Article Text

Abstract
OBJECTIVE To develop a method for the detection of bilateral Horner’s syndrome in patients with bilateral interruption of the cervical sympathetic pathway or widespread autonomic neuropathy.
METHODS Darkness pupil diameters and redilatation times during light reflexes have been recorded with infrared TV pupillometry in 65 healthy subjects, 47 patients with unilateral Horner’s syndrome, and 20 patients with bilateral Horner’s syndrome. The aetiologies of the last group were diabetic autonomic neuropathy (three cases), amyloidosis (four), pure autonomic failure (PAF) (four), dopamine-β-hydroxylase deficiency (two), and one case each of hereditary sensory and autonomic neuropathy (HSAN) type III, carcinomatous sympathetic neuropathy, familial dysautonomia, multiple system atrophy, Anderson-Fabry disease, and anterior spinal artery thrombosis at C5,6 and one had had bilateral cervical sympathectomies.
RESULTS Darkness diameters on the affected side were below normal in 12 patients with unilateral Horner’s syndrome, the measurement yielding only 26% sensitivity for detection of the condition. By contrast, the time taken to reach three quarter recovery in the light reflex (T3/4) was abnormally prolonged (redilatation lag) in 33 of the same eyes. The measurement yielded 70% sensitivity and 95% specificity for detection of the condition. In 20 cases, diagnosed on clinical grounds as having bilateral Horner’s syndrome of various aetiologies, pupil diameters were abnormally small on both sides in five and on one side in three patients. Fourteen of these patients had significant redilatation lag in both eyes, five patients in one eye, and one patient had it in neither eye. Measurement of redilatation lag was therefore a more sensitive diagnostic test than pupil diameter in both unilateral and bilateral Horner’s syndrome.
CONCLUSIONS Provided that the pupils are not tonic, bilateral Horner’s syndrome can be diagnosed on the basis of redilatation lag. It occurs clinically in some generalised autonomic neuropathies and with interruption of the local sympathetic nerve supplies to the two eyes.
- Horner’s syndrome
- pupil
- redilatation lag
Statistics from Altmetric.com
Recognition of Horner’s syndrome due to an ocular sympathetic deficit is usually straightforward if the condition is unilateral and a normal eye is available for comparison. Bilateral sympathetic deficits are, however, hard to detect because the cardinal signs of ptosis, miosis, redilatation lag and diminished responsiveness to cocaine eyedrops are so variable. Such signs may not only be hard to detect clinically but may be absent altogether. In this respect pupil size on its own is of little diagnostic value because only about one third of affected pupils in patients with a unilateral Horner’s syndrome have diameters less than expected from the normal range although they are almost invariably smaller than those of the unaffected eyes.
In this study we have explored the use of redilatation time as an indicator of impaired sympathetic function. The method is based on findings by Lowenstein and Loewenfeld1 which indicate that the peripheral sympathetic system is responsible for dilating the pupil late in the recovery phase of the light reflex. Findings on healthy subjects given guanethidine eyedrops2 and on patients with unilateral Horner’s syndrome3-5 have confirmed the lag that occurs at this point in recovery. We have measured the normal range in healthy subjects and the prolongation associated with sympathetic blockade induced by topical guanethidine. Using the normal range we have defined redilatation lag as a three quarter recovery time which is above the 97.5 centile and on this basis present findings in 47 patients with unilateral Horner’s syndrome and in 18 patients with generalised sympathetic neuropathy with eye signs together with two other patients whose sympathetic supply to the two eyes was interrupted. Such patients seem to have bilateral Horner’s syndrome. Some preliminary findings have been published.6
Subjects and methods
SUBJECTS
Sixty five healthy subjects (40 men, 25 women), mean age 44.1 (range 19–72) years, were recruited to the study. None had evidence of eye disease. Forty seven patients (28 men, 19 women) aged 17 to 75 years with unilateral Horner’s syndrome, and 20 patients (11 men, 9 women) aged 17 to 74 years thought on clinical grounds to have bilateral Horner’s syndrome were studied (table 1). Eighteen of these patients had widespread autonomic dysfunction. The aetiologies were diabetic autonomic neuropathy (three cases), amyloidosis (four), pure autonomic failure (PAF) (four), dopamine-β-hydroxylase deficiency (two siblings), and one case each of hereditary sensory and autonomic neuropathy type III, multiple system atrophy, familial dysautonomia, carcinomatous sympathetic neuropathy, and Anderson-Fabry disease. One additional patient had an anterior spinal artery thrombosis at the level C5,6 with segmental motor signs and marked bilateral ptosis and one had had bilateral cervical sympathectomies for Raynaud’s disease. None of the subjects was taking drugs likely to interfere with pupil function and any with tonic pupils were excluded. Each subject gave consent to participation and approval was given by the ethics committee of West Lambeth Health Authority.
Characteristics of 20 patients with bilateral Horner’s syndrome
TOPICAL DRUG TREATMENT
Local sympathetic blockade was induced on one occasion in six of the healthy subjects by application of one drop of 5% guanethidine in one eye twice daily for 3 days beforehand. In six patients thought to have bilateral Horner’s syndrome adrenoceptor sensitivity of the iris was tested by instillation of 2% phenylephrine eyedrops and the effects compared with previously published data on age matched healthy subjects.7 None of these six patients had dry eyes as a feature of their autonomic neuropathy.
PUPILLOGRAPHY
Pupil diameters were measured in darkness with an Applied Science Laboratories binocular infrared TV pupillometer (Whittaker 1800 model) as previously described.8 Light reflexes were induced with xenon arc illumination, 1 second duration at 10 second intervals, focused in the plane of the pupil, at an intensity sufficient to produce the largest possible reflex for each subject. Redilatation speed was assessed from measurement of the times taken from the peak of the reflex to reach one half (T1/2), three quarters (T3/4) and seven eighths (T7/8) recovery towards the baseline diameter at the onset of the reflex. In each instance, responses were sought to a train of four or five pulses, the first reflex was discarded and measurements obtained on as many as possible of the remainder, averaging where appropriate. In some subjects undergoing pupillography for the first time only one artifact free reflex could be obtained. Evidence of tonic reaction was sought by observing the profile of pupil contraction to continuous light. Pupils showing abnormally slow contractions were excluded.
STATISTICS
Relations between age, pupil diameter, reflex amplitude, and redilatation times, with confidence intervals where appropriate, were assessed by regression analysis using standard methods. Darkness pupil diameter was found to decline significantly with age. Redilatation time was dependent on reflex amplitude alone. In each instance deviations of individual normal values from the lines of best fit were normally distributed. Repeatability of the measurements of T3/4redilatation time was assessed in 11 healthy subjects by recording six light reflexes in each and relating the values found to the value expected on the basis of the amplitude of the individual reflexes. This yielded an average coefficient of variation of 19.2%. Sensitivity and specificity for the detection of Horner’s syndrome by measurement of darkness diameter or T3/4 were calculated by standard methods.
Results
In 65 healthy subjects light reflexes varied in amplitude from 1.20 to 3.48 mm, T1/2 from 0.5 to 2.05 seconds, and T3/4 from 1.15 to 5.00 seconds. The T7/8redilatation time could be measured in only 55 subjects; it varied from 2.30 to 8.50 seconds. All three measures of redilatation time were strongly dependent on the light reflex amplitude (in each case p<0.001), the regression accounting for 72%, 31%, and 19.4% of the variances of T1/2, T3/4, and T7/8 respectively. For each measure, the data with lines of best fit and 95% confidence intervals are shown in fig 1. Redilatation times were not directly influenced by sex or age but a small indirect relation was found between redilatation time and pupil diameter because small pupils tended to have smaller reflex amplitudes. Pretreatment with guanethidine produced no change in T1/2 (1.75 sv 1.02 s; p=0.076) but resulted in marked prolongation of T3/4 (5.08 s v2.28 s; p=0.005) and T7/8 (7.32 sv 3.93 s; p=0.001) times.

Pupil redilatation times (T1/2, T3/4, and T7/8) in 65 healthy subjects. Lines are linear regression lines of best fit with 95% CIs.
On the basis of the published data of Lowenstein and Loewenfeld,1 of the present observed guanethidine response, and the inability to record T7/8 in all subjects, the T3/4 value was taken as the critical redilatation measure for assessment of pupillary sympathetic function in patients. A normal range is presented in table 2.
Normal range of T3/4redilatation times with 95% confidence intervals
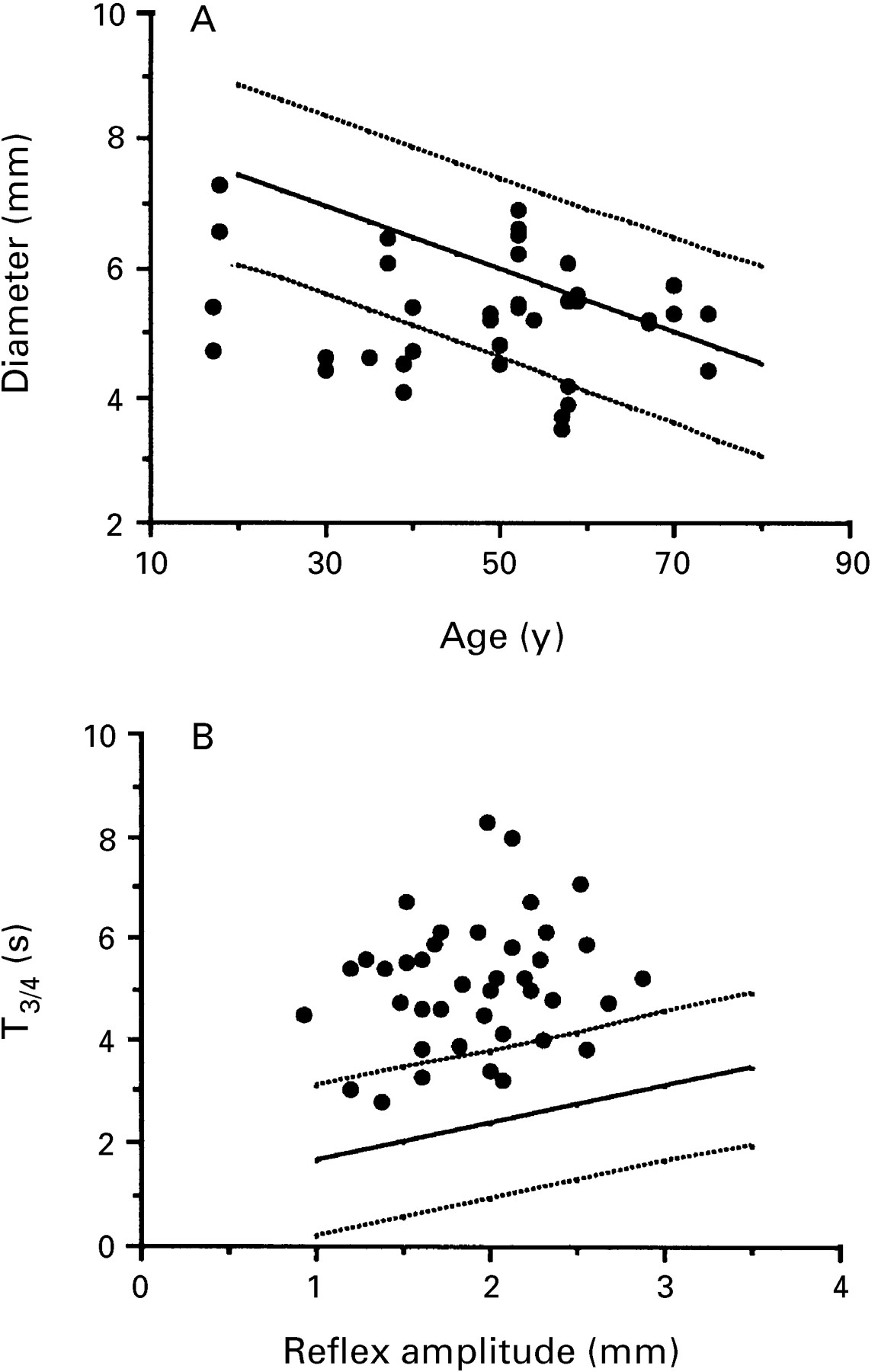
In 47 patients with unilateral Horner’s syndrome the darkness diameter of the affected pupil (5.17 (SEM 0.16) mm) was less than that of the normal pupil (6.09 (SEM 0.15) mm) (p<0.001) but in only 12 cases was it reduced sufficiently to be below the normal range for the patient’s age (fig 2 A). Seven of the 65 healthy subjects had darkness diameters below the normal range. The detection of Horner’s syndrome by measurement of darkness diameter from these data yielded sensitivity of 26% and specificity of 89%. In 33 of the cases of unilateral Horner’s syndrome there was sufficient redilatation lag in the affected eye to take the T3/4 value above the normal upper limit (fig 2B); in 21 instances it was⩾5.0 seconds. By comparison, three of the 65 healthy subjects had values above normal. The detection of Horner’s syndrome by measurement of T3/4, therefore, has sensitivity of 70% and specificity of 95%.

Darkness diameters (A) and T3/4redilatation times (B) of affected pupils in 47 patients with unilateral Horner’s syndrome (symbols as in fig 1).
The pupil diameters and redilatation profiles of the 20 patients with bilateral Horner’s syndrome are shown in fig 3 A and B. The individual findings are summarised in table 3. Five patients had both pupils abnormally small and three had asymetric pupils, one of which was abnormally small. Twelve patients, including three with amyloidosis, one with diabetes, and two with PAF, had both pupils of normal size.
{kind=link}
{kind=link}
{kind=link}
Darkness diameters (A) and T3/4redilatation times (B) of affected pupils in 20 patients with bilateral Horner’s syndrome (symbols as in fig 1).
Summary of pupil findings in 20 patients with bilateral Horner’s syndrome; numbers of patients with abnormally small pupils (miosis) or prolonged T3/4 values (redilatation lag)
In 14 of the patients (70%) both pupils showed redilatation lag with T3/4 values above the normal range. In five other patients only one pupil was affected and in one patient, who was diabetic with small pupils and widespread autonomic neuropathy, no significant lag was present. In 22 pupils the T3/4 value was ⩾5.0 s.
Phenylephrine eyedrop responses were tested in one patient with multiple system atrophy (patient 8), in two patients with pure autonomic failure (patients 13 and 15), in one patient with Anderson-Fabry disease (patient 6), and in two patients with dopamine-β-hydroxylase deficiency (patients 16 and 17). The responses were greater than expected on the basis of the patients’ age (mean (SEM) 3.28 (0.25) v 1.25 (0.15), p<0.001). Ten of the 12 pupils dilated beyond the upper limit of the normal range and were therefore supersensitive.
Discussion
Our results confirm previous findings that redilatation lag in the pupillary light reflex is characteristic of Horner’s syndrome. Using infrared TV pupillometry and a statistically based comparison with dilatation profiles of normal eyes, we have detected it in 70% of affected pupils in patients with unilateral Horner’s syndrome and in 82% of pupils in a selected group of patients thought on clinical grounds to have bilateral Horner’s syndrome. It seems likely that many of these could have been detected clinically for in 45% and 55% of these two groups of eyes the T3/4 time was 5 seconds or more, a level of delay which is readily perceptible to a trained observer. That the proportion of eyes showing significant lag is not higher presumably reflects both the wide variability of this variable within the normal population and the incompleteness of sympathetic block in the affected eyes of the patients concerned.
On the basis of these findings and of the supersensitivity to phenylephrine seen here and previously reported in diabetic patients,7 bilateral Horner’s syndrome seems to be a real clinical entity. It can be found in certain patients with widespread autonomic neuropathy such as occurs particularly in diabetes mellitus, amyloidosis, and pure autonomic failure. Its occurrence and detection inevitably depends not only on a reduction of sympathetic input but also on the persistence of sufficient parasympathetic function to produce a light reflex response. Furthermore, the original findings of Lowenstein and Lowenfeld1 indicate that the peripheral sympathetic nervous system exerts its influence on the redilating pupil only in a reflex of substantial size. Redilatation lag is therefore unlikely to be detectable in patients whose pupils are severely affected by neuropathy of both branches of the autonomic nervous system, when reflexes may be small, such as can occur in diabetes mellitus9 and also presumably in amyloidosis and pure autonomic failure as well as other systemic autonomic neuropathies.
Among the patients with bilateral disease, we excluded any whose pupils were obviously tonic—that is, any in whom pupillary movements were slowed overall—and particularly any in whom the constriction phase of the response to continuous light was abnormally prolonged. Fifteen of these patients had evidence from autonomic function tests of parasympathetic as well as sympathetic dysfunction. It is conceivable that some parasympathetic reinnervation may have occurred in some of these 15 patients and we cannot therefore exclude the possibility that minor degrees of tonicity may have been present, thus contributing to the redilatation lag reported. Because of the rapid constrictor response and the large size of the reflexes obtained, however, a major contribution seems improbable.
The presence of bilateral redilatation lag as part of Horner’s syndrome in autonomic neuropathy is an indication that the eye is affected more by sympathetic than by parasympathetic neuropathy. By contrast, its absence does not imply the absence of a sympathetic deficit. We have recently seen one such patient, a young man whose eyes showed marked ptosis, pupils of mid-diameter with very small light reflexes without redilatation lag but with marked pupillary supersensitivities to both the sympathomimetic agent phenylephrine and the parasympathomimetic agent pilocarpine. It was concluded that he had some features of Horner’s syndrome but that because of the parasympathetic deficit the darkness miosis and the redilatation lag were absent. The absence of miosis in most of the patients reported here may be similarly explained.