Article Text

Statistics from Altmetric.com
Bevacizumab (Avastin, Genentech) is a recombinant humanised, full length, anti-VEGF monoclonal antibody that binds all isoforms of VEGF-A. It has been shown to prolong survival of patients with advanced colon cancer when combined with 5-fluorouracil.1 In this report, we describe the effect of bevacizumab in two patients with choroidal neovascularisation (CNV) secondary to pathological myopia, which was refractory to other treatment.
Case reports
Patient 1
AM is a 36 year old white man who was diagnosed with subfoveal CNV caused by pathological myopia (right eye = −11.50 D, left eye = −11.50 D) in his left eye in September 2002 for which he received three photodynamic therapy (PDT) treatments. He developed subfoveal CNV in his right eye in June 2003 and received one PDT treatment combined with an intravitreous injection of 4 mg of triamcinolone acetonide. In May 2004, he presented with recurrent subfoveal CNV in his right eye and refused PDT. Off-label use of bevacizumab was discussed and after informed consent, the patient decided to proceed.
Just before treatment in July 2004, best corrected visual acuity (VA) was 20/40 in the right eye and 20/25 in the left eye. There was a ring of hyperpigmentation centred on the fovea with a surrounding ring of subretinal blood and substantial subretinal fluid in the right eye (fig 1A). An optical coherence tomography (OCT) scan through the centre of the fovea confirmed the presence of extensive subretinal fluid (fig 1B, asterisks) with subretinal tissue in the centre of the fovea (arrowheads). An OCT map showed severe thickening and subretinal fluid throughout the centre of the macula (foveal thickness 510 μm, macular volume 9.29 mm3). In the left eye, there were pigmentary changes and no subretinal blood or fluid (foveal thickness, 201 μm). In the right eye, the early phase of a fluorescein angiography (FA) scan showed a central area of hyperfluorescence surrounded by blocked fluorescence from subretinal blood (fig 2A). Central fluorescence increased in the mid phase (fig 2B) and in the late phase the area of hyperfluorescence was larger with indistinct borders indicating leakage of dye into surrounding tissue (fig 2C).

Fundus appearance and optical coherence tomogram of patient 1 at baseline and after starting infusions of bevacizumab.
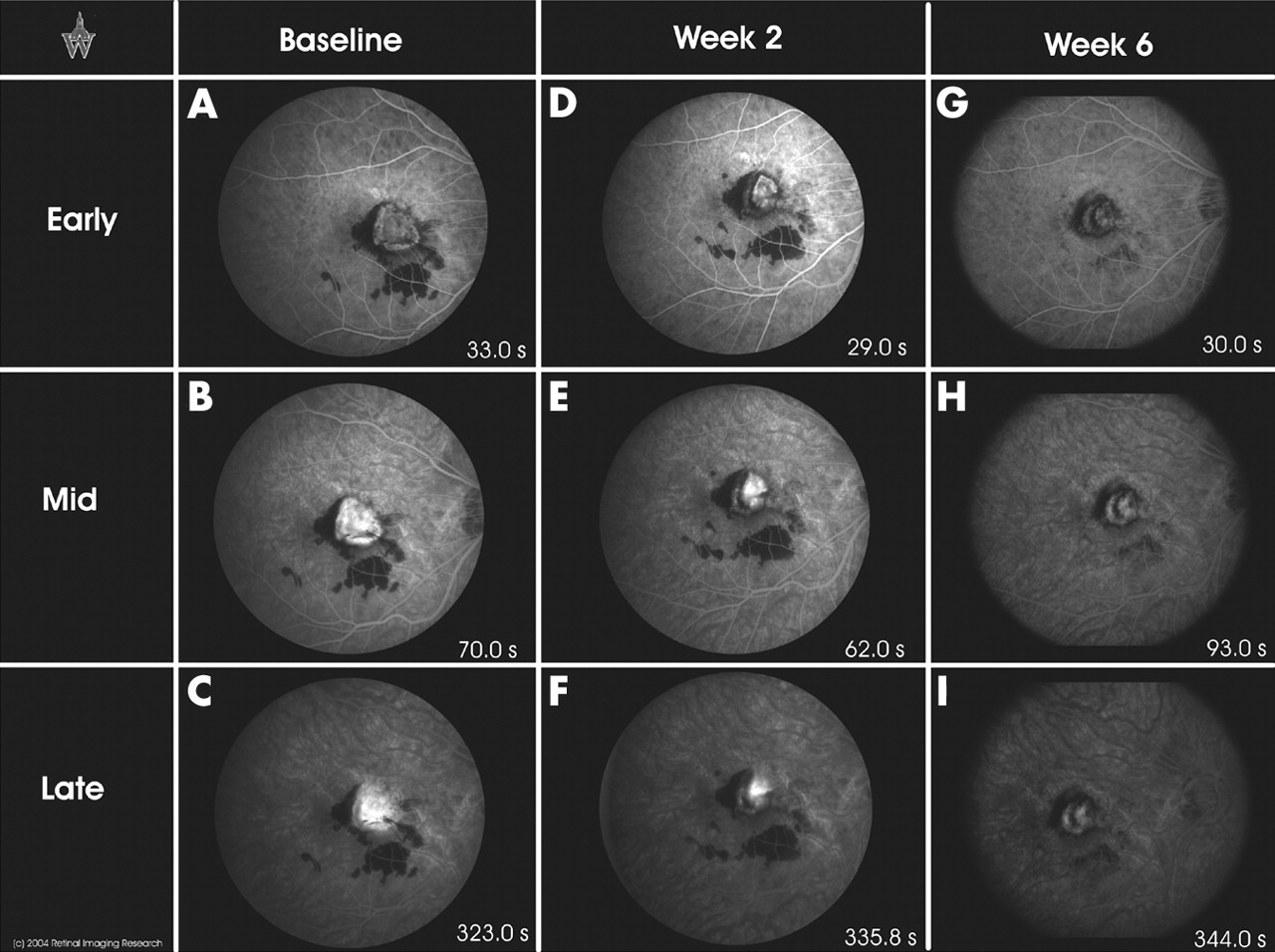
Fluorescein angiography of patient 1 at baseline and after starting infusions of bevacizumab.
The patient received an intravenous infusion of 5 mg/kg of bevacizumab, which he tolerated well. He noted subjective improvement in vision in both eyes within 7 days and 2 weeks after the infusion, VA was 20/20 in both eyes and biomicroscopy showed less subretinal fluid (fig 1C), confirmed by OCT (fig 1D, asterisk). Compared to the pre-infusion OCT, the retinal thickness map showed substantial improvement with a decrease in foveal thickness (330 μm from 510 μm) and macular volume (6.89 mm3 from 9.29 mm3). In the early phase of a FA in the right eye (fig 2D), the hyperfluorescent area was reduced compared to a corresponding frame of the baseline FA (fig 2A). The intensity of hyperfluorescence increased between the early and mid phase (fig 2E) and there was evidence of dye leakage from the CNV during the late phase (fig 2F). The patient received second and third infusions of 5 mg/kg of bevacizumab without any difficulty. Six weeks after the first infusion and just before the fourth infusion, VA was 20/20 in each eye and biomicroscopy showed no identifiable subretinal fluid in the right eye and resorption of almost all of the subretinal blood (fig 1E). OCT confirmed that there was no subretinal fluid (fig 1F) and the retinal thickness map showed further improvement compared to the map after the first infusion. Foveal thickness measured 244 μm and macular volume was 5.80 mm3. Early phase of the FA showed further reduction in the area of hyperfluorescence (fig 2G) compared to a corresponding frame of the FA done after the first infusion (fig 2D). There was only a mild increase in brightness of the hyperfluorescent area in the mid phase of the FA (fig 2H) and sharp borders with no further increase in brightness in the late phase (fig 2I). This indicates that there was little collection of dye within the CNV and no leakage into surrounding tissue—two favourable signs. Nine months after the fourth infusion, the patient was asymptomatic and visual acuity was 20/20 in each eye. FA showed no evidence of leakage in either eye.
Patient 2
LL is a 52 year old white woman with pathological myopia (refractive error −17.75 sphere and −18.75 + 0.75×165). The left eye developed subfoveal CNV in February 2002 and the patient had six PDT treatments with the last in January 2004. The right eye developed juxtafoveal CNV and was treated with photocoagulation in April 2002. Recurrent CNV occurred beneath the fovea and was treated with PDT on two occasions, the most recent in January 2004.
The patient presented in July of 2004 complaining of progressive loss of vision in both eyes. Visual acuity was 20/100 in the right eye and 20/200 in the left eye. In the right eye, there was a laser scar between the disc and the nasal border of the fovea. There were flecks of subretinal haemorrhage and mild subretinal fluid. In the left eye there was hypopigmentation surrounded by a ring of hyperpigmentation with subretinal fluid, blood, and thickening in the macula (fig 3A). OCT in the left eye showed prominent retinal thickening surrounding a small central area of retinal atrophy (fig 3B, arrow). The retinal thickness map showed the thickest region of the retina to be located on the inferotemporal side of the fovea. Foveal thickness was 311 μm and macular volume was 7.30 mm3. In the right eye, OCT showed retinal thinning in the region of the laser scar inferonasal to the fovea (fig 3C, arrows), and thickening superotemporal to the fovea with a pocket of subretinal fluid (asterisk). Foveal thickness was 296 μm and macular volume was 5.91 mm3. There was subfoveal CNV in both eyes, and it was decided to transit the left eye because there was more retinal thickening in the left eye. The early phase of the FA showed a central area of hyperfluorescence and surrounding blocked fluorescence from subretinal blood (fig 4A). The hyperfluorescence became much brighter during the mid phase of the FA (fig 4B) and leaked during the late phase (fig 4C). The patient refused additional PDT and after careful consideration of potential risks and benefits and signing a consent form, the patient was given four intravenous infusions of 5 mg/kg of bevacizumab at intervals of 2 weeks, which she tolerated well.

Fundus appearance and optical coherence tomogram of patient 2 at baseline and after starting infusions of bevacizumab.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fluorescein angiography of patient 2 at baseline and after starting infusions of bevacizumab.
Examination before the fourth infusion showed a VA of 20/64 in the right eye and 20/200 in the left eye. Biomicroscopy in the left eye showed reduced subretinal blood compared to the baseline examination, but persistent macular thickening (fig 3D) confirmed by OCT, which showed a foveal thickness of 304 μm and a macular volume of 7.37 mm3. In the right eye, there was mild residual subretinal fluid and a few flecks of subretinal blood temporal to the laser scar. OCT in the right eye showed reduced retinal thickening and minimal subretinal fluid with foveal thickness of 249 μm and a macular volume of 5.78 mm3 (fig 3F). In the left eye, early phase of a FA (fig 4D) showed a similar area of hyperfluorescence as that seen in the early phase of the baseline FA (fig 4A), but substantially less fluorescence during the mid (fig 4E) and late (fig 4F) phases than the corresponding phases of the baseline FA, indicating less filling of the CNV with dye. There was still substantial leakage of dye into surrounding tissue in the late phase (fig 4F). The patient returned 2 months after the fourth infusion noting subjective visual improvement that had allowed her to resume many activities that she had previously stopped. VA was 20/64 in the right eye and 20/200 in the left. Contact lens biomicroscopy in the left eye showed no identifiable subretinal blood or fluid, and macular thickness appeared reduced (fig 3G). This was confirmed by OCT (fig 3H; foveal thickness 253 μm, macular volume 6.40 mm3). In the right eye, there was no identifiable subretinal blood or fluid and OCT showed no changes from the scan at week 6. FA in the left eye showed reduced hyperfluorescence compared to previous FAs at all phases, early (fig 4G), mid (fig 4H), and late (fig 4I), and no leakage.
Comment
In two patients, intravenous infusions of bevacizumab resulted in reduced fluorescein angiographic evidence of leakage from CNV and decreased retinal thickening and subretinal fluid. This anatomical evidence of improvement was accompanied by visual improvement in two of the three eyes in which there was active subfoveal CNV at baseline. The one eye that did not show objective evidence of visual improvement had prominent subretinal fibrosis and a central area of retinal atrophy at baseline. Although spontaneous improvement cannot be ruled out with certainty, the course of these two patients suggests that antagonism of VEGF with bevacizumab provided benefit. No ocular or systemic side effects were observed.
Recent studies have suggested that VEGF may be an important stimulus for neovascular age related macular degeneration (AMD).2,3 Despite differences in pathogenesis among the disease processes, the effect of bevacizumab in the two patients reported here suggests that VEGF may be an important stimulus for CNV in pathological myopia as well as AMD. While uncontrolled observations in two patients do not justify widespread use of bevacizumab in patients with CNV, additional studies are warranted. A controlled clinical trial is needed to determine if bevacizumab is safe and effective in patients with subfoveal CNV caused by pathological myopia and, if so, to determine the appropriate frequency of administration.
Linked Articles
- Correction