Article Text

Statistics from Altmetric.com
The concept of reducing intraocular pressure by way of surgery which preserves the internal trabeculum has recently enjoyed renewed interest.1-4 It mirrors an expanding body of reports proposing non-penetrating surgery as a viable alternative to conventional trabeculectomy in glaucoma management. Central to the appeal of this technique is the avoidance of ocular entry which obviates the need for an iridectomy and theoretically limits early postoperative hypotony. This in turn minimises the attendant sequelae of hyphaema, choroidal effusions, shallow anterior chambers, and cataract.
Non-penetrating surgery is broadly descriptive of two technical approaches. Deep sclerectomy, initially described by Krasnov,5 then Kozlov et al6 in slightly modified form, creates a Descemet's window that allows aqueous seepage from the anterior chamber. Subsequent fluid egress is thought to proceed subconjunctivally, resulting in a filtration bleb, as well as along deeper suprachoroidal routes. Further placement of a collagen implant in the scleral bed has been advocated to help maintain the scleral drainage reservoir.78 The second technique, viscocanalostomy, also requires deep scleral dissection and creation of a filtering window. Ultimate outflow, however, relies on the patency of putative aqueous exit channels, supposedly achieved through identifying and dilating Schlemm's canal using high density viscoelastic. Here, the superficial scleral flap is sutured down tightly, minimising subconjunctival fluid outflow and bleb formation.9
Current debate concerning the role of non-penetrating surgery as a successor to the gold standard trabeculectomy has revolved around its relative effectiveness in short to medium term intraocular pressure (IOP) control and safety.1011 Its justification will, however, have to be judged on the stage of randomised control trials12 that examine longer term IOP control, safety, and visual outcomes. Secondary issues relate to introducing a new surgical technique and involve audit, quality of life and cost considerations, and research into understanding drainage mechanisms so as to provide a rational basis for treatment. Central to this discussion is the need for clear goals and better informed decisions in choosing treatment appropriate to this chronic disease. It is the purpose of this article to judge how far studies on non-penetrating surgery have gone to address these requirements.
Sustained IOP control
Trabeculectomy has been the surgical procedure of choice for treating uncontrolled primary glaucoma since 1967. Prospective randomised control trials have shown that standard trabeculectomy is more effective than medical treatment in reducing IOP over the medium term of up to 5 years.1314 In one trial, Migdalet al found that, after 5 years, mean IOP was 4.4 mm Hg lower after surgery compared with medicine (p<0.0001) and this was controlled below 21 mm Hg in 98% of the surgical group but in only 68% of those treated medically.14
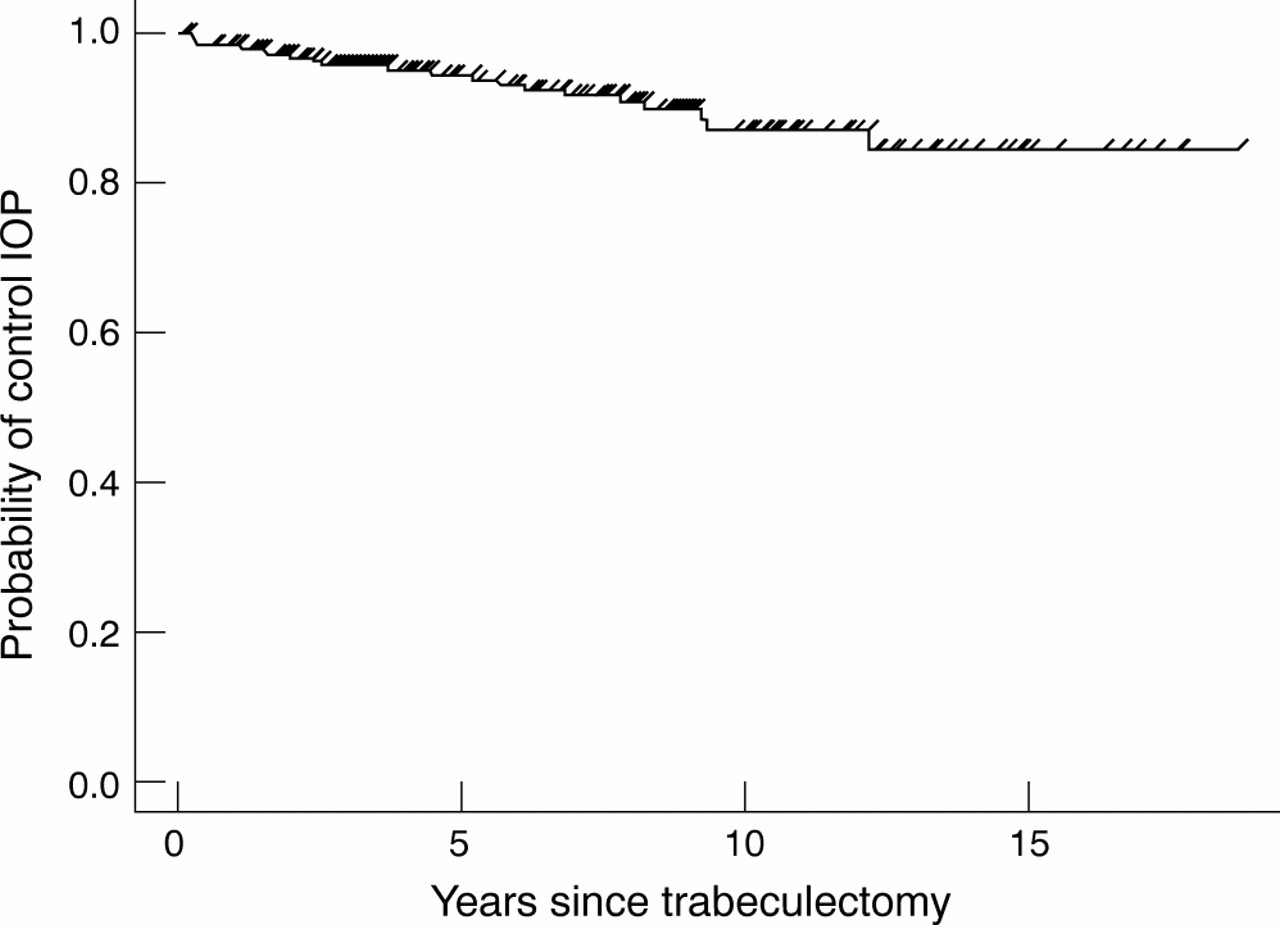
Efficacious interventions in glaucoma should be able to offer long term IOP control in parallel with the disease's chronicity and retrospective studies show that this is achievable with trabeculectomy surgery. Watson et al found that 90% of patients with up to 22 years of follow up after trabeculectomy had IOP levels below 20 mm Hg, with no trend towards increase over time.15 In the same vein, Moltenoet al reported that over a 15 year period, trabeculectomy successfully controlled IOP below 22 mm Hg in 85% of cases (Fig 1).16

Long term control of IOP in trabeculectomy.(Reprinted from Molteno et al,16 with permission from Elsevier Science.)
Comparable long term outcomes do not exist for the newer non-penetrating surgery technique. In the medium term, however, Karlenet al10 found that though initial IOP reduction below 21 mm Hg was universal after deep sclerectomy, this had fallen to 44.6% after 36 months. Subsequently, 41% of eyes required an additional procedure called YAG goniopuncture to restore outflow, while selective use of postoperative 5-fluorouracil applications and topical hypotensive medication was also necessary, suggesting a trend towards rising IOP over time.
Preliminary IOP outcomes over time in non-penetrating surgery studies have been reported and are summarised in Figure 2 by the principal investigator. Results from Carassa,17 Gandolfi (personal communication, Feb 2000), and Lachkar (European Glaucoma Society (EGS) Glaucoma Symposium, 1999) come from randomised control trials, while Demailly and Megevand (both EGS Glaucoma Symposium, 1999), Wishart (UK Glaucoma Society Meeting, 1999), Stegmann et al9 and Mermoud et al10 have reported results from uncontrolled observational series. Figure 2 shows a general pattern of declining IOP control, or rising IOP, with time in non-penetrating surgery. Of note is the marked difference in viscocanalostomy results between Stegmannet al's9 and Carassa's studies.17 The Stegmann study reports a series of viscocanalostomies in black African patients where long term IOP was controlled below 22 mm Hg in 82.7% of subjects without topical medication. The reasons to account for this difference are not clear.

Success of IOP control over time following non-penetrating glaucoma surgery. The symbols represent reported results of separate studies as identified by their principal investigators. There is a trend towards diminished IOP control over time as illustrated by the broken line. ds=deep sclerectomy, visco=viscocanalostomy, ajt=aspiration of juxtacanalicular trabeculum, RCT=randomised control trial.
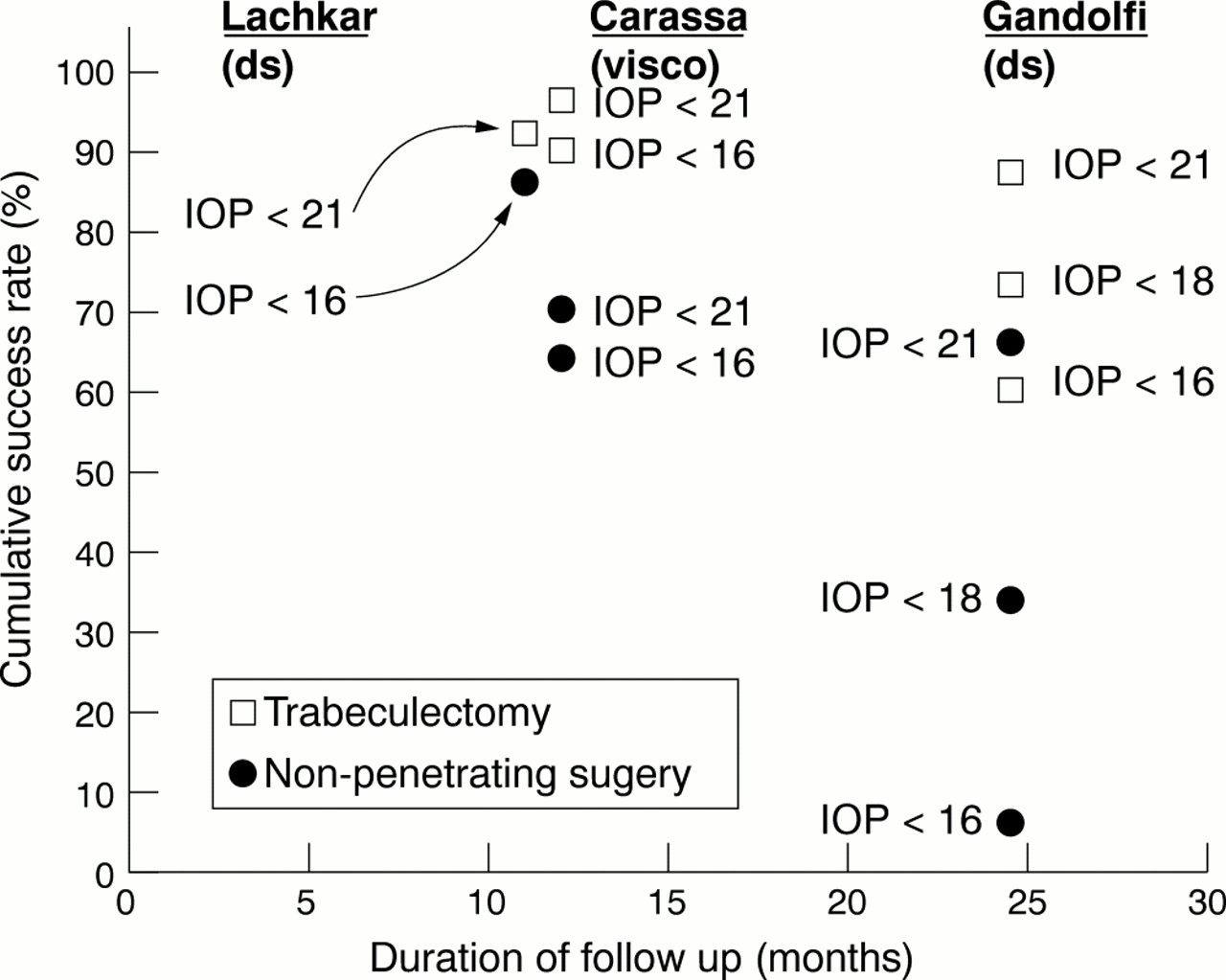
Several centres have randomised control trials under way comparing non-penetrating surgery with standard trabeculectomy. A summary of IOP control over time in these trials is shown in Figure 3. Definitions of IOP success in the Carassa and Gandolfi studies are stratified to include more stringent IOP levels and are in line with modern concepts of control. Early randomised control trials are unanimous in showing that standard trabeculectomy produces lower and better sustained IOP control than either viscocanalostomy or deep sclerectomy. While IOP control diminishes over time in non-penetrating surgery, this is better maintained in trabeculectomy and is in agreement with previously published data.

Randomised control trials comparing IOP control over time for non-penetrating surgery and conventional trabeculectomy. The trials are identified by their principal investigators and definitions of IOP success are stratified in the Carassa and Gandolfi studies. IOP control was better in trabeculectomy at every defined level and time. ds=deep sclerectomy, visco=viscocanalostomy.
Intraocular pressure and visual fields
There is evidence to support the role of sustained IOP reduction by trabeculectomy in preserving visual fields and two randomised control trials are of note. (1) Jay et al18 compared primary trabeculectomy with conventional management over 4.6 years and found significantly greater field loss in the latter group whose mean IOP was higher by 5.8 mm Hg (p<0.001). (2) Migdal et al14found significantly less visual field deterioration in trabeculectomy treated patients with a lower mean IOP of 14.1 mm Hg, compared with laser and medically treated groups with mean IOPs of 18.5 mm Hg (IOP difference: p<0.0001, Fig 4). These studies confirm a trend towards better visual field preservation with lower IOP.

Change in visual fields over time following trabeculectomy, laser, and medical treatment in a randomised control trial.(Reprinted from Migdal et al,14 with permission from Elsevier Science.)
Concerning long term visual outcomes following trabeculectomy, a retrospective study found that despite successful surgical IOP control in 85% of glaucoma patients, the proportion of eyes showing progressive visual field loss more than doubled over 15 years of follow up. Of patients with at least 10 years of post-trabeculectomy follow up, those who had lost visual field had a significantly higher mean IOP than those with stable fields (15.7 mm Hg compared with 14.1 mm Hg, p=0.017).16 These results reaffirm that the incidence of visual field progression may rise with time despite surgically controlled IOP below 22 mm Hg, and show a trend towards better visual field preservation with lower IOP.
Preliminary results from ongoing randomised control trials show that IOP is lower and better sustained over time following trabeculectomy compared with non-penetrating surgery (Fig 2), indicating that trabeculectomy is the preferred procedure where a target IOP in the low teens is deemed necessary for visual preservation.
Risk profile and surgical technique
While it has been suggested that deep sclerectomy results in less hypotony, hyphaema, cataract formation,11 and postoperative flare and cells19 concern has repeatedly been expressed about the steep learning curve associated with this type of surgery.13 One report found that inadvertent perforation of the trabecular meshwork occurred in 30% of initial cases.10 Perforation requires conversion to conventional trabeculectomy which may result in suboptimal flap construction, leading to overdrainage. This particular constellation of problems raises the added spectre of intraocular toxic risk if, as suggested, adjunctive intraoperative antimetabolites are used. Following such conversion, the incidence of postoperative hypotony is reported to be 90% while hyphaema is 68%.20
A commonly voiced concern about trabeculectomy surgery is the risk of late postoperative cataract development. The Collaborative Normal Tension Glaucoma Study, the only prospective randomised control trial to address this issue, showed that cataract developed in 26% of the treatment group (of which 16% occurred in operated eyes) compared with 11% of non-treated group. Duration to cataract formation was 822 days in the former compared with 1200 days in the latter. Both these differences were statistically significant.21 This operation is therefore ripe for supplanting by another with similar primary outcomes but fewer cataract complications. Non-penetrating surgery may be such an operation but to prove its benefit to the patient, reduced cataract incidence needs to be substantiated by a randomised control trial with adequate power.
There is still ambiguity concerning the relative benefits of different non-penetrating operations. This is further complicated by a proliferation of proposed modifications ranging from making multiple perforations, peeling, and aspiration of the remaining trabecular tissue2 to the use of implants derived from materials like collagen78 or crosslinked hyaluronate.22Additionally, the lack of robust data to support any particular variation promotes confusion in a technique already widely acknowledged to be difficult.13 All said, technical difficulty is not in itself insurmountable so long as its potential disadvantages are outweighed by increased efficacy.
Cost and quality of life considerations
There is a growing requirement for the health benefits of new interventions to be verified in randomised control trials in order that their costs may be justified. Viscocanalostomy requires the use of a special disposable cannula and high molecular weight viscoelastic, both of which add a combined £120 ($US 200) to the cost of surgery. In deep sclerectomy, the adjunctive collagen implant is priced at approximately £120,1 significantly more than the application of antiproliferative agents. While this price is justifiable should the implant have proved benefit, there is no clear evidence at present to support its use.823 In addition, the use of different permutations of YAG goniopuncture,24 postoperative 5-fluorouracil, and topical hypotensive medication10 all apparently integral to ensuring success, add further to its price structure.
The expenditure implications of using topical medication, in particular, are lifelong and dwarf those of other initial one-off procedures. To place this in perspective, it has been estimated that the cost of 20 years of medical treatment with necessary monitoring would have amounted to £12 000 ($US 20 000) in 1996 terms, not accounting for possible morbidity associated with treatment.25 In addition, topical medication is not without its own set of drawbacks, not least its ability to induce conjunctival cellular change which may limit the survival of functioning filtration blebs.26 It would appear that an operation which appropriately controls IOP, while obviating the need for other costs, especially ongoing medication, would represent an ideal choice of treatment.
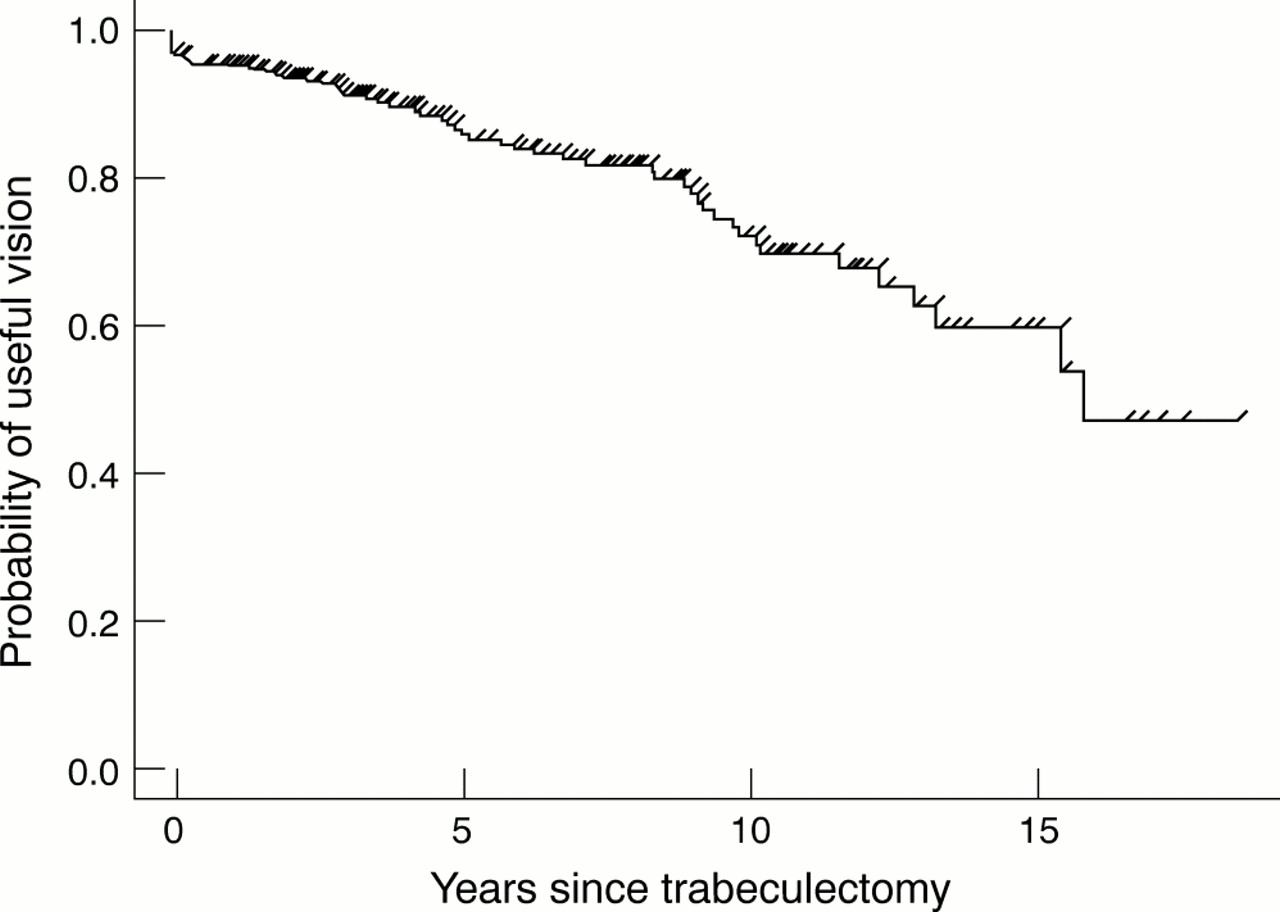
Treatment ultimately seeks to limit visual disability and its potential to restrict quality of life in glaucoma. This quality, measured by functional status and sense of wellbeing, is lower in patients with glaucoma compared with control subjects, and is influenced by visual acuity, visual field impairment, and topical medication use. Cardiovascular disease and other non-vascular systemic disease, both more prevalent in this age group, add further to the impact of reduced visual function on quality of life.27-29 One report found that, despite successful long term IOP control following trabeculectomy, the probability of retaining useful vision declined by 31% over 15 years. Half of visual disability was directly attributable to glaucoma and Figure 5 illustrates its rising incidence over time.16 The minimum challenge facing any new treatment must surely be to maintain such outcomes and do so more efficiently.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probability of retaining useful vision over time following trabeculectomy. Useful vision was defined as visual acuity better than 20/400 and visual field radius greater than 5°. Half of visual disability was estimated to be attributable to glaucoma.(Reprinted from Molteno et al,16 with permission from Elsevier Science.)
Conclusion
The present body of research into non-penetrating surgery has set an early stage on which these operations may be openly and rationally judged as alternatives to the gold standard trabeculectomy. The considerations for justifying new treatments in the context of lifelong disease are many and complex, requiring rigorous assessments that must prove safety and real health benefits over time. More exacting modern concepts would also embody financial and quality of life perspectives. Fundamental questions relating to basic mechanisms of outflow need to be addressed so as to provide a sure premise for treatment as well as pave the way for fresh insights and improvements. Several randomised control trials comparing new and conventional approaches are under way which will, with appropriate follow up, provide a basis for comparison. Current trials are, however, known to have small numbers and this will limit the extent to which these issues can be addressed. Until a larger, possibly multinational study with adequate power is conducted, we may not have sufficient information to justify a change in surgical practice.