Article Text

Abstract
OBJECTIVE This study was designed to establish whether a ratio of three units of Dysport® is equivalent to one unit of Botox® for the treatment of cervical dystonia.
METHODS Patients with predominantly rotational cervical dystonia, and a minimum of four previous Botox treatments, were randomised to receive either the clinically indicated dose of Botox or three times that dose in Dysport units. Study botulinum toxin was administered in a double blind fashion, to one or more clinically indicated muscles, at one or more sites per muscle. Patients returned for assessment two, four, eight, and 12 weeks after treatment.
RESULTS A total of 73 patients (Dysport, 38; Botox, 35) were entered. The Dysport group received a mean (SD) dose of 477 (131) (range 240–720) Dysport units, and the Botox group received a mean (SD) dose of 152 (45) (range 70–240) Botox units. The mean (SEM) post-treatment Tsui scores for the Dysport group (4.8 (0.3)) and the Botox group (5.0 (0.3)) were not statistically different (p=0.66). The study had 91% power to detect a clinically significant difference of two points. Both groups showed substantial improvement in Tsui score by week 2 (mean (SD); Dysport, 46 (28)%; Botox, 37 (28)%), with a peak effect at week 4 (mean (SD); Dysport, 49 (29)%; Botox, 44 (28)%). A similar response profile was seen for other assessments of efficacy. The duration of effect, assessed by time to retreatment, was also similar (mean (SD); Dysport, 83.9 (13.6) days; Botox, 80.7 (14.4) days; p=0.85). During the study 22 of 38 (58%) Dysport patients reported 39 adverse events, and 24 of 35 (69%) Botox patients reported 56 adverse events (p=0.35). A global assessment of efficacy and safety considered that 29 of 38 (76%) Dysport patients and 23 of 35 (66%) Botox patients were treatment successes (p=0.32).
CONCLUSION Patients with predominantly rotational cervical dystonia treated with the clinically indicated dose of Botox or three times that dose in Dysport units show similar improvements and do not have significantly different safety profiles.
- botulinum toxin
- cervical dystonia
- bioequivalence
Statistics from Altmetric.com
Botulinum toxin type A is a potent neurotoxin isolated fromClostridium botulinum. Despite its highly toxic nature, botulinum toxin has therapeutic applications, and it has become the treatment of choice for many dystonic conditions, including cervical dystonia.1
Cervical dystonia is characterised by sustained involuntary contractions of the cervical muscles leading to painful and disabling postures. Rotation of the chin and tilt, flexion, or extension of the head are thus present either in isolation or in various combinations. A prevalence of 89/million population has been reported.2
Botulinum toxin therapy induces a temporary, partial chemodenervation of the injected muscles.3 Injection into cervical muscles causes relaxation in muscle tone and fibre atrophy and reduces motor unit potential size,4 thereby decreasing the force of muscle contraction. This produces relief from pain, increased range of free movement, improved resting posture, and less overall disfigurement, leading to improved quality of life for most patients.
Dysport® and Botox® are the two preparations of botulinum type A toxin commercially available at present. It is clear from the literature and from clinical experience that the units used to quantify the toxin activity of the two products are not equivalent. This apparent difference in the potency of the two products causes difficulties when comparing the results of studies using the different preparations, and when changing from one preparation to the other. It is likely that any difference between the two products is the result of the different assay methods used to quantify the activity of the products,5 and a bioequivalent ratio of one Botox unit to three Dysport units has been suggested.6 7
This study was designed to compare a clinically established dose of Botox with three times that dose in Dysport units in the treatment of patients with predominantly rotational cervical dystonia.
Methods
ETHICAL CONSIDERATIONS
This study was conducted in accordance with the Declaration of Helsinki and its amendments, as well as the guidelines for good clinical practice. It was approved by the appropriate national regulatory organisations and local research ethics committees. The study was explained fully to eligible patients, and written informed consent was obtained before any study specific assessments were performed.
STUDY POPULATION
Patients were required to have predominantly rotational cervical dystonia, with involuntary contractions of a constant duration, as defined by Tsui et al.8 In addition, a minimum of four previous Botox treatments were required, with the latest being within 10–16 weeks of study treatment.
Patients with other forms of cervical dystonia were thus excluded, as were patients who required more than 250 units of Botox, or a dose of Botox 100 units more than a previous dose shown to be effective. Other exclusion criteria were hypersensitivity to botulinum toxin, swallowing abnormalities (moderate difficulty in swallowing liquids or solids), pregnancy or breastfeeding, myasthenia gravis or other disease of the neuromuscular junction, and unwillingness or inability to comply with the protocol. Any patient who had taken an investigational new drug (a new chemical entity not registered for use) in the preceding three months, or was due to receive such a drug during the study period, was also excluded.
TSUI SCORE
The total Tsui score8 (0–25) was calculated using the equation (A × B) + C + D, where each component of the equation was made up as follows:
A=Amplitude of sustained movements: a combined score made up from assessment of the amplitude of rotation, laterocollis, anterocollis, and retrocollis, which were scored from 0–3 (0=absent, 1<15°, 2=15–30°, 3>30°).
B=Duration of sustained movements, where 0=none, 1=intermittent, and 2=constant.
C=Shoulder elevation, where 0=absent, 1=mild and intermittent, 2=mild and constant, or severe and intermittent, and 3=severe and constant.
D=Tremor, which was calculated by multiplying the severity of tremor (0=none, 1=mild, 2=severe) by the duration (0=none, 1=occasional, 2=continuous).
The inclusion criteria required patients to have a predominantly rotational form of cervical dystonia, as defined by a rotation score of at least 1, a laterocollis score no greater than the rotation score, a retrocollis score of no more than 1, and an anterocollis score of 0.
ASSESSMENTS AT ENTRY (WEEK 0)
Demographic data (sex, date of birth, weight, height, race) and vital signs (heart rate, systolic/diastolic blood pressure, temperature) were assessed and recorded. Other data collected included the date that cervical dystonia was first diagnosed, whether the patient had any other type of dystonia, or if any relative also had cervical dystonia. Also recorded were the date of the patient’s first Botox treatment, their total number of treatments, the cumulative dose of Botox injected, the maximum single dose injected, and the date, dose, and injection sites of the most recent Botox injection.
The signs and symptoms of cervical dystonia were assessed, and the total Tsui score was calculated. Pain associated with cervical dystonia was assessed by the patient as none, mild, moderate, or severe.
Details of all medical events experienced by the patient, and all concomitant medication received by the patient during the seven days prior to entry were recorded.
ASSESSMENTS AT WEEKS 2, 4, 8, AND 12
Tsui score and pain associated with cervical dystonia were assessed and recorded as described previously. In addition, both the patient and the investigator assessed cervical dystonia symptoms in relation to the symptoms at entry before receiving study toxin (symptom free, improvement >50%, improvement <50%, no improvement, or worse).
Adverse events either seen by the investigator or reported by the patient were assessed and recorded. As well as the diagnosis, each adverse event was assessed for intensity (mild, moderate, severe), seriousness (not serious, serious), action taken (none, treatment, other), duration, and relation to the study drug (probable, possible, unlikely, unrelated). Vital signs and changes in concomitant medication were also assessed and recorded.
ASSESSMENTS ON COMPLETION OF THE STUDY
Study completion occurred at the week 12 assessment, or earlier if patients required retreatment. The need for retreatment was based on a global clinical evaluation of each patient, and the protocol allowed patients to be re-treated as early as week 8. Patients who were not re-treated at week 12 were followed up until week 16 to collect retreatment details. The date of re-treatment, or the reason for not re-treating, was recorded for each patient.
On completion of the study the investigator made a global assessment of the efficacy and safety of the study toxin. Efficacy was assessed on a six point scale (excellent, good, moderate, slight improvement, no change, or worse). Safety was assessed in terms of adverse events on a five point scale (none, mild, moderate, severe, or extreme). Patients were considered a treatment success if the efficacy assessment was excellent, good, or moderate, and the safety assessment was none, mild, or moderate.
STUDY TOXINS
Dysport (Speywood Pharmaceuticals Ltd, Maidenhead, UK) was supplied in clear glass vials as a freeze dried white pellet containingClostridium botulinum type A toxin haemagglutinin complex together with 125 μg human albumin and 2.5 mg lactose. Each vial contained 500 Dysport units. It was recommended that vial contents should be reconstituted in sodium chloride injection BP (0.9%), and used within one hour.
Botox (Allergan Inc, Irvine, California, USA) was supplied from commercial stock as a crystalline complex containing Clostridium botulinum type A toxin with an associated haemagglutinin protein, 500 μg human albumin, and 0.9 mg sodium chloride. Each glass vial contained 100 Botox units. It was recommended that the vial contents should be reconstituted according to the manufacturer’s instructions.
RANDOMISATION, BLINDING, AND ADMINISTRATION OF STUDY TOXIN
The doses used in this study were not fixed, but based on the clinical need of each patient. At entry, the investigator assessed the clinical symptoms of the patient and reviewed previous responses to treatment, to determine the next clinically indicated dose and the most appropriate injection sites. Eligible patients were randomised to receive either the clinically indicated Botox dose or three times that dose in Dysport units. Before the start of the study a randomisation list was generated in blocks of four patients and each centre was allocated sufficient patient numbers, with individual patient randomisation envelopes.
Blinding of the study medication was the responsibility of the study pharmacist. This role was performed by the hospital pharmacy at the five Swedish centres, and by a designated study nurse at the two Finnish centres. The study pharmacist was not involved with patient management or assessment. Once the investigator informed the study pharmacist of the proposed dose for the patient, the study pharmacist opened the next randomisation envelope, which allocated either Dysport or Botox treatment, and prepared a syringe with the appropriate dose of study toxin. Injection volume was determined by the proposed Botox dose (1ml/100 units), regardless of actual study toxin, thereby maintaining the study blind.
Treatment was administered by intramuscular injection to one or more muscles as clinically indicated, and each muscle could be injected at more than one site. No further botulinum toxin treatment was given until the end of the study. Only the clinically indicated Botox dose and the muscles injected were recorded. The investigator remained blinded throughout the study, and was only made aware of treatment allocation at the end of the study when all data were ready for analysis.
STATISTICAL ANALYSIS
Two primary efficacy variables were identified by the protocol: the mean post-treatment Tsui score up to week 12 or until retreatment if this was before week 12, and the time between administration of study toxin and re-treatment.
The sample size calculation was based on the mean post-treatment Tsui scores. It was planned to recruit 90 patients (45 patients/group) to ensure that the study would have 90% power to detect a clinically significant between group difference (α=0.05, two tailed test) in the mean post-treatment Tsui score of two or more points, assuming an SD of three points. The study was brought to a close once all available eligible patients had been recruited from the participating centres. Despite not recruiting 90 patients, the primary efficacy index was less variable than predicted, such that with 73 patients the study had 91% power.
Plans for the statistical analysis of the study were summarised in the protocol and presented in detail in a prospective analysis plan. No changes were made to this plan after the unblinding of the study.
All randomised patients also received study medication, and completed the study. All patients, therefore, were included in the efficacy and safety analyses. Due to a between group difference in Tsui score at entry, and between group differences in the mean post-treatment Tsui score at some centres, the overall analysis of the mean post-treatment Tsui score was performed using analysis of covariance (ANCOVA). The time to re-treatment was compared between groups using a Cox proportional hazards survival analysis, and the investigator’s global assessment (success/failure) was compared between groups using the χ2 test. Treatment groups were also compared statistically for the overall incidence of adverse events, as well as the incidence of each of the main adverse events. Other data have been summarised only.
Results
PATIENT DISPOSITION
A total of 73 patients (Dysport, 38; Botox, 35) entered the study at seven centres (five Swedish, two Finnish), who recruited totals of 21 (29%), 14 (19%), 12 (16%), nine (12%), eight (11%), five (7%), and four (5%) patients. All patients were treated and there were no withdrawals. Two Dysport patients and five Botox patients completed the study at week 8, and therefore did not have an assessment at week 12.
DEMOGRAPHIC AND OTHER BASELINE CHARACTERISTICS
Table 1 shows a summary of patient demographics, cervical dystonia history, previous toxin treatment, and cervical dystonia symptoms at entry. Overall, the two treatment groups were well matched. The between group difference in Tsui score of 1.1 points suggests that the status of the Botox group may have been slightly worse at entry. Also, a higher proportion of patients were female in the Dysport group, the time since diagnosis of cervical dystonia was slightly shorter in the Dysport group, and fewer Dysport patients had other dystonias or a family history of cervical dystonia. At entry 24 of 38 (63%) patients in the Dysport group were receiving a total of 62 concomitant medications, and 22 of 35 (63%) patients in the Botox group were receiving a total of 44 concomitant medications. The most often used concomitant medications were analgesic, antidepressant, antiepileptic, and neuroleptic drugs, and sedatives. Anticholinergic drugs were used by only three patients in each group.
Demographic and baseline data
STUDY TOXIN TREATMENT
Patients in the Dysport group received a mean (SD) dose of 477 (131) (range 240–720) Dysport units, and patients in the Botox group received a mean (SD) dose of 152 (45) (range 70–240) Botox units. Similar proportions of patients in each group received injections in the sternocleidomastoid (Dysport, 35 of 38, 92%; Botox, 34 of 35, 97%), splenius capitis (Dysport, 36 of 38, 95%; Botox, 30 of 35, 86%), trapezius (Dysport, 25 of 38, 66%; Botox, 23 of 35, 66%), and levator scapulae (Dysport, 17 of 38, 45%; Botox, 12 of 35, 34%). Injection of the sternocleidomastoid, splenius capitis, and trapezius was the most common combination for both groups (Dysport, 14 of 38, 37%; Botox, 11 of 35, 31%).
PRIMARY EFFICACY VARIABLES
The post-treatment Tsui scores showed a between group difference of one point (mean (SD): Dysport, 4.8 (2.4); Botox, 5.8 (2.6)). When adjusted for baseline and centre effects (mean (SEM): Dysport, 4.8 (0.3); Botox, 5.0 (0.3)); the difference of 0.2 points was not significant (p=0.66). The study had 91% power to detect a between group difference of two points.
All Dysport patients and 33 of 35 (94%) Botox patients were re-treated with botulinum toxin at the end of the study. One Botox patient was not re-treated due to suspected pancreatic carcinoma, which was subsequently rediagnosed as pancreatic inflammation. The other Botox patient was not re-treated within the time frame of this study because benefit was still apparent at week 16. The mean time to re-treatment was three days shorter in the Dysport group (mean (SD), range; Dysport, 84 (14), 56–122; Botox, 81 (14), 49–111)), although this was not significant (p=0.85). Including the seven patients (Dysport, two; Botox five) re-treated at week 8, a total of 10 of 38 (26%) Dysport patients and 11 of 35 (32%) Botox patients required re-treatment earlier than the scheduled week 12 visit. Also, five of 38 (13%) Dysport patients and three of 35 (9%) Botox patients were re-treated after week 12.
SECONDARY EFFICACY VARIABLES
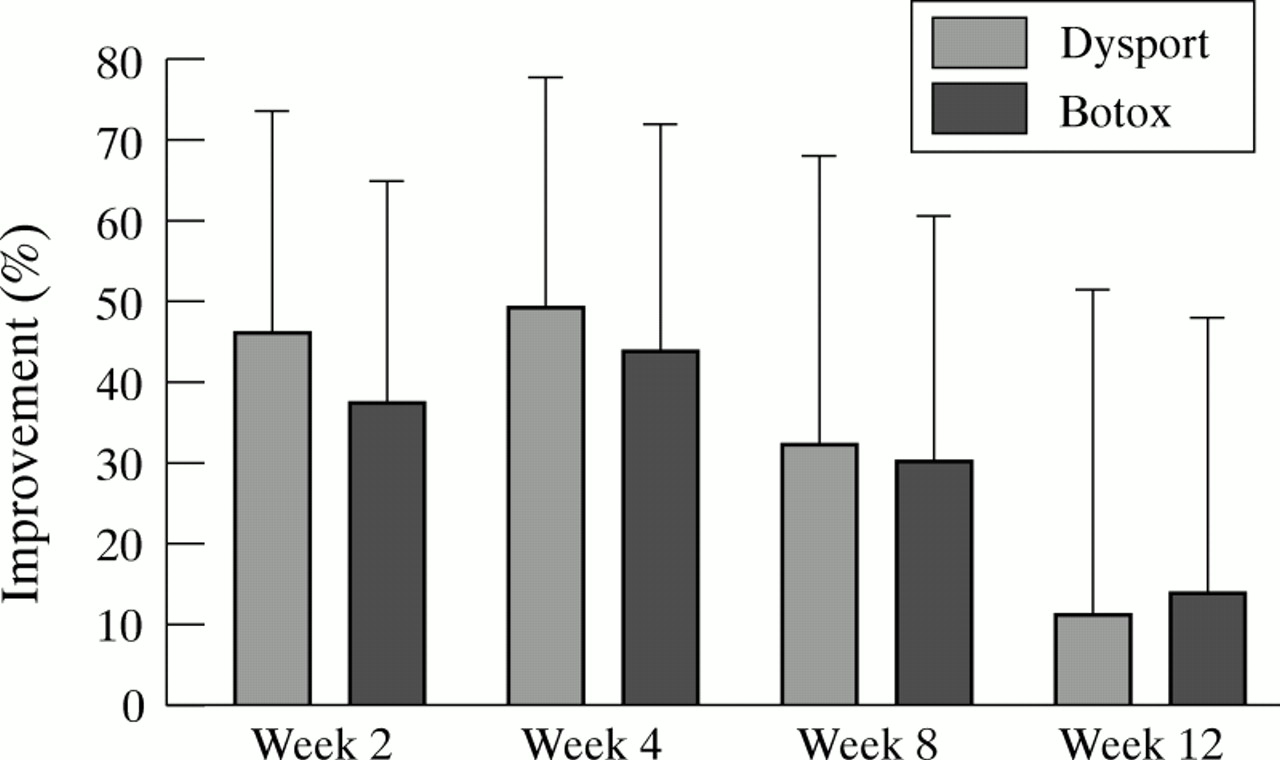
Figure 1 presents the percentage improvements in Tsui score. Despite the difference of 1.1 points at entry, the magnitude and profile of the response to study toxin were very similar for both groups. Tsui scores had greatly decreased at week 2 (mean (SD): Dysport, 4.0 (2.2); Botox, 5.4 (3.0)), with the peak response being found at week 4 (mean (SD): Dysport, 3.8 (2.3): Botox, 4.7 (2.7)). Tsui scores increased at week 8 (mean (SD): Dysport, 5.1 (3.1); Botox, 5.9 (3.0)), and increased further by week 12 (mean (SD): Dysport, 6.2 (2.9); Botox, 7.2 (3.4), but did not reach baseline levels for either group.
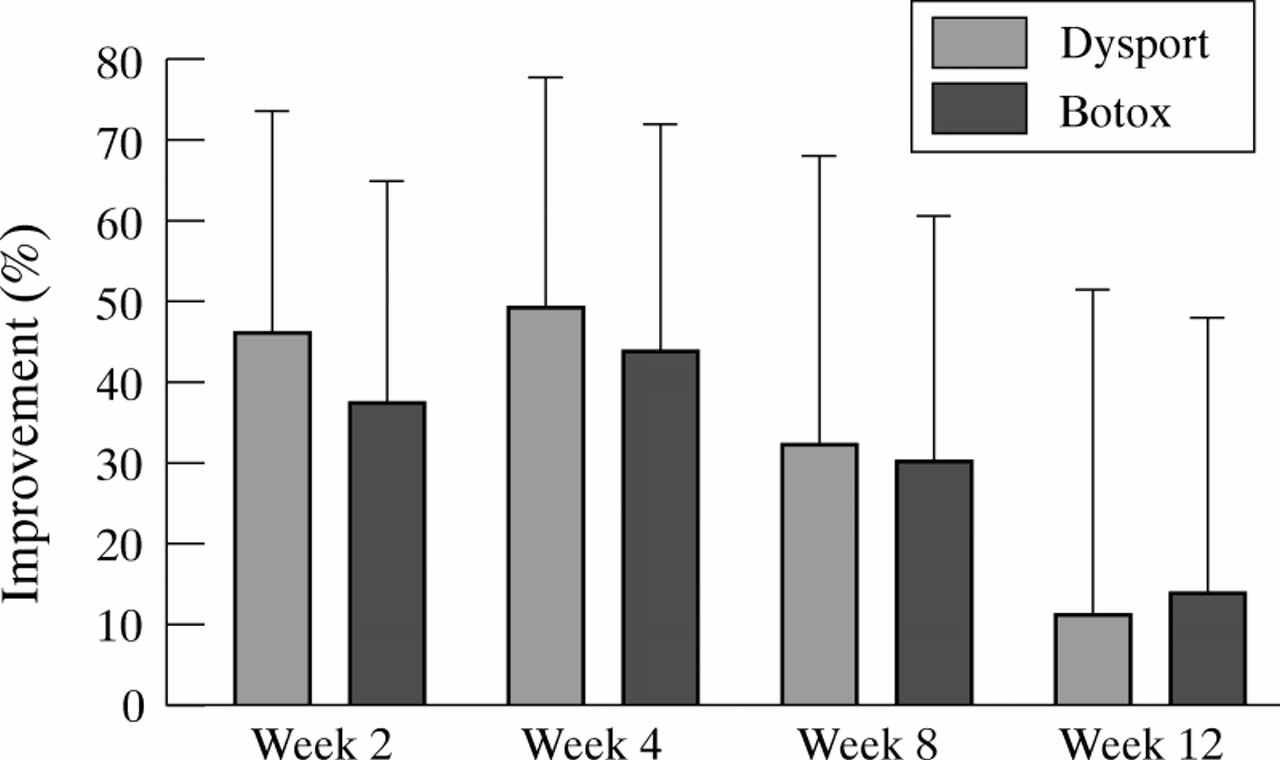
Mean (SD) percentage improvement in Tsui score compared with baseline at weeks 2, 4, 8, and 12.
Figure 2 shows details of the pain associated with cervical dystonia at each visit. Both groups had a similar proportion of pain free patients at entry, and similar proportions reported mild, moderate, or severe pain. The proportion of pain free patients in each group was considerably higher than baseline at week 2, and had decreased almost to baseline levels by week 12. Figure 3 shows investigator assessments of change in cervical dystonia symptoms since entry. Most patients in both groups had improved by week 2 (Dysport, 32 of 38, 85%: Botox, 29 of 35, 83%). Although a similar proportion of patients in both groups still had improved cervical dystonia symptoms at week 4, there were more patients with a greater than 50% improvement in the Dysport group. No patient was considered symptom free at any point during the study. At each visit, investigator assessment of the proportion of patients with improved symptoms, was marginally higher than the proportion suggested by patient self assessment. The response profiles, however, were very similar with the peak effect occurring by week 4, when investigators reported that 63 of 73 (86%) patients had improved, compared with 55 of 73 (76%) patients after patient self assessment.

Patient assessment of the severity of pain associated with cervical dystonia.

{kind=link}
{kind=link}
{kind=link}
Investigator assessment of change in cervical dystonia symptoms since entry.
SAFETY ASSESSMENT
Table 2 summarises adverse events. Overall, 39 adverse events were reported by 22 of 38 (58%) patients in the Dysport group, and 56 adverse events were reported by 24 of 35 (69%) patients in the Botox group (p=0.35). Treatment groups were not statistically different with regard to any individual adverse event (p>0.05). The proportion of adverse events reported as mild (Dysport, 23 of 39, 59%; Botox, 37 of 56, 66%), moderate (Dysport, 14 of 39, 36%; Botox, 18 of 56, 32%), and severe (Dysport, two of 39, 5%; Botox, one of 56, 2%) were similar for both groups. One serious adverse event was reported for a Botox patient after diagnosis of pancreatic cancer, although this was later rediagnosed as pancreatic inflammation. Seven adverse events reported by five Dysport patients, and 10 adverse events reported by eight Botox patients required concomitant medication.
Adverse events
Investigators considered that 14 adverse events reported by 12 of 38 (32%) Dysport patients, and 18 adverse events reported by nine of 35 (26%) Botox patients, were possibly or probably related to the study toxin. Dysphagia (Dysport, six; Botox, four) was the most common toxin related adverse event in both groups. The incidence of adverse events during the first four weeks after study toxin administration was also assessed. Both groups were well matched with 17 of 38 patients (45%) in the Dysport group reporting 27 adverse events, and 18 of 35 patients (51%) in the Botox group reporting 30 adverse events. Dysphagia (Dysport, five; Botox, four) and pharyngitis (Dysport, four; Botox, five) were the most commonly reported adverse events in the first four weeks.
GLOBAL EFFICACY AND SAFETY ASSESSMENT
Although there were a greater number of treatment successes in the Dysport group (29 of 38, 76.3%) compared to the Botox group (23 of 35, 65.7%), the difference was not significant (p=0.32).
Discussion
The effectiveness and safety of Dysport and Botox have been well established in patients with cervical dystonia, and although the potencies of the two preparations are both assessed using a mouse LD50 test, it is clear that one unit of Dysport is not the same as one unit of Botox. Attempts to explain this discrepancy have focused on bioassay technique differences5; however, this does not help physicians determine the clinically equivalent doses of the two preparations.
The results of this study provide substantial evidence that three units of Dysport are clinically equivalent to one unit of Botox. This 3:1 bioequivalence ratio is supported by clinical studies in blepharospasm and hemifacial spasm,6 and also in spasmodic dysphonia.7 Another open study could not detect treatment differences with a 4:1 ratio in patients with blepharospasm and hemifacial spasm.9 There has even been a report10 suggesting the bioequivalence ratio could be as high as 6:1, although this was based on few patients overall, and particularly small numbers of patients receiving Dysport. This is the first randomised double blind study to consider the question of bioequivalence. It is also the first to control for the injection volume, and to apply statistical methodology to the calculation of sample size and the analysis of results.
Non-responsiveness to botulinum toxin is a minor problem, but it was none the less a potential source of error for this study. Consequently, primary non-responders were excluded from the study by the requirement for all patients to have demonstrated a response to botulinum toxin treatment, and the chance of including secondary non-responders was greatly reduced by excluding patients requiring a dose of Botox 100 units more than a previous dose shown to be effective. The dose of botulinum toxin is often adjusted during the first few treatments to define the optimum dose. The requirement for a minimum of four previous toxin treatments, therefore, increased the probability that patients received the optimum dose based on previous clinical experience.
The selection of patients with primarily rotational cervical dystonia reflected the need to ensure a homogenous patient population. Patients with other forms of cervical dystonia, as well as being less common, also require injection of different muscle groups, thereby making comparisons more difficult, especially with regard to side effects. Furthermore, as rotation is a major component of the Tsui score, it could be expected that treatment effects and between group differences would be more easily detected in patients with a primarily rotational cervical dystonia. However, there is no reason to think that the results of this study are not equally applicable to other forms of cervical dystonia.
It is clear from the results of a recent Dysport dose ranging study that patients with rotational cervical dystonia show dose responsiveness between 250 and 1000 Dysport units,11 so although the dose ranges in this study were 240–720 Dysport units and 70–240 Botox units, it is likely that the 3:1 bioequivalence ratio will also apply at dose levels above and below those used in this study.
The duration of the study and the timing of the assessments were determined by the well established pharmacodynamic properties of botulinum toxin in this patient population. The onset of action is usually evident within two weeks of treatment, the peak effect occurs at four to eight weeks, and most patients require retreatment after 10–16 weeks. For both groups, and for all assessments of efficacy, the effect of study toxin was evident at week 2, with a peak effect occurring at week 4. The duration of benefit from study toxin was assessed by recording the time to re-treatment, which ideally is determined purely on the basis of clinical need. However, in reality the time to re-treatment is also influenced by the practicalities of attending out patient clinics, and in this study most patients were re-treated at their scheduled week 12 visit, which may have reduced the possibility of detecting a difference between groups. However, as both groups had similar proportions of patients who were treated earlier or later than week 12 there is no evidence to suggest that either toxin has a longer duration of benefit.
Several rating scales are available for assessing symptoms and signs of cervical dystonia, but there is no generally accepted gold standard.12 The widely used scale described by Tsuiet al 8 shows good interrater reliability, and improvements produced by botulinum toxin have been shown to correlate with subjective efficacy assessments.13 It was therefore considered to be the most appropriate scale for a multicentre study. It should be noted that although interrater reliability was not assessed, all investigators were familiar with the scale, and the study was designed to assess the change in Tsui score after treatment rather than absolute values. The Toronto western spasmodic torticollis rating scale (TWSTRS)12 is a more recent development with potentially higher interrater reliability. A comparison of the Tsui and TWSTRS scales, however, has shown that both adequately assess the improvement of cervical dystonia after botulinum toxin treatment.14 Indeed, the mean Tsui scores at entry in the present study were very similar to that reported by Tarsy,14 suggesting that the choice of patient population and primary efficacy variable were adequate to be able to determine the treatment response to botulinum toxin. It should be noted that the baseline Tsui scores for patients in this study could well have been higher if there had been no prior exposure to botulinum toxin. The sample size was based on the mean post-treatment Tsui score, which was considered to be an appropriate assessment that reflected the time to onset of effect, the peak effect, and also the duration of the effect.
This study was designed to have 90% power to be able to detect a clinically significant between group difference in mean post-treatment Tsui score of two points, and despite having fewer patients than planned the study actually had 91% power. Once adjusted for baseline differences and centre effects the between group difference of 0.2 points was neither statistically nor clinically significant. This study has not shown that the potency of three Dysport units is identical to the potency of one Botox unit. Rather it has provided an indication of the clinical equivalence of the two formulations of botulinum toxin. As the effect of the two toxins was so similar in this study it is unnecessary to determine the ratio that gives identical potency. It would also be impractical as the present study would have required a total of 6812 patients (3406/group) for the between group difference to be statistically significant at the 95% level. Whether a similarly designed study with a different dose ratio would detect significant differences remains to be determined.
After injection of botulinum toxin some patients experience pain or irritation at the injection site, and it is not unusual to find the unintentional weakening of muscles in close proximity to the target muscles. The typical profile of botulinum toxin related adverse events has been shown by large postmarketing surveillance studies as well as smaller clinical trials,11 and includes dysphagia, neck weakness, voice changes, and dry mouth or throat. There have also been reports of more distant adverse events, possibly related to the systemic spread of the toxin, including flu-like symptoms,15 autonomic effects,16 and subclinical disturbance of neuromuscular transmission.17The adverse event profiles found in both groups were consistent with the expected profiles of predominantly local adverse events. Although more adverse events were found in the Botox group over the whole study period, it is noteworthy that the adverse event profiles were well matched during the first four weeks after toxin administration, when adverse events related to toxin would be most likely to occur.
In conclusion, the evidence from this study indicates that patients with predominantly rotational cervical dystonia treated with the clinically indicated dose of Botox or three times that dose in Dysport units show similar improvements and do not have significantly different safety profiles.