (figures 2 and 3) based on an a priori inspection of PCV patients from our institution. The classification was applied at the time of the review of the clinical data (after the patients had already been treated) and, therefore, did not influence the judgment of the attending ophthalmologists or their treatment decisions.
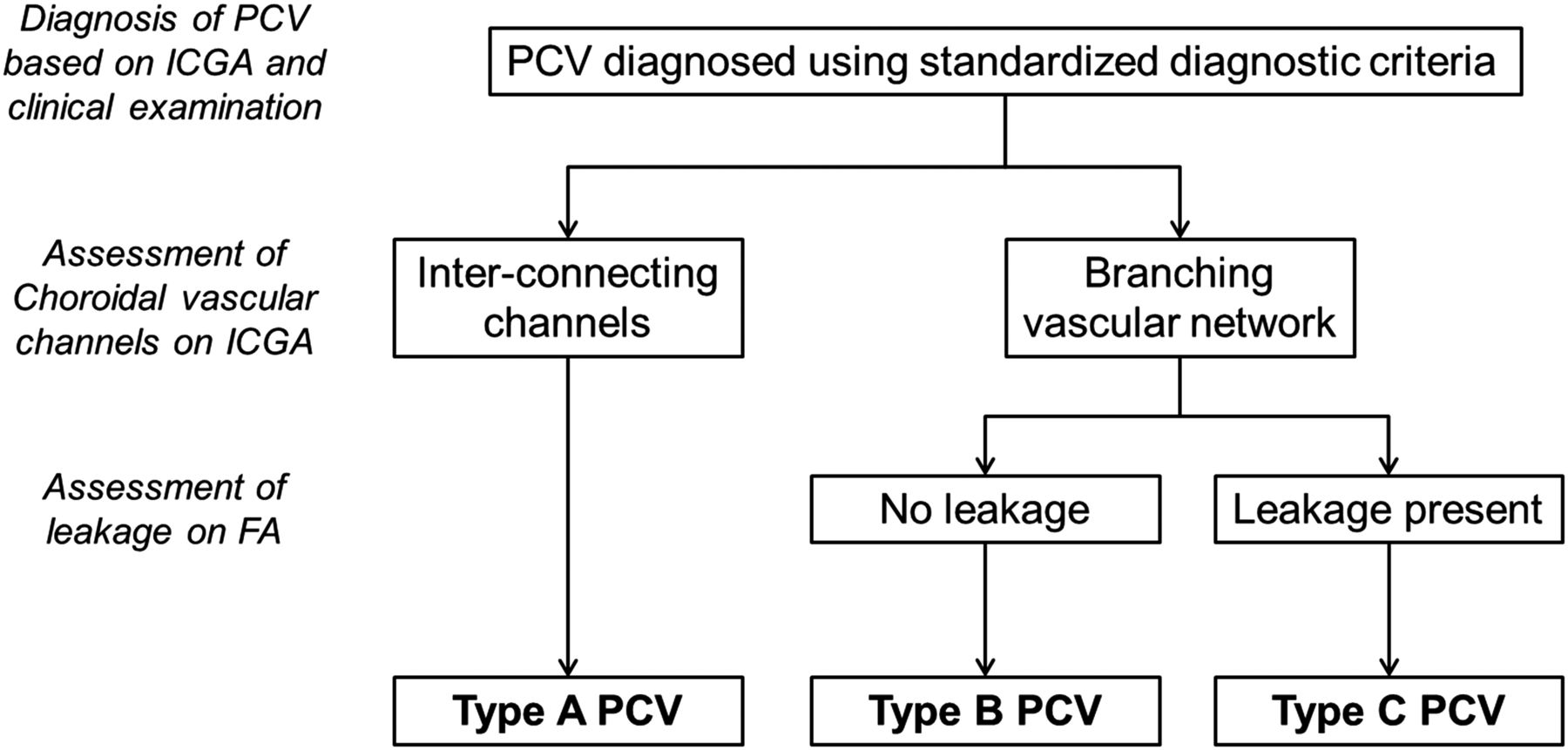
Classification system for polypoidal choroidal vasculopathy (PCV). ICGA—indocyanine green angiography. FA—fluorescein angiography.

{kind=link}
{kind=link}
{kind=link}
Vascular subtypes of polypoidal choroidal vasculopathy (PCV), illustrating indocyanine green angiography (ICGA) and fluorescein angiography (FA) features. (A) Type A PCV—ICGA reveals polyps and interconnecting channels nasal to the fovea. (B) Type A PCV—Early FA showing pooling and retinal pigment epithelium (RPE) window defects. (C) Type A PCV—Late FA showing pooling and RPE window defects, but no leakage. (D) Type B PCV—ICGA demonstrating polyps at the periphery of a large branching vascular network. (E) Type B PCV—Early FA showing RPE window defects. (F) Type B PCV—Late FA showing pooling in a pigment epithelium detachment and RPE window defects, but no leakage. (G) Type C PCV—ICGA showing polyps and a branching vascular network. (H) Type C PCV—Early FA showing pooling. 2I. Type C PCV—Late FA showing leakage at the macula and temporally.
The angiogram images were assessed for the presence of a branching vascular network on ICGA and presence of late leakage from the PCV lesion on FA. For Type A PCV, polyps were supplied by interconnecting channels (figure 1A–C). These consisted of a network of criss-crossing vessels which had no specific point of origin or direction of flow, but filled simultaneously during the choroidal filling phase. For Types B and C, a distinct branching vascular network was observed (figure 1D–F). The dye originated from a specific point (commonly a feeder vessel) and exhibited a distinct direction of flow, usually radiating toward the periphery to supply the polyps. In Type B, no leakage was observed on FA, whereas in Type C, significant late leakage was seen (figure 3). The location of the PCV lesions were defined as previously described.3 In brief, macular lesions occurred predominantly within a circle of 3 mm radius (two disc diameters) centred on the fovea. Peripapillary lesions occurred predominantly within one disc diameter of the optic disc margin, and lesions located elsewhere were extramacular.
Good visual outcome was defined as VA ≥20/40, while moderate visual loss (MVL) was defined as a loss of ≥3 lines from the initial presenting VA.
Statistical analysis was performed using SPSS V.16 (SPSS, Chicago, Illinois, USA). χ2 Tests were used to compare the proportions of various groups, and unpaired t tests used to compare means, with p<0.05 considered statistically significant.
Results
The mean age of the 107 patients was 66.6 years (range, 31–91, SD±10.3), and 62.6% were males (table 1). Overall, 5 patients were excluded from this study due to inability to confirm the diagnosis of PCV using the above criteria. The most common diagnostic features of PCV were nodular hyperfluorescence (95.3%), hypofluorescent halos around the nodule (81.3%) and branching vascular networks (77.6%). Pulsation of the polyps occurred in 25.2%, the frequency of orange subretinal nodules was 37.4% and massive submacular hemorrhage occurred in 7.5% of patients. Most PCV lesions were located at the macular region (94 eyes, 87.9%), while seven were peripapillary (6.5%), and six were extramacular (5.6%). The mean lesion area on ICG was 6.9 mm2 (range, 0.07–40.0, SD±8.2 mm2).
Comparison of characteristic among the 3 PCV subgroups
PCV vascular subtypes
Using our classification system, 24 patients (22.4%) were Type A, 26 (24.3%) were Type B, and 57 (53.3%) were Type C. There were no significant differences among the three PCV subtypes in terms of gender or laterality (table 1).
Evaluation of clinical outcomes
To avoid confounding due to PCV location, the visual outcomes of lesions located at the macula (94 patients) are presented below. There was no significant difference between the three PCV subtypes in terms of the total number of PDT treatments received.
Overall, 37.5% of all patients achieved good VA (≥20/40) at 5 years (table 2). There were statistically significant differences in the visual outcomes among the three PCV subtypes at all time points. Type A had the best visual outcomes, with 80–100% of patients achieving good VA over the 5-year period. By contrast, between 56.2% and 75% of patients with Type B maintained good VA, and the percentage of patients with Type C PCV who achieved this was much lower, ranging from 7.7% to 22.2%.
Visual outcomes of the PCV subtypes over 5 years (macular location only)
Analysing the proportion of patients who lost ≥3 lines from baseline, patients with Type A PCV had the best outcomes (table 2), with none experiencing MVL except at 24 months. MVL among Type B PCV ranged from 8.7% to 23.5% during the first 3 years, but decreased to 0% in the fourth and fifth years. By contrast, MVL for Type C PCV was considerably greater, ranging from about 40% to 50% in years 1–3, and increased to 57.7% by 5 years.
Over 5 years, recurrences occurred in 35.1% of patients, with the recurrence rates varying according to subtype (Type A: 15.8%, Type B: 21.7%, Type C: 48.1%, p=0.078). The lesion size varied significantly among PCV subtypes, and was smallest for Type A, and largest for Type C (table 1). Overall, the mean PCV lesion area increased from baseline to the final visit (6.7 mm2 vs 10.7 mm2, p=0.001). Analysing by subtype, there was no significant change in lesion area for Type A (1.8 mm2 vs 1.8 mm2, p=0.875), while the area increased from 5.4 mm2 to 10.1 mm2 for Type B (p=0.079), and from 9.1 mm2 to 13.8 mm2 for Type C (p=0.006). The PCV subtype at the end of the study remained the same in 77 of 94 patients (81.9%). Among Type A, 73.7% of patients remained the same, and 26.3% became Type C by 5 years. For patients classified as Type B at the start, 60.9% remained Type B, whereas the remaining 39.1% developed leakage and were reclassified as Type C. Of patients initially diagnosed as Type C, 94.2% remained Type C, and only 5.8% were reclassified as Type B. There were no cases of either Type B or C converting to Type A.
Performing multivariate analysis with PCV subtype, lesion size on ICGA and age as variables, PCV subtype and age were significant factors for visual outcomes. Patients with Type C and Type B PCV had higher rates of VA <20/40, with OR of 53.7 (95% CI 5.8 to 496.5, p<0.001) for Type C, and OR 13.7 (95% CI 1.4 to 46.4, p=0.023) for Type B. For every year of increase in age, the risk for poor visual outcome increased by a factor of 1.06 (95% CI 1.002 to 1.125, p=0.044).
Discussion
In this study, we have described a novel classification system for PCV, and demonstrated in a consecutive cohort of symptomatic, treatment-naive patients, that the PCV subtype seen at the time of initial clinical presentation influences the 5-year visual outcome. Type A had the best visual outcomes, in terms of achieving good visual acuity (≥20/40) or avoidance of MVL (≥3 lines of VA), whereas the visual outcomes were intermediate in Type B, and worst for Type C.
There remains controversy whether PCV is a subset of AMD, or an independent clinical entity,14 ,19–21 and it is not the purpose of this study to address that question. Regardless of its nature, PCV has certain distinctive features which are readily identifiable on ICGA, and which are not seen in patients with typical AMD. Additionally, their clinical outcomes differ from typical AMD patients.19 ,20 Therefore, it is relevant to consider adopting standardised diagnostic and classification criteria for PCV in order to allow comparison of clinical outcomes among different studies.
The clinical outcomes of PCV reported in the literature vary considerably, with rates of poor visual outcome ranging from 35% to 68.2%.4 ,15 ,22 While generally believed to have better visual prognosis than AMD, some of patients with PCV do suffer severe visual loss.22–24 At 5 years, 31.2% of our patients experienced moderate visual loss, which is consistent with previous reports. However, the three subgroups of PCV demonstrated significant differences in their long-term visual outcomes, which illustrates the usefulness of the classification system. The variability in the visual outcomes and clinical course of PCV in various studies may be related to variation in PCV diagnostic criteria and, possibly, the existence of clinical subtypes of PCV with different clinical patterns and prognosis.
To our knowledge, only a few authors have attempted to classify the PCV lesions, but many did not compare long-term clinical outcomes of the different groups. Various studies have classified the polypoidal lesions based on clinical features,14 polyp configuration,15–17 location17 or size,16 or the appearance of the vascular patterns,18 ,25 with two authors correlating the polyp configuration with clinical outcomes.15 ,16
Some papers have focused on the branching vascular network associated with the polyps. In particular, Yuzawa et al18 described two subtypes of PCV: ‘typical PCV’, where neither feeder nor draining vessels were detectable, and ‘polypoidal CNV’, where feeder and draining vessels are visible on ICGA, and network vessels are numerous. Tanaka et al25 reported that the rs800292 variant of the complement factor H gene and the rs10490924 variant of the age-related maculopathy susceptibility 2 (ARMS2) gene were associated with polypoidal CNV, but not with typical PCV. However, that paper did not report the visual outcomes associated with the 2 subtypes. While there are similarities in the descriptions (Type A in our series may correspond to ‘typical PCV’, and Types B and C may correspond to ‘polypoidal CNV’), our study has further subdivided the patients based on FA leakage, and demonstrated significant differences in visual outcomes between these subtypes over a 5-year period.
A standardised classification system for PCV can be applied to future clinical studies, especially randomised clinical trials. Since our results show that different subtypes have different clinical outcomes over 5 years, it may be important to assess the subtype of PCV, and allocate them equally across different treatment arms. For the individual patient, this classification system allows prognostication of this disease. In this series, 80% to 100% of Type A PCV had good visual outcomes, whereas only 7.7% to 22.2% of Type C achieved the same outcomes. By classifying PCV, the patient can be counselled more accurately on his visual prognosis, and the presence of a more severe subtype of PCV would alert the clinician to the need for more stringent and closer follow-up.
It is interesting that lesion size was not a significant factor on multivariate analysis. A possible explanation is the collinearity of the PCV subtype and lesion size. The size of the PCV lesion is significantly correlated with lesion type (table 1), and hence the effect of lesion size would have been accounted for by classifying PCV into subtypes.
The strengths of this study include a large series of consecutive patients who were followed-up over a long duration, the diagnosis of PCV using stringent and standardised diagnostic criteria based on CSLO ICGA and clinical examination, and consistent assessment and management by the same retinal specialists.
Limitations include the retrospective nature of this study. However, the main objective of this study is to describe a classification system for PCV, and to demonstrate that the PCV subtype at presentation is associated with the eventual clinical outcome. It would be useful in future to see if the same outcomes occur in a prospective study.
In summary, we have proposed a novel classification system for PCV using CSLO angiographic features. The PCV subtype on presentation affects the long-term clinical outcomes over 5 years. This classification system may have important applications to future clinical studies, as well as in the management of the individual patient.
Acknowledgments
This study was supported by the National University of Singapore-National Healthcare Group Clinician Leadership in Research Grant CLR-09006 (Dr Tan). Dr Tan also receives research funding from the National Healthcare Group Clinician Scientist Career Scheme Grant (CSCS/12005) and travel support from Bayer (South East Asia) Pte Ltd, Heidelberg Engineering and Novartis. Dr Tock Han Lim receives travel support from Novartis, Bayer and Heidelberg Engineering.
References
Footnotes
This study was presented at the American Academy of Ophthalmology Annual Meeting 2012 (November 2012, Chicago, USA).
-
Contributors All authors fulfil the requirements for authorship, and all contributors have been appropriately acknowledged.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Institutional Review Board of the National Healthcare Group.
-
Provenance and peer review Not commissioned; externally peer reviewed.