Article Text

Statistics from Altmetric.com
A recent paper by Kobayashi and co-workers1 on temporary amniotic membrane patching for acute chemical burns highlights the difficulty in the consistent classification of this type of injury.
Roper-Hall’s classification of acute chemical injuries to the eye is based on the original classification of Ballen2,3 and there is little difference between them. However, in neither classification is the grade based on the most severe sign. This immediately leads to the problem of trying to classify an eye having, for example, corneal signs of one grade and conjunctival signs of another. There is also difficulty in grading the conjunctival and limbal injuries.
Dua et al4 recognised the problem of assessing limbal stem cell damage and proposed a quasi-analogue scale in order to incorporate intergrade variations. They suggested using limbal fluorescein staining as a marker of limbal stem cell damage. However, their grading scheme is complex and departs significantly from that of Roper-Hall. Although fluorescein staining is a useful sign, it does not necessarily imply limbal stem cell damage or failure and has not been shown to be a better index of limbal damage than perilimbal ischaemia. Importantly, it is also becoming apparent, that both the fornices and mucocutaneous junction of the conjunctiva are important for conjunctival regeneration.5–7 In fact, Roper Hall stressed the importance of involvement of contiguous areas of the conjunctiva, which may lead to symblepharon formation.4
Although there are limitations with Roper-Hall’s classification, it is simple and remains popular. Rather than replace Roper-Hall’s and Ballen’s classification,2,3 we suggest a modification, which addresses some of the issues raised and makes the classification more robust.
One of the questions that needs to be answered is whether to base the grade of injury upon the most severe sign or on a combination of ocular surface signs. A combination of signs using three parameters (cornea, limbus, and conjunctiva), each with three levels requires 27 possible combinations to avoid crossover. To avoid this complexity and without evidence to indicate a difference in prognosis, it would seem reasonable therefore to base the grade of injury on the most severe sign.
Although limbal ischaemia does not necessarily imply limbal stem cell failure, it remains to be shown that it is less indicative than fluorescein limbal staining of limbal damage. We propose therefore to continue to use limbal ischaemia in the grading of injury.
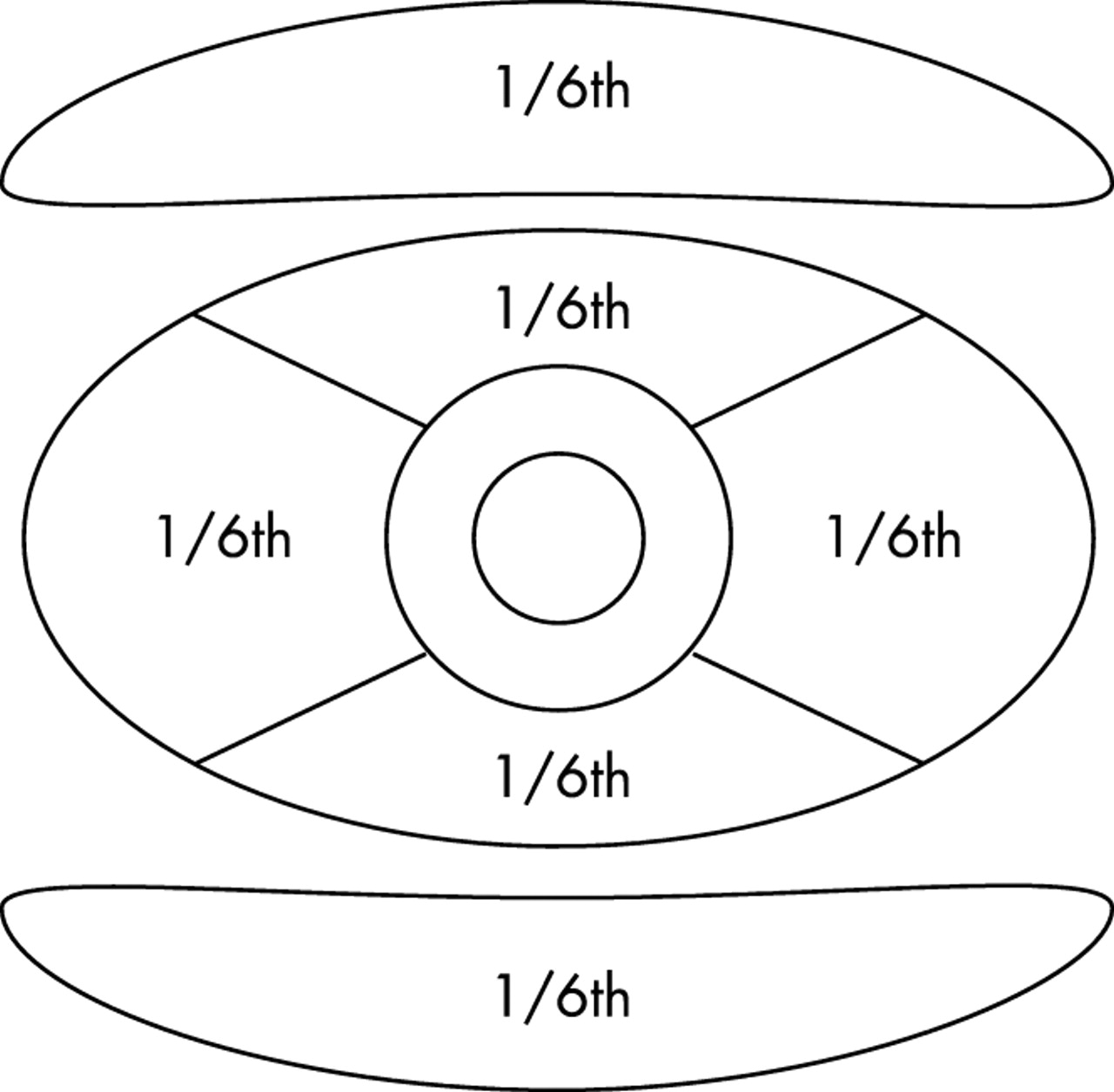
With regard to conjunctival involvement, in order to be able to include the total area of involvement, we suggest dividing the conjunctival surface into bulbar and tarsal areas, as is natural. The bulbar and tarsal conjunctiva comprise approximately two thirds and one third of the total conjunctival surface respectively. Using conjunctival fluorescein staining as an indicator of the extent of conjunctival damage, the area of involvement can be based on the fraction of the third involved, limiting any division into not less than sixths—that is, the tarsal surfaces together comprise a third of conjunctiva (see fig 1). This includes the issue that a vertical distribution of conjunctival injury is as important as a horizontal distribution.
{kind=link}
Estimation of conjunctival injury. For example, 1/6th+1/6th = 1/3rd.
Corneal involvement in terms of prognosis remains an area of difficulty. Although it may be assumed that limbal and conjunctival damage implies a worse prognosis than isolated corneal damage, this has yet to be shown. In addition, a severe chemical injury involving the cornea but not the limbus, or vice versa, would be expected to be an uncommon event. We therefore propose to retain the degree of corneal damage (as proposed by Roper-Hall2 and Ballen3) in grading of the injury (see table 1).
Modified classification of ocular chemical injuries
Thus, grade I is identified by any isolated corneal epithelial injury. Grade II includes limbal or conjunctival involvement, but involves less than one third of the area involved. Grade III includes either a hazy cornea, defined as obscurity of the iris or pupil details (as per Roper-Hall’s and Ballen’s original descriptions), and/or greater than one third of limbal or conjunctival damage. With the advent of recent surgical techniques such as amniotic membrane transplants and limbal allografts, the prognosis of more severe ocular chemical injuries previously classified as Roper-Hall grade IV have improved and no longer carry a uniformly poor prognosis.2 Therefore, we reason that these cases can be included in grade III of our proposed classification.
In conclusion, in the absence of good evidence for re-classifying ocular surface injuries, it would seem reasonable to keep to the Roper-Hall/Ballen classification and to move it forward by addressing the weaknesses of that system. We hope that the proposed grading system improves the consistency with which chemical injuries are reported in the literature, serves as a basis for controlled comparative evaluation of modern treatment, and stimulates further work in this area.
References
Author’s response
The response by Harun et al is to be commended in so far as it highlights the problems with the current Roper-Hall classification system and the difficulties it poses in evaluating outcome and efficacy of treatments in ocular surface burns. As a proposed modification, however, it is a retrograde step.
The three major issues with the Roper-Hall1 classification were that it lumped all injuries with 50% or more of limbal involvement into one category, did not take into account conjunctival involvement in the actual classification, and placed undue emphasis on the degree of corneal haze.
The proposed modification by Harun et al goes a step backwards by grouping all injuries with more than 33% limbal involvement into one category. The grading of a patient with all 12 clock hours of limbus involvement would then be the same as one with just over 3 clock hours of limbus involvement! The prognosis given to these two patients cannot be the same, given that the Roper-Hall and the Dua, King, and Joseph2 classifications are prognostic classifications. Furthermore, a patient presenting with less than one third limbus involvement does not necessarily come with less than one third conjunctival involvement, which could be much more. The proposed modification does not allow for such variances, which are frequent. The Dua, King, and Joseph classification has the flexibility to allow for such variables and also to progressively document change both improvement and deterioration, over the acute phase of the injury. The authors rightly point out that the degree of ischaemia does not always correspond to degree of limbal involvement. Yet limbal involvement without ischaemia, in the form of loss of stem cells, can have an equally important impact on prognosis. That is precisely why the Dua, King, and Joseph classification considers limbal involvement (to encompass ischaemia as well) rather than limbal ischaemia alone.
The point about conjunctival involvement is well made in the proposed modification. This does not differ significantly from the Dua, King, and Joseph classification. The latter was the first to take this aspect of burns into account in determining severity and prognosis. The authors mention the importance of tarsal conjunctival involvement. This is a valid though often an impractical consideration. Associated swelling, induration, thickening, shrinkage and the like, of the lids make tarsal conjunctival evaluation impractical if not impossible in some cases, in the immediate post-injury period. It was for this practical consideration that the Dua, King, and Joseph classification included only the extent of bulbar conjunctival involvement in determining the grade. It is interesting to note that the authors disregard limbal fluorescein staining as an indicator of limbal damage (as proposed in the Dua, King, and Joseph classification) but propose fluorescein staining as an indicator of conjunctival damage in evaluating extent of conjunctival damage. This implies that fluorescein staining is appropriate to evaluate both conjunctival epithelial damage and conjunctival ischaemia but not limbal epithelial damage and limbal ischaemia. There is no rationale for this.
Corneal haze can be an indicator of the offending chemical rather than the severity of the insult. It is not uncommon to find a clear and transparent cornea, which is totally denuded of its epithelium, immediately after a chemical injury. This can stay so for a few days before becoming rapidly hazy or opaque, or remain clear and become re-epithelialised. Corneal endothelial damage leading to stromal oedema and haze can occur later in the course of an acute chemical injury. Conversely, a hazy cornea with a resultant scar could do well following a corneal graft procedure if the limbal involvement is minimal. The proposed modification retains corneal haze as a grading parameter and includes a hazy cornea in grade 3 only. There are many chemical injuries, which involve 3–6 clock hours of the limbus (30–50%) with a clear cornea. These do not fall well in any grade in the proposed new classification and highlight the inherent problem in the Roper-Hall classification and its proposed modification.
Most important of all, the proposed classification is purely theoretical and has not been validated. The Dua, King, and Joseph classification is based on several years of clinical experience of managing burns including more than 67 patients. It is simple and easy to use (clock hours of limbus involvement and percentage of conjunctival involvement), flexible, and allows for all combinations of different extents of involvement of the two structures. It is validated as a prognostic indicator and allows for accurate comparison of cases. The proposed new classification/modification fails on all these counts.