Article Text

Abstract
Aims To compare long-term clinical outcomes following small incision lenticule extraction (SMILE) and femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK) for myopia and myopic astigmatism correction.
Methods In this retrospective study, we enrolled a total of 101 patients (101 eyes) who underwent SMILE or FS-LASIK 3 years prior. Measured parameters included uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), manifest refraction and corneal wavefront aberrations.
Results No significant differences in patient characteristics were found between the two groups. At the 3-year follow-up, UDVA was better than or equal to 20/20 in 90% and 85% (p=0.540) of the eyes; the efficacy indexes were 1.05±0.19 and 1.01±0.21 in the SMILE and FS-LASIK groups, respectively (p=0.352). Safety indexes were 1.19±0.17 and 1.15±0.20 in the SMILE and FS-LASIK groups, respectively (p=0.307). Eighty per cent and 65% of eyes were within ±0.50 D of the attempted spherical equivalent correction after SMILE and FS-LASIK, respectively (p=0.164). Vector analysis revealed no significant differences in astigmatic correction between the two groups (p>0.05). Surgically induced spherical aberration was higher in the FS-LASIK group than in the SMILE group (p<0.001).
Conclusion Long-term follow-up analysis suggested that both SMILE and FS-LASIK were safe and equally effective for myopic and astigmatic correction.
- small incision lenticule extraction (SMILE)
- femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK)
- Myopia
- astigmatism
- Aberrations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- small incision lenticule extraction (SMILE)
- femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK)
- Myopia
- astigmatism
- Aberrations
The availability of femtosecond technique has helped to promote microkeratome-free refractive surgeries.1 Both femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK) and small incision lenticule extraction (SMILE) have become the preferred surgery of choice for an increasing number of surgeons who perform refractive surgeries.2–5
The advantages of SMILE, compared with FS-LASIK, include the requirement for a smaller incision and avoidance of flap-related complications. Moreover, although femtosecond technique plays a role in both SMILE and FS-LASIK, the key photoablation procedure is performed with ultraviolet light by an excimer laser in FS-LASIK; in SMILE, a femtosecond laser uses near-infrared light to photodisrupt stromal tissue. SMILE is associated with less keratocyte apoptosis, proliferation and inflammation in the early corneal wound healing period6 7; however, no significant differences in terms of short-term clinical outcomes have been reported.1 8–12 Thus, it remains to be determined whether different lasers and surgical procedures impact long-term clinical outcomes. In this study, we aimed to investigate 3-year clinical outcomes following SMILE and FS-LASIK for myopia and myopic astigmatism correction.
Subjects and methods
Subjects
In this retrospective study, we enrolled patients who underwent SMILE or FS-LASIK at the Refractive Surgery Center of the Department of Ophthalmology, Eye and ENT Hospital of Fudan University. Patients received a written invitation for an additional 3-year follow-up if they lived near Shanghai and exhibited 20/20 or better uncorrected distance visual acuity (UDVA) on the first day after the procedures. Preoperative inclusion criteria included age over 18 years, sphere up to −9.50 dioptres (D) with astigmatism up to −5.00 D, corrected distance visual acuity (CDVA) of 20/20 or better and stable refraction for 2 years. Patients with systemic diseases, a history of ocular surgery or trauma or a history of ocular disease other than myopia or astigmatism were excluded. This study followed the tenets of the Declaration of Helsinki. Informed consent was obtained from all participants. Data from the right eye of each patient were selected for statistics.
Procedures
The same surgeon (XZ) performed all surgical procedures. In the SMILE procedures, a 500 kHz VisuMax femtosecond laser system (Carl Zeiss Meditec, Jena, Germany) was used, with a pulse energy of 130 nJ. The lenticule diameter was set between 6.25 and 6.70 mm; the cap diameter was set to 7.5 mm at a 120 µm depth. A 90° single-side cut, with a length of 2 mm, was created during the procedure. In the FS-LASIK procedures, the same femtosecond laser system was used for flap creation, followed by a MEL 80 excimer laser (Carl Zeiss Meditec) for stromal ablation, with a pulse energy of 185 nJ. Flap diameter and thickness were 8.5 mm and 100 µm, respectively, with standard 90° hinges and 90° side cut angles. The planned optic zone was set between 6.25 and 6.70 mm. After FS-LASIK, a soft contact lens was worn, then removed at 1 day postoperatively. Topical levofloxacin, 0.1% fluorometholone solution and non-preserved artificial tears were used after both SMILE and FS-LASIK.
Measurements
UDVA, CDVA and manifest refraction were recorded. Corneal thickness and achieved optical zone were measured with Scheimpflug camera imaging (Pentacam HR, Type 70900, Wetzlar, Germany). Achieved optical zone was defined as the largest ring diameter when the difference between the mean ring power and the pupil centre power was ≤1.50 D, as reported previously.13
Astigmatism correction after SMILE and FS-LASIK was compared by using vector analysis. The following parameters were recorded: preoperative and postoperative astigmatism (as determined by manifest refraction), target-induced astigmatism (TIA) (astigmatic change the surgery was expected to induce), surgically induced astigmatism (SIA) (astigmatic change the surgery actually induced), difference vector (DV) (the vector difference of the residual astigmatism), correction index (CI) (the ratio of achieved correction to intended correction), magnitude of error (MofE) (algebraic difference of the residual astigmatism), angle of error (AofE) (algebraic difference of the axis of the residual astigmatism), index of success (IOS) (the proportion of the residual astigmatism, compared with TIA) and flattening index (FI) (the proportion of achieved correction at the intended axis).
Corneal wavefront aberrations were also measured with the Pentacam HR under scotopic light settings in the central 6 mm zone. Root-mean-square of higher order aberrations (HOAs) from the third to sixth order, spherical aberration and coma of the cornea were evaluated.
Data analysis
All statistical analysis was performed with the Statistical Package for Social Sciences (SPSS, V.20). The Kolmogorov-Smirnov test was used to test for normality. The Mann-Whitney U test was used to compare data between two groups. To compare proportions, Fisher’s exact test was used. For all tests, p<0.05 was considered statistically significant.
Results
Patient characteristics are presented in table 1. No significant differences in patient characteristics were found between the two groups (all p>0.05). No postoperative complications, such as cornea ectasia and infection, were observed in any patient.
Characteristics of the SMILE and FS-LASIK groups
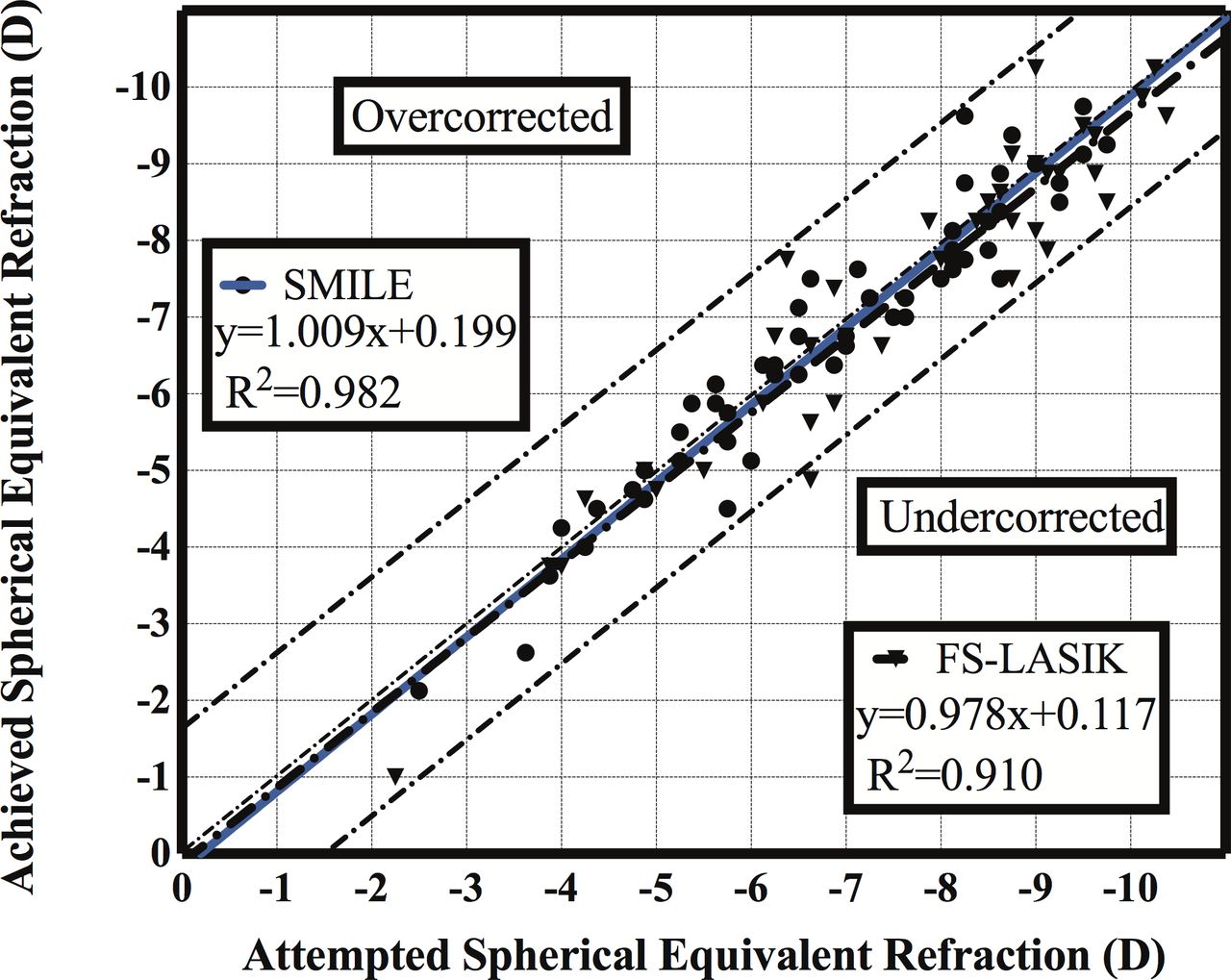
Clinical outcomes at 3 years are summarised in table 2. At the 3-year follow-up, in the SMILE group, UDVA was better than or equal to 20/20 and 20/16 in 90% and 63% of eyes, respectively; in the FS-LASIK group, the corresponding proportions were 85% (p=0.540, compared with SMILE) and 44% (p=0.012), respectively. The efficacy indexes were 1.05±0.19 and 1.01±0.21 after SMILE and FS-LASIK, respectively (p=0.352). Two per cent of eyes lost one Snellen line and 65% of eyes showed an increase of 1–2 lines in the SMILE group; in the FS-LASIK group, the corresponding proportions were 12% (p=0.039) and 56% (p=0.409), respectively. The safety index was 1.19±0.17 in the SMILE group and 1.15±0.21 in the FS-LASIK group (p=0.307). Scatterplots of achieved versus attempted spherical equivalent are shown in figure 1. Eighty per cent and 65% of eyes were within ±0.50 D of the attempted spherical equivalent correction after SMILE and FS-LASIK, respectively (p=0.164).

A scatterplot of attempted versus achieved manifest refraction spherical equivalent correction at 3 years after SMILE and FS-LASIK. FS-LASIK, femtosecond laser-assisted laser in situ keratomileusis; SMILE, small incision lenticule extraction.
Comparisons of refractive outcomes between the SMILE and FS-LASIK groups
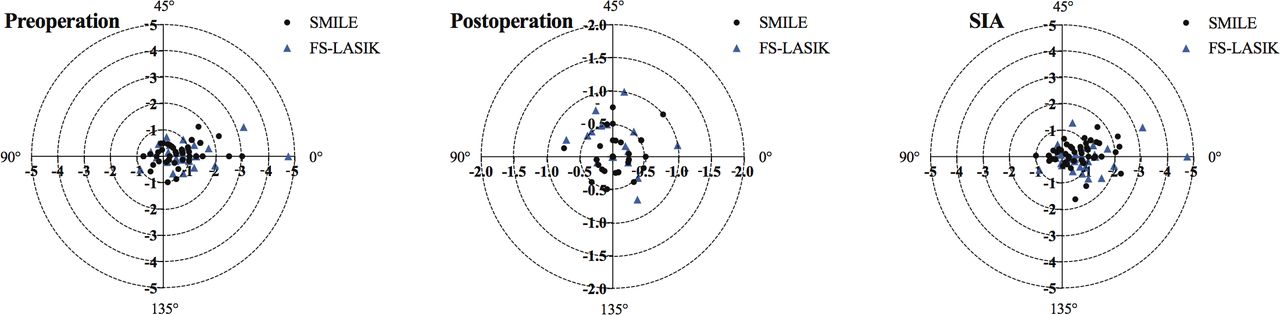
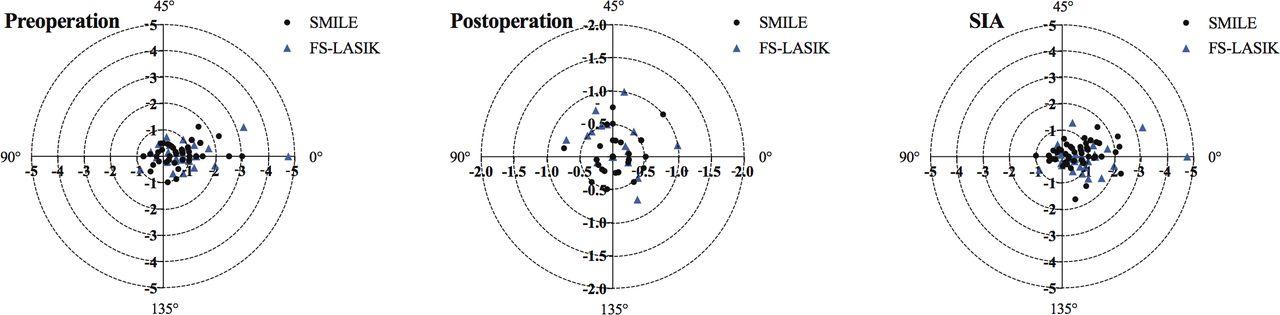
There were no significant differences in TIA, SIA, DV, CI, MofE, AofE, IOS or FI between the two groups (all p>0.05) (table 2). Double-angle plots depicting the preoperative and postoperative astigmatism and SIA of eyes are shown in figure 2.
{kind=link}
{kind=link}
Double-angle plots depicting preoperative and postoperative astigmatism and surgically induced astigmatism (SIA) of eyes after SMILE and FS-LASIK. FS-LASIK, femtosecond laser-assisted laser in situ keratomileusis; SMILE, small incision lenticule extraction.
Table 3 shows the aberration outcomes. Postoperative and induced spherical aberrations were higher in the FS-LASIK group than in the SMILE group (both p<0.001). There were significant differences in postoperative HOAs, spherical aberration and coma in the SMILE (p<0.001, p<0.001 and p=0.020, respectively) and FS-LASIK groups (p<0.001, p<0.001 and p=0.007, respectively), compared with preoperative values. Achieved optical zone was larger in the SMILE group (5.48±0.68) than in the FS-LASIK group (5.19±0.57) (p=0.045).
Comparisons of corneal aberrations between the SMILE and FS-LASIK groups
Discussion
SMILE and FS-LASIK are popular refractive surgeries, and each has its own characteristics. Long-term observation of outcomes following these two surgeries, which use different lasers and follow different surgical procedures, may help facilitate the future development and application of refractive surgeries.
In previous studies comparing short-term outcomes following SMILE and FS-LASIK, no significant differences were reported in refractive outcomes.1 8–12 In this study, we found no significant differences in long-term outcomes. In this study, UDVA was better than or equal to 20/20 and 20/16 in 90% and 63% of eyes in the SMILE group at the 3-year follow-up visit; the corresponding proportions were 85% (p=0.540, compared with SMILE) and 44% (p=0.012), respectively, in the FS-LASIK group. The efficacy indexes were 1.05±0.19 and 1.01±0.21 after SMILE and FS-LASIK, respectively (p=0.352). The efficacy index observed at the 3-year follow-up visit was similar to that observed at the 4-year follow-up in the SMILE group (1.07±0.16).14 Pedersen et al15 demonstrated that 72% of high-myopic eyes had a UDVA of 20/20 or better, 3 years after undergoing SMILE. Kobashi et al16 found that, at 2 years postsurgery, 100% of eyes in the SMILE group and 93% of eyes in the wavefront-guided LASIK group had a UDVA of 20/20 or better. Regarding safety, in the present study, the safety index was 1.19±0.17 in the SMILE group and 1.15±0.21 in the FS-LASIK group (p=0.307). The safety index at the 5-year follow-up visit for the first 91 eyes that received SMILE worldwide was 1.2.17 In the present study, 80% and 65% of eyes were within ±0.50 D of the attempted spherical equivalent correction after SMILE and FS-LASIK, respectively (p=0.164). These numbers were 100% and 93%, respectively, in the study by Kobashi et al.16 Although SMILE induces a lower rate of keratocyte apoptosis, proliferation and inflammation, compared with FS-LASIK,6 7 the 3-year refractive outcomes observed following these two surgeries are almost equivalent. Based on the results at the 3-year follow-up, it can be inferred that both SMILE and FS-LASIK are effective, predictable and safe procedures.
Vector analysis revealed no differences between the two groups, in terms of astigmatic correction. A previous prospective study demonstrated that SMILE offered less favourable astigmatic correction, compared with FS-LASIK.18 However, this difference might be because the surgeons involved were proficient with LASIK but not with the SMILE procedure; this might have affected both centration and astigmatic correction. In contrast, in the present study, the surgeon had been performing SMILE procedures for >1 year. The outcomes observed in the present study, which are similar to those observed in another study,19 show that both procedures yielded acceptable outcomes, with respect to astigmatism correction.
In this study, SMILE exhibited significant reductions in induced spherical aberration, compared with FS-LASIK. Similar outcomes have been reported previously.8 20 21 A possible reason for this finding may be a larger achieved optical zone after SMILE, compared with FS-LASIK, for a similar planned optical zone22; importantly, postoperative spherical aberration is related to optical zones. There was no difference in the incidence of induced coma between SMILE and FS-LASIK groups. Because induced coma might be associated with decentration, the centration of the treatment zone in patient-controlled fixation during SMILE may be similar to active eye tracker-assisted FS-LASIK.23
A limitation of this study is the presence of selection bias. Patients with visual complaints may be more inclined to agree to undergo additional 3-year follow-up examinations. Thus, it would be better to investigate the stability if some patients had not lost their follow-up visit data.
In conclusion, long-term outcomes of both SMILE and FS-LASIK demonstrate that these procedures are safe and equally effective for myopic and astigmatic correction.
Ethics approval
This study was approved by the ethics committee of the Eye and ENT Hospital of Fudan University.
References
Footnotes
TH and YX are joint first authors.
TH and YX contributed equally.
Contributors Concept and design: TH, YX and XZ. Data collection and analysis: TH, YX, XH, JS, LZ and XC. Writing the article: TH and YX. Critical revision of the article: XH, JS, LZ, XC and XZ. Final approval of the article: all authors.
Funding Supported in part by the National Natural Science Foundation of China for Young Scholars (Grant No. 81600762 and 81500753), the National Natural Science Foundation of China (Grant Nos. 81570879 and 81770955) and the Project of Shanghai Science and Technology (Grant Nos. 17411950200 and 17411950201).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Available on request from the author TH.
Linked Articles
- At a glance