Article Text

Statistics from Altmetric.com
A 23 year old man presented with a 10 day history of general malaise and a 1 week history of floaters in both eyes, predominantly in the right. He denied a febrile illness and exposure to animals. General medical history was unremarkable. He was not taking any medications.
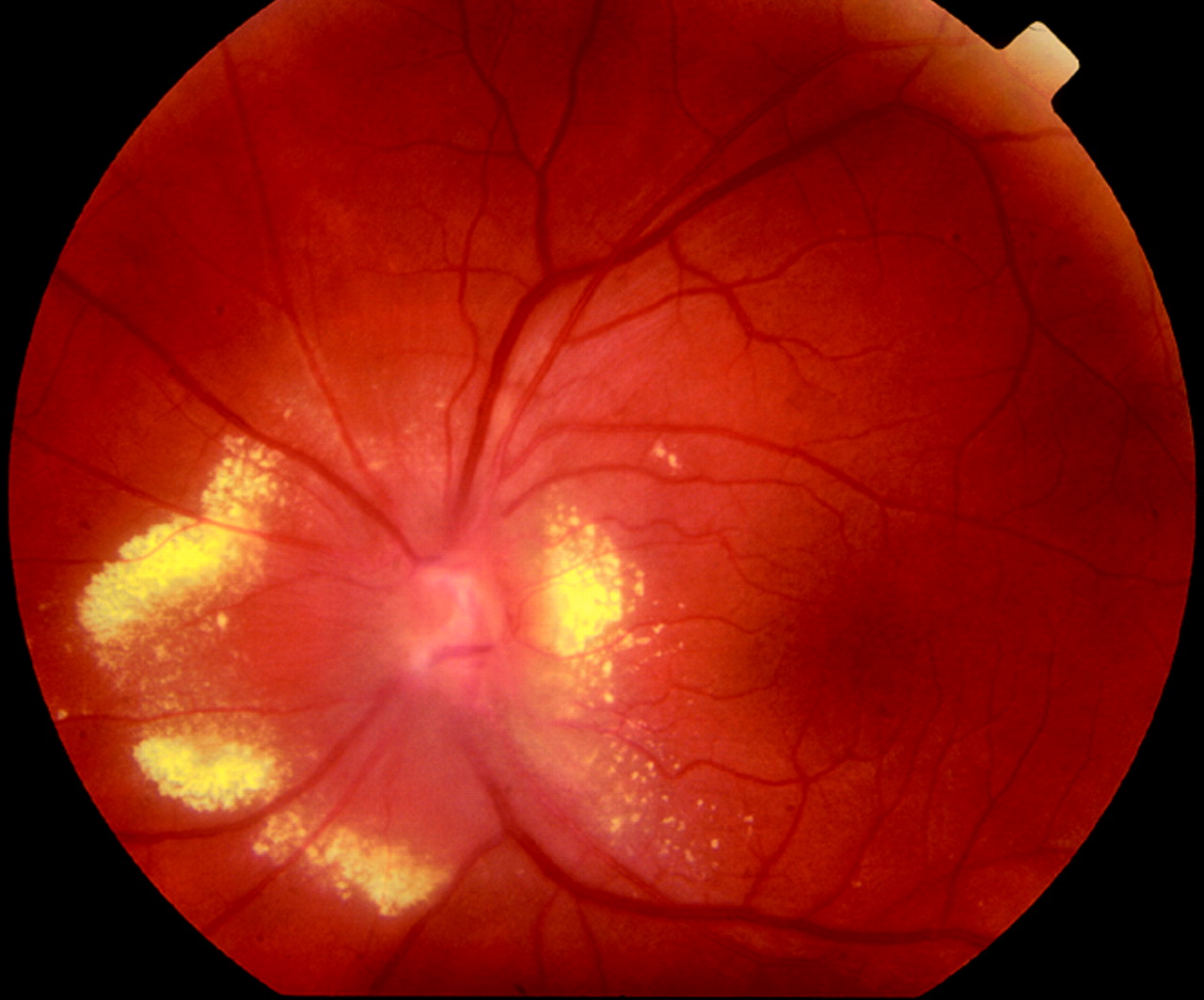
On examination his visual acuity was 6/4-1 in the right eye and 6/4 in the left eye. Anterior chambers were quiet in both eyes. Dilated retinal examination showed 2+ vitreous cellular activity in the right eye and 1+ in the left eye, as well as evidence of bilateral neuroretinitis. The right optic disc was swollen with large dilated tortuous vessels associated with marked gliosis. The lesion was surrounded by lipid exudate and an inferior preretinal haemorrhage (fig 1). In the left eye, there was also a prominent sheathed arteriole superior to the fovea.

Colour fundus photograph of right eye showing papillary aneurysmal lesion with overlying gliosis, peripapillary hard exudate, and inferior preretinal haemorrhage.
Fluorescein angiography in the early phase demonstrated the arterial aneurysmal vascular changes on the optic disc (fig 2). Significant leakage occurred in the mid-phase (fig 3). There was no evidence of retina arteriolar or venular occlusion.

Fluorescein angiography of right eye showing early filling of the arteriolar aneurysmal lesion on the optic disc.

Fluorescein angiography of right eye showing mid-phase peripapillary leakage.
Full blood count with differential, serum electrolyte, C reactive protein, and erythrocyte sedimentation rate results were normal. The serum IgG was slightly elevated (IgG 14.26 g/l, normal laboratory range 6.12–12.93 g/l) and the serum IgA and IgM levels were normal, with a normal serum electrophoretic pattern. HIV serology was negative. Mantoux test, treponemal serology, antinuclear antibody, rheumatoid factor, and sarcoid results were also negative. An orbital computed tomography (CT) scan did not show significant abnormalities.
The diagnosis of cat scratch disease was confirmed by an elevated titre for Bartonella (Rochalimaea) henselae of 1:128 using the indirect fluorescent antibody test.
The patient was treated with 150 mg oral doxycycline twice daily and 100 mg oral rifampicin twice daily. The vitritis settled with prednisone. However the aneurysmal disc changes remained unchanged. At 1 year follow up his visual acuity was 6/6 in both eyes. The left eye subsequently developed marked papillary vasoproliferative changes at 12 months (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Colour fundus photograph of the left eye showing severe papillary vasoproliferative changes at 12 months.
Comment
Cat scratch disease (CSD) is typically a benign and self limiting illness, caused by Bartonella henselae bacteria (previously known as Rochalimaea henselae) lasting 6–12 weeks in the absence of antibiotic treatment. Ocular lesions occur in about 6% of cases.1 This case illustrates the papillary vasoproliferative changes that can occur with CSD. Retinal vascular proliferative changes may be of diagnostic significance and should be sought in patients with ocular CSD.
Ocular manifestations of cat scratch disease include Parinaud’s oculoglandular syndrome, neuroretinitis, optic neuritis, focal chorioretinitis, retinitis, exudative maculopathy, serous retinal detachment, vitreous inflammation,2 and in this report, retinal vasoproliferative lesions. An angiomatous lesion has previously been described in cat scratch disease.3 It has also been known to be associated with central retinal artery and vein occlusion, as well as neovascular glaucoma.4
Doxycycline and rifampicin have been used to treat neuroretinitis in CSD, as they have superior penetration into the central nervous system and eye.4–6 Long term prognosis is usually good, although some patients may acquire a mild post infectious optic neuropathy.6 The prevalence of CSD requires further study but it may be more common than expected in the general population or in patients with idiopathic uveitis.7 Therefore, it is important to look for papillary vasoproliferative changes that may suggest the diagnosis of CSD.