Article Text

Abstract
Descemet membrane endothelial keratoplasty (DMEK) allows for selective replacement of damaged endothelial cells, using only donor Descemet's membrane with endothelium. However, early adoption by corneal surgeons has been limited (illustrated by graft registry reports: 0.7% all corneal transplants in the USA; 0.4% in Australia for 2011) due to challenges in donor preparation and surgical technique. Recently, innovative donor preparation techniques may improve availability of pre-stripped DMEK donors from eye banks. The refinement of donor insertion and manipulation techniques has also improved outcomes and reduced graft detachment rates—still, the most common postoperative complication following DMEK. Randomised studies are needed to compare clinical practices and surgeon preferences, such as intraoperative use of long-acting gas, early versus late intervention of graft detachments and postoperative steroid management. A review of current literature reveals that most publications to date are reports from similar study cohorts by surgeons who pioneered and advocate this technique. Thus, more long-term clinical studies in other tertiary centres are required in order to confirm if the purported advantages of DMEK such as improved visual outcomes and reduced graft rejection are replicable among most corneal surgeons.
- Cornea
Statistics from Altmetric.com
Introduction
The concept of selectively replacing damaged endothelial cells (ECs), in the form of endothelial keratoplasty (EK), has revolutionised corneal transplantation.1 Patients suffering from endothelial dysfunction are now able to benefit from a surgery, which has a more rapid visual recovery, better refractive outcome and superior tectonic integrity, compared with the traditional full-thickness or penetrating keratoplasty (PKP).2–5 Over the years, EK techniques have also evolved to be more selective in the layers of corneal replacement: from a stromal layer with endothelium and Descemet's membrane (DM) for deep lamellar endothelial keratoplasty (DLEK),1 to a thinner stromal layer in Descemet stripping endothelial keratoplasty (DSEK);6 and more recently, Descemet membrane endothelial keratoplasty (DMEK), where only endothelium and DM is replaced (figure 1).7 ,8
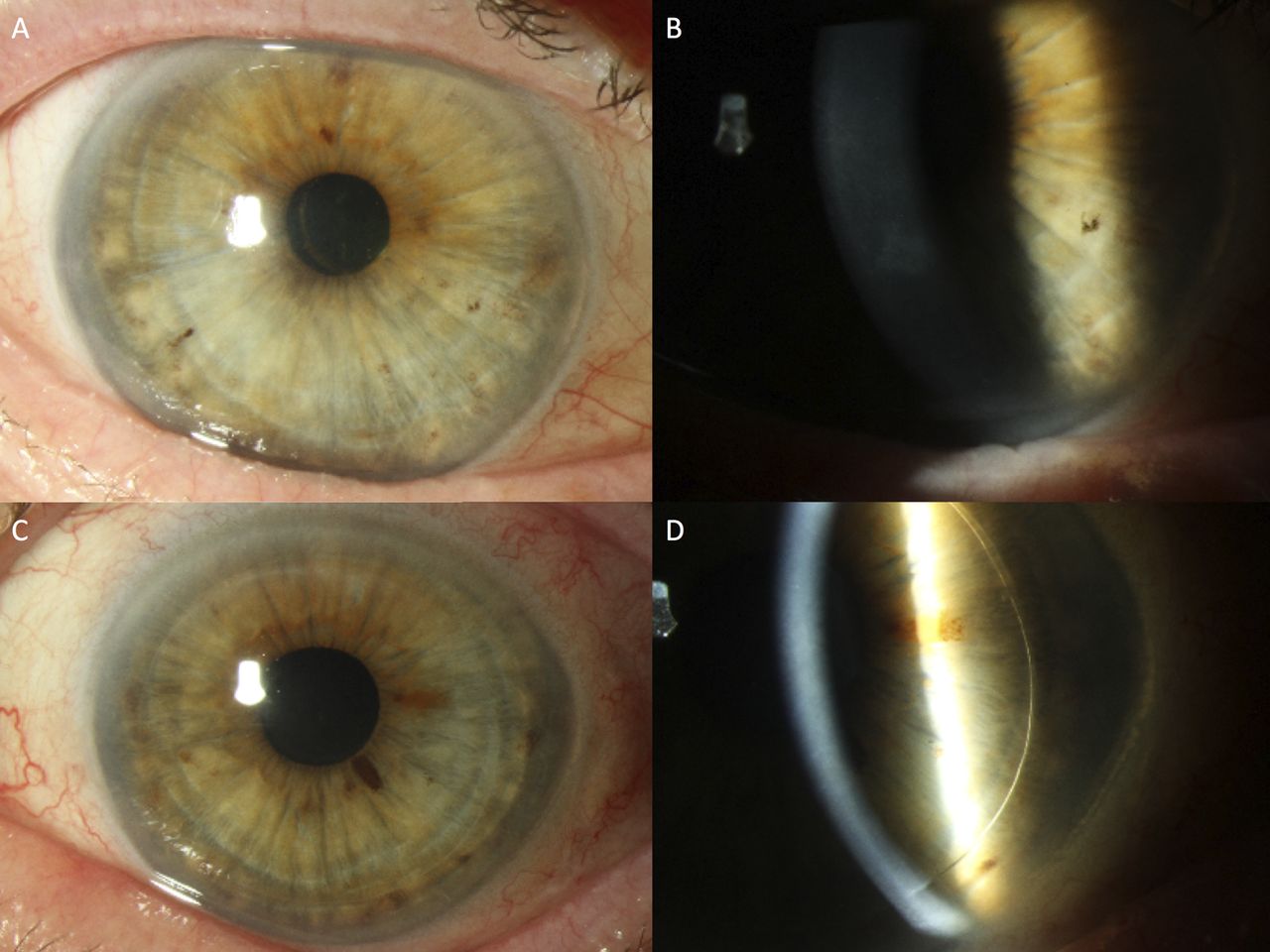
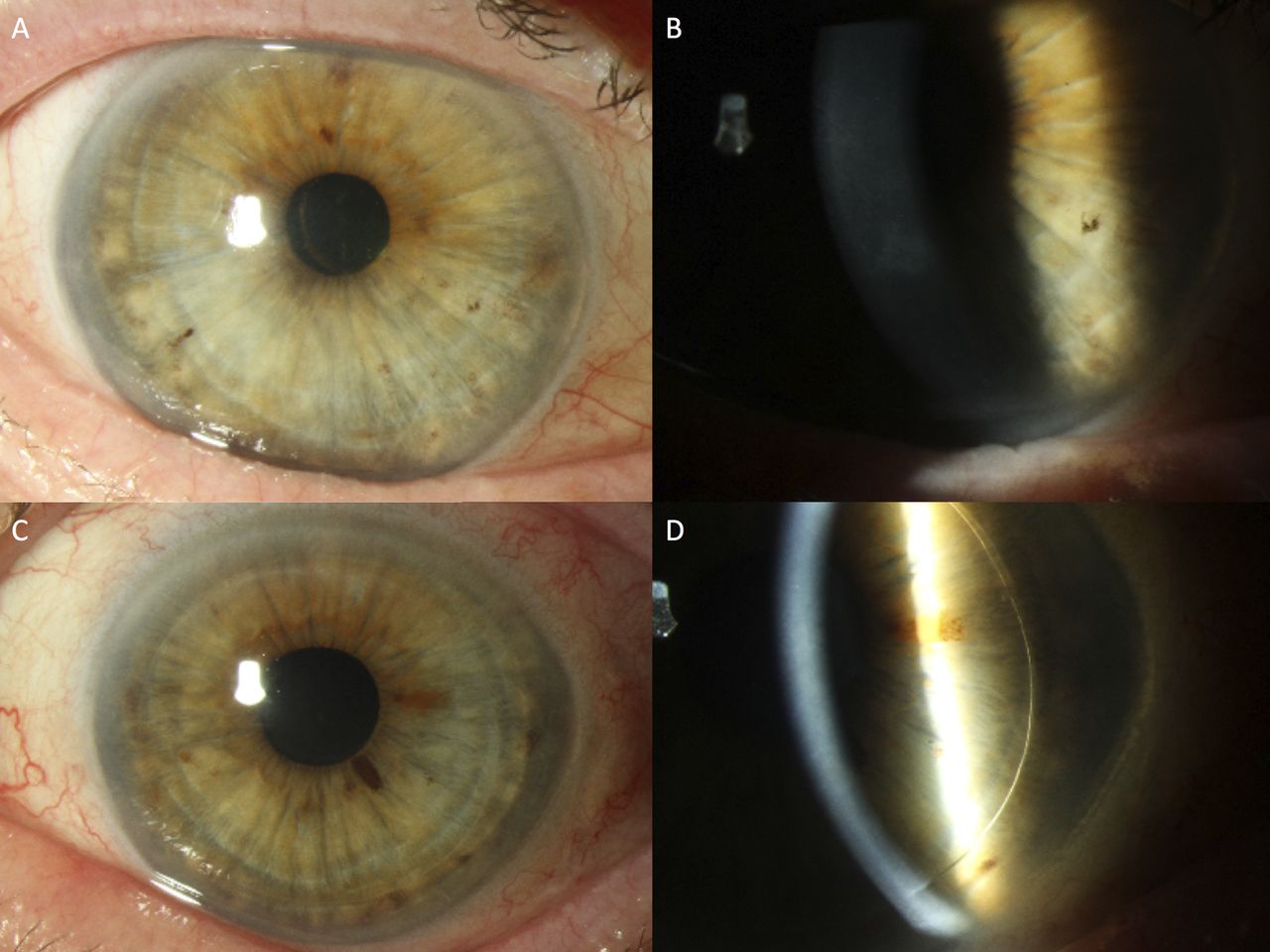
Postoperative slit-lamp photographs comparing endothelial keratoplasty techniques. (A) Descemet membrane endothelial keratoplasty. (B) Descemet membrane endothelial keratoplasty with graft edge barely visible. (C) Descemet stripping automated endothelial keratoplasty with visible graft edge.
Once surgical techniques and donor preparation methods by eye banks were refined and implemented, Descemet stripping automated endothelial keratoplasty (DSAEK) became the main EK technique that rapidly gained popularity among surgeons.9 ,10 While DSAEK enjoyed all the benefits of EK surgery over PK, the posterior corneal stroma in DSAEK donors often contributed to hyperopic shift and, in some cases, suboptimal visual recovery.11–14 DMEK is a more anatomically accurate procedure that just replaces DM and endothelium,1 potentially leading to a more rapid, and better visual recovery with minimal refractive change.15–20 However, widespread adoption is currently highly limited due to the relative difficulty of donor preparation, the overall challenging surgical technique and seemingly increased early complications.21 The 2013 Eye Bank Association of America report revealed that although the USA has firmly adopted DSEK, which comprised 48.7% of all grafts performed in the USA (and exceeded that of elective or optical PK surgeries, which comprised 42.8% of cases), DMEK was only performed in 3.2% of cases. However, the report also noted that the total number of DMEK cases performed in the USA, although small, had more than doubled compared with the previous year—from 0.7% in 2011 to 1.6% in 2012 and 3.2% in 2013.22 The 2012 Australian Graft Registry reported that only 0.4% of all grafts performed from 2010 to 2011 were DMEK surgeries.23
In 2006, when Melles first introduced the concept of DMEK, he declared that ‘neither DLEK nor DSAEK may eventually survive’.2 Although this clearly has not happened as yet, with few surgeons switching from DSEK to DMEK,21 a better understanding of the technique is gradually improving.24 The purpose of this review is to objectively summarise the progress in DMEK, with regard to donor preparation, surgical techniques, postoperative management and clinical outcomes almost 10 years on.
Surgical techniques: donor preparation
Donor preparation for DMEK has gradually evolved from its initial description by Melles.8 The most common technique described was initially popularised as the ‘standard’ technique described in 2008,25 and then further modified to a ‘standard no touch technique’.26 In the original technique, a hockey stick is used to loosen the peripheral DM just centrally from the scleral spur over 180–360°. The DM is then stripped with a fine forceps—either 50%, then followed by a superficial trephination, then completing the DM stripping; or 100% DM stripping with full-thickness trephination using a contact lens underneath. The latter technique allows for the preservation of the underlying cornea stroma, which may be used for other procedures such as anterior lamellar keratoplasties.27
Since then, variants of this technique have been described in an attempt to improve DMEK graft harvesting success and outcomes (figure 2).28 There is also an impetus from eye banks to innovate new and reliable techniques to prepare DMEK donors with minimal EC damage and reduced wastage.27 Inventive techniques have been described, such as the use of hydrodissection with the donor on an anterior chamber maintainer with the endothelium side up;29 and variants of air-dissection similar to a ‘reverse big bubble’ technique.30 ,31 However, variability and failure to obtain a ‘big bubble’ remains an issue, with reports of up to 83% EC loss, and many donors with a significant layer of remaining stroma attached to the DM.32 More recently, a technique has been described using injection of organ culture storage medium to cleave the DM-stromal plane while the donor is still submerged.33 ,34 Essentially, donor corneas were submerged in tissue culture medium while a 25-gauge needle was inserted bevel up, beneath the trabecular meshwork into the stroma and injected with storage medium to create a liquid bubble, before the bubble is removed and the donor is trephined to size. The reported advantages include a larger diameter, more reliable cleavage with fewer attempts at injection and reduced EC loss.34 ,35
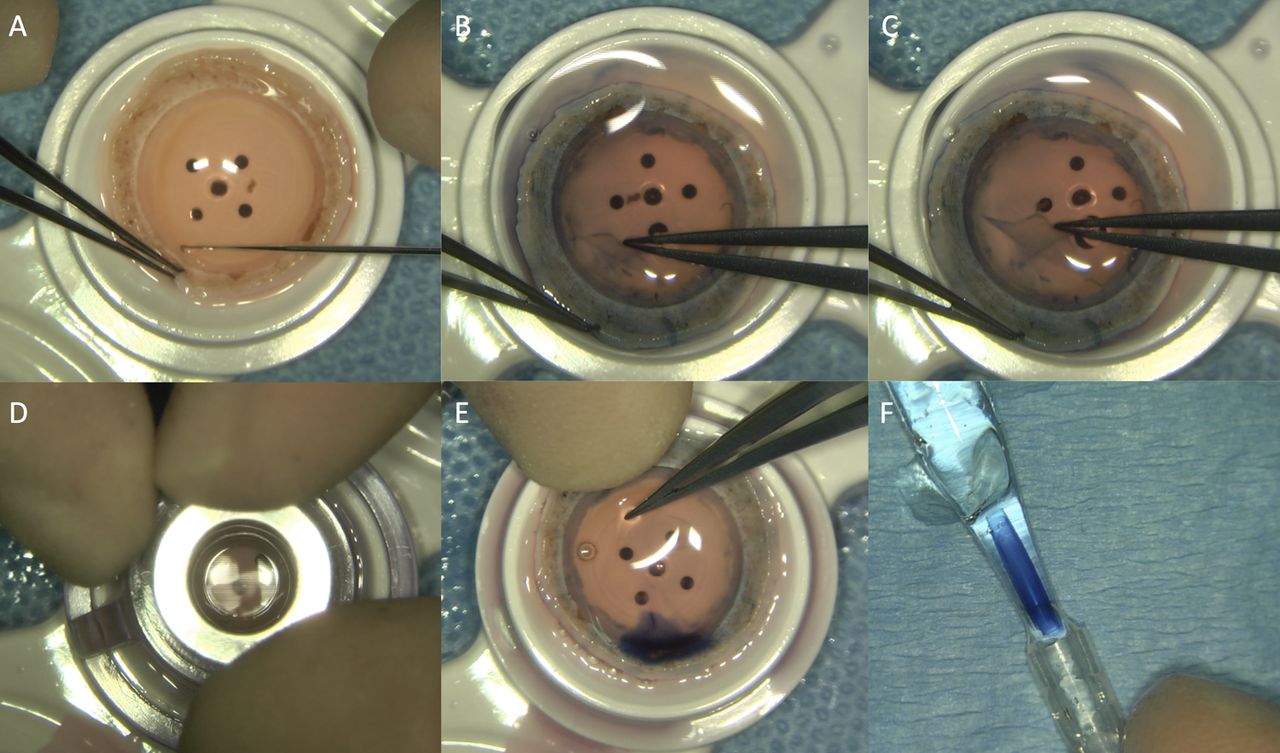
Descemet membrane endothelial keratoplasty donor preparation technique. (A) Scoring donor edge with Sinsky hook. (B) Stripping DM donor from edge. (C) Ensuring DM is stripped at least 50% with no tears. (D) Trephination of donor. (E) Remaining trephined donor stripped and stained with dye. (F) Donor inserted into glass injector.
Donor staining is important for visualisation of the graft edges and determination of graft orientation intraoperatively. While the use of trypan blue 0.06% is reported to be safe for corneal ECs in vitro (up to 0.4% concentrations immersed for 15 min),36 the safety of the concentrations and durations of staining used in vivo is relatively unknown.37 Newer dyes such as patent blue and methyl blue, approved for retinal membrane staining, may be safer in terms of corneal endothelial toxicity in vitro.36 Asymmetrical marking of the donor may also be useful for determining the graft orientation after insertion into the eye.38 More importantly, donor preparation may be influenced by donor characteristics. Some have advocated choosing older, non-diabetic donors as these are related to possible ease in graft preparation and handling. Donor tissue from younger donors (ie, <50 years of age) may tear easily due to stronger adherence to the stroma,39 and generally form tighter scrolls, thereby increasing unfolding times and EC loss.40 ,41 However, further studies are required to provide adequate evidence for this to influence eye bank and clinical practice in terms of donor choice and staining techniques.
Surgical techniques: donor insertion
While most publications have focused on DMEK donor preparation and insertion, adequate recipient eye preparation is probably just as important. An adequately sized descemetorrhexis may be important for graft attachment in order to reduced overlap between donor and recipient DM, which may cause donor lift-off in the periphery (unlike DSEK where the stripping diameter is often smaller than the donor).42 The use of trypan blue 0.06% staining in the recipient after stripping the DM can be useful to ensure complete DM removal as residual fragments of the anterior banded layer of the host DM have been associated with a higher risk of detachments.43 As it is believed to reduce graft adherence, avoidance of viscoelastics during the recipient preparation has been advocated, although some surgeons report the safe use of cohesive viscoelastics as long as it is thoroughly removed before donor insertion.44 ,45
One of the challenges of DMEK comes from the fact that the DM, once separated from stroma, has an innate tendency to form a tight scroll with the endothelium on the outside of the scroll (especially in younger donor tissue), and this is arguably still the most difficult step in DMEK surgery. Current techniques all involve injecting the DM through a wound, which now may be smaller than in DSEK. There have been a variety of instruments described for DMEK donor insertion: modified intraocular lens cartridge, modified semi-rigid tubing, implantable Collamer lens inserter and a cartridge, or a glass injector.46–48 All these techniques protect the DM scroll from the wound but may still be susceptible to endothelial damage caused by contact with the injector lumen (figure 3). However, no direct comparative studies have been conducted to compare outcomes using these inserters, at the time of this publication. Donor insertion, and, more importantly, unscrolling and manipulation of the donor scroll in the eye, remains a major barrier to many surgeons attempting to learn DMEK.24
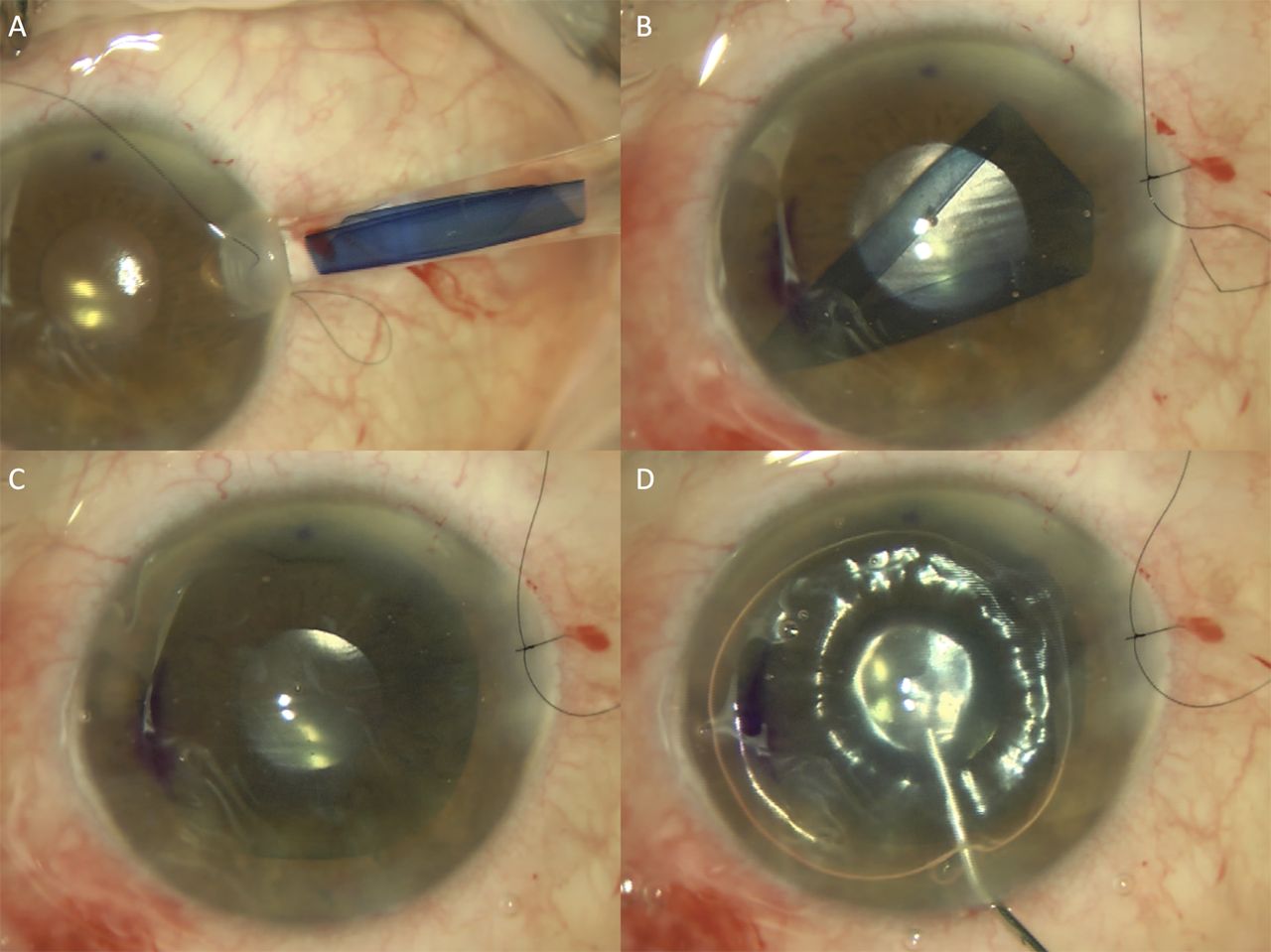
Descemet membrane endothelial keratoplasty donor insertion technique. (A) Insertion of donor via glass injector through temporal 3.2 mm clear corneal tunnel. (B) Double scroll formation with endothelium rolled upwards. (C) Donor unscrolled in shallow anterior chamber. (D) 20% SF6 gas combination with air injected under donor for full air fill with inferior peripheral iridectomy.
Confirming the correct graft orientation is a key step after donor insertion, with various techniques such as direct visualisation of a cannula between donor layers,7 ,44 use of a hand-held or microscope-mounted slit beam,49 illumination techniques,50 asymmetrical marking on the graft38 and even intraoperative optical coherence tomography (OCT) (figure 4).51

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intraoperative, spectral domain optical coherence tomography during Descemet membrane endothelial keratoplasty. (A) Imaging helps to demonstrate donor orientation after insertion. (B) Intraoperative donor graft adhesion within 1 min of full air fill at 30 mm Hg of pressure, with noticeable interface fluid still present. (C) Confirmation of improved intraoperative graft adhesion after 8 min, with reduction of interface fluid at the end of surgery with bandage contact lens on the cornea.52
Many different graft unfolding techniques have also been described, which essentially comprise a stepwise approach to unfolding a double scroll by tapping the cornea in a shallow anterior chamber, and the use of an air bubble to assist in tight or single scrolls.53 ,54 The efficiency of this step is important as it has been reported that the rate of graft detachments and EC loss increases significantly with a more difficult graft unfolding, probably related to greater endothelial trauma.55 The use of longer-acting gas (most commonly, non-expansile concentrations of SF6 gas with air, ie, 20% SF6) intraoperatively with a peripheral iridectomy has been described with no increased toxicity to corneal endothelium, but this has not been directly compared with the use of air in a randomised fashion to demonstrate that this actually improves graft adhesion.44 While most authors advocate ‘air-filling’ times of at least 1 h7 ,46 ,53 (presumably from past experiences with DSEK), a study using intraoperative OCT suggests that complete graft adhesion during DMEK is achieved around 5–6 min.51
Complications and postoperative management
Graft detachment versus re-bubble rates
Graft detachment is the most common complication after DMEK surgery. Initial reports of complete graft detachments were as high as 30%,4 while partial graft detachments were up to 62–63%.17 ,19 However, with improved techniques and surgical experience, reported graft detachments have reduced to 34.6% in a multicentre study,55 and as low as 4% in one case series.56 However, when evaluating DMEK complications one has to be aware that some authors choose to emphasise on re-bubble rates rather than detachment rates. For example, re-bubble rates were as high as 73.8% (presumed all graft detachments were re-bubbled) in one series,57 to as low as 3–6% (with a 15.8–50% partial detachment rate).58 ,59 This reflects the variation in DMEK surgeons’ preferences and beliefs: on the one hand, conservative surgeons may choose to observe graft detachments for months before any intervention41 ,60 while, on the other hand, surgeons may repeat air injections for all, if not most, of their graft detachments within 1–2 weeks.61 While late intervention allows the chance for the cornea to clear spontaneously, visual recovery is longer, while the delayed healing may lead to potential corneal scarring, poorer final visual outcome and lower EC count.62 However, there are currently no direct comparative studies to compare the outcomes of early versus late air injections after graft detachments following DMEK.
Graft rejection
The incidence of ‘classical’ allograft rejection after DMEK is widely reported to be ‘rare’, which is one of the purported advantages of DMEK. One series reported a 0.7% rejection episode rate after DMEK compared with historical control groups of DSEK (9%) and PK (17%). However, the comparative groups in this particular study were heterogeneous, with 12% pseudophakic bullous keratopathy in the DSEK group compared with 3% in the DMEK group.63 Moreover, another publication from the same centre and time frame reported a 5.1% rejection episode rate in 1 year, although that was attributed to difference in surgeons’ tapering corticosteroid regimes (all graft rejections were from one centre using a ‘earlier tapering regime’ of prednisolone acetate 1% every 2 h while awake for 2 weeks, four times daily for 1 month, three times daily for 1 month, twice daily for 1 month and once daily indefinitely; the authors advocated prednisolone acetate 1% four times daily for 4 months, three times daily for a month, twice daily for 1 month and once daily indefinitely).19 Nonetheless, graft rejection episodes following DMEK may well be under-reported and heavily dependent on postoperative monitoring and varying steroid regimes. Although only one centre reported graft rejection rates of <1%, most report graft rejection ranges of around 1.4–5%64 and a mean of 3.7% in a large multicentre multisurgeon series.56 Patients may present with symptoms such as eye redness, discomfort or reduction in visual acuity with characteristic Khodadoust lines with keratic precipitates, but some patients may be asymptomatic and detected on routine follow-up (30% were asymptomatic).65 In one large series, 7 of 500 eyes experienced immune allograft rejection, anytime from 4 to even 42 months after surgery.64 Interestingly, these patients developed characteristic EC changes a few months before the allograft rejection on routine specular microscopy, suggesting that there may be a role for routine endothelial imaging for the detection and prevention of allograft rejection in patients with DMEK.64 These studies suggest that allograft rejection in DMEK is probably not as rare as we think, with reports supporting a slow-onset immune response different to the clinical manifestations seen in DSEK and PK.64 Surgeons should continue to be vigilant for mild episodes of allograft rejection that can occur at anytime in the postoperative period, while more studies are needed to investigate the role of topical corticosteroid regime to prevent EC damage and improve DMEK graft survival.66
Minor postoperative complications
Most other postoperative complications reported by various studies have been relatively rare with only one multicentre, multisurgeon study with adequate numbers to represent the various uncommon complications.56 These included epithelial defects and/or erosion (3.0%), secondary glaucoma (2.8%) and significant Descemet graft folds (1.9%). The remaining complications were reported in <1% of cases, such as anterior synechiae, hypotony, pupillary block, subepithelial haze and interface pigment deposits. One study reported an unusually high rate of cystoid macular oedema, detected in up to 13.3% of eyes following DMEK with cataract extraction, and 12.5% of eyes following DMEK alone, within 6 months after surgery.67 Post-DMEK incidence of raised intraocular pressure can be as high as 12% (2.7% developing glaucoma), most of which was secondary to steroid response.68 As a result of improving techniques and reduced detachment rates, primary iatrogenic graft failure rates have also reduced from as high as 20% in initial series to as low as 2.2%.69
Outcomes: visual acuity and EC loss
Most studies have reported good visual recovery and final outcomes following DMEK.7 ,15–20 Within 6 months, 79–94% of eyes could achieve best (spectacle)-corrected visual acuity (BCVA) of at least 20/40, while 22–47% may attain BCVA of at least 20/20.16 ,20 Most studies have also reported that DMEK causes a mild hyperopic shift of <+0.50 D after 6–12 months' follow-up.17 ,70 However, it is important to note that early reports of visual outcomes in DMEK were performed in early cases of corneal decompensation from Fuchs dystrophy, with mild–moderate preoperative visual loss (median preoperative visual acuity 20/40–20/50).45 ,71 These eyes may possibly have less preoperative anterior stromal scarring or reversible stromal changes compared with chronic cases of bullous keratopathy with poor vision.72 Nonetheless, compared with DSEK in the fellow eye, patients reported significantly better visual acuity and preferred their vision in the DMEK eye in unmasked studies.15 ,18 ,73 ,74 Although some studies suggest that DSEK visual outcomes can be improved by using thinner donor tissue,75 ,76 randomised comparisons of DMEK and ultra-thin DSEK are needed.3 Though studies have reported a slower visual recovery after ultra-thin DSEK compared with DMEK, a comparable percentage of eyes achieve BCVA of 20/20 or better 1 year after surgery.76 As the results of ultra-thin DSEK improve, the purported benefits of DMEK may eventually be overshadowed by the ease and reliability of the widely performed DSEK.76
Endothelial cell loss following DMEK ranges widely, from 32% to 40% at 3 months, and 36% to 40% at 6 months.15 ,17 ,19 ,20 ,47 ,57 ,77 Longer term studies with a variable follow-up rate report EC loss of around 19–36% at 1 year.20 ,61 ,78 ,79 The longest term results report a median 5-year cell loss of 39% in DMEK (28 eyes), which compared favourably with prior reports of DSEK (53%) and PKP (70%) performed for similar indications.61 This study reported median EC loss of 27% at 12 months (548 eyes), 28% at 24 months (254 eyes), 31% at 36 months (98 eyes), 36% at 48 months (41 eyes) and 38% at 60 months (28 eyes).61 Another long-term study in 300 eyes reported EC loss of 35% at 6 months (254 eyes), 38% at 12 months (234 eyes), 43% at 24 months (130 eyes), 47% at 36 months (63 eyes), 52% at 48 months (25 eyes) and 55% at 60 months (9 eyes), which suggests a sharp decrease in the first six months, followed by a yearly decrease of approximately 7%.80 These reports of long-term EC loss in DMEK is encouraging compared with DSEK and PKP.13 The reported median EC loss in DSEK is high initially, but drops to an annual EC loss of 3–6% after the first year, which then ranges 44–46% at 3 years,81 ,82 and 51–54% at 5 years.82 ,83 In comparison, while the annual EC loss was gradual during the first decade after PKP of around 4–8% per year up to overall 70% EC loss at 5 years, there is minimal change in graft survival and EC loss from 5 to 10 years (Cornea Donor Study).81 ,84 These studies suggest that even though the initial EC loss was greater after DMEK and DSEK, the long-term rate of EC loss of DMEK may be lower compared with PKP. However, the two long-term studies on DMEK have a 96–97% loss to follow-up rate at 5 years, without reporting graft survival data, thereby underlining the need for more studies with long-term results to confirm the long-term efficacy of DMEK. In addition, most DMEK studies reporting on EC loss rates refer to the initial results of DSEK using the taco folding technique as a comparator, but today lower cell loss rates have been reported with improved donor insertion techniques.13 ,85–87
Conclusion
There is increasing evidence that DMEK has a role in improving outcomes for patients who require selective endothelial replacement. However, there are currently few adequately powered studies with sufficient long-term follow-up, with many publications reporting results from the same study cohorts by the same surgeons, many of whom pioneered and advocate this technique. Thus, more studies from other centres around the world are needed to confirm whether these results are replicable, and only time will tell whether DMEK in its current state is a procedure with the potential to be universally adopted by corneal surgeons in their routine clinical practice. Randomised studies comparing techniques (eg, ultra-thin DSEK vs DMEK) and trials comparing intraoperative techniques or postoperative management regimens are required to establish DMEK as the main EK technique of choice.
References
Footnotes
Contributors All authors met the ICJME criteria: (1) substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.