Article Text

Abstract
Purpose To assess the prevalence and severity of preoperative and postoperative astigmatism in patients with cataract in the UK.
Setting Data from 8 UK National Health Service ophthalmology clinics using MediSoft electronic medical records (EMRs).
Design Retrospective cohort study.
Methods Eyes from patients aged ≥65 years undergoing cataract surgery were analysed. For all eyes, preoperative (corneal) astigmatism was evaluated using the most recent keratometry measure within 2 years prior to surgery. For eyes receiving standard monofocal intraocular lens (IOLs), postoperative refractive astigmatism was evaluated using the most recent refraction measure within 2–12 months postsurgery. A power vector analysis compared changes in the astigmatic 2-dimensional vector (J0, J45) before and after surgery, for the subgroup of eyes with both preoperative and postoperative astigmatism measurements. Visual acuity was also assessed preoperatively and postoperatively.
Results Eligible eyes included in the analysis were 110 468. Of these, 78% (n=85 650) had preoperative (corneal) astigmatism ≥0.5 dioptres (D), 42% (n=46 003) ≥1.0 D, 21% (n=22 899) ≥1.5 D and 11% (n=11 651) ≥2.0 D. After surgery, the refraction cylinder was available for 39 744 (36%) eyes receiving standard monofocal IOLs, of which 90% (n=35 907) had postoperative astigmatism ≥0.5 D and 58% (n=22 886) ≥1.0 D. Visual acuity tended to worsen postoperatively with increased astigmatism (ρ=−0.44, P<0.01).
Conclusions There is a significant burden of preoperative astigmatism in the UK cataract population. The available refraction data indicate that this burden is not reduced after surgery with implantation of standard monofocal IOLs. Measures should be taken to improve visual outcomes of patients with astigmatic cataract by simultaneously correcting astigmatism during cataract surgery.
- angle
- epidemiology
- treatment other
- vision
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cataract extraction is the most commonly performed surgery overall by the National Health Service (NHS). Approximately 350 000 operations are performed per year on patients with a mean age of 77 years1. Approximately 30% of persons in the UK aged 65 years and over have visually impairing cataracts in one or both eyes.2
There is an increasing patient demand to minimise postoperative refractive error during cataract surgery.3 Residual astigmatism after cataract surgery may result in reduced unaided distance visual acuity (VA), which in turn may hinder satisfactory postoperative refractive results. Spectacle independence for distance activities is unlikely unless patients achieve ≤0.50 dioptres (D) of astigmatism after surgery4 and the OR of needing spectacles has been found to increase significantly with each dioptre of astigmatism.5
Currently, epidemiological evidence on the prevalence and severity of astigmatism prior to cataract surgery is mostly sourced from single-site, prospective or cross-sectional studies.6–10 In addition, there is very little epidemiological evidence on the prevalence and severity of residual astigmatism following cataract surgery.11
Large, longitudinal real world studies describing astigmatic patients undergoing cataract surgery are needed to inform the potential requirement of simultaneous correction of astigmatism during surgery. The principle aim of the present study was to address this knowledge gap by determining the prevalence and severity of preoperative and postoperative astigmatism in a large, real world population of eyes with cataract in the UK. An exploratory objective was to describe the effect of postoperative residual astigmatism on patients’ VA.
Methods
Data source
This retrospective cohort study used data collected using the MediSoft Ophthalmology electronic medical record (EMR) system, a longitudinal data source collecting ophthalmic care episodes (including any ophthalmology visits and surgeries) and diagnostic information for over 1 million patients and over 150 ophthalmology clinics across the UK.12
A total of eight cataract clinics was selected based on the number of cataract surgeries (proxy for final cohort sizes), time of EMR adoption (estimate of historical data available), geography (to ensure representativeness) and visual assessment recording (to ensure consistency of outcome reporting). All patient data extracted, processed and analysed for this study were fully anonymised and compliant with the UK NHS rules governing use of patient-level healthcare data (as defined in the Data Protection Act of 1998). Anonymised database analyses of this type do not require ethical permission as they are viewed as audit or service evaluation.13 This study was approved by the participating NHS centre’s Caldicott Guardian.
Study population
All the analyses were performed at the eye level. Data were extracted for eyes with a first record of phacoemulsification of the lens and implantation of a prosthetic intraocular lens (IOL) (cataract surgery) between 1 January 2005 and 1 January 2015. Eyes were followed from the date of cataract surgery for up to 12 months and were required to have a valid record of preoperative keratometry cylinder (taken from biometry), used for estimating the magnitude of corneal astigmatism (dioptres). In attempts to exclude secondary types of non-age-related cataracts, eyes from patients aged less than 65 years on the date of first cataract surgery were not included in the analyses. In addition, eyes were excluded if they had any co-surgeries performed at the time of cataract surgery or repeat surgeries following cataract surgery (cases where intraoperative surgical adjuncts such as use of iris hooks, opposite clear corneal incisions (OCCI), capsular tension ring and performing limbal relaxing incisions (LRIs) were included). Finally, as only a small number of eyes (N=92, 0.1% of total eyes) were implanted with toric IOLs, these were included in the population description but excluded from postoperative analyses. No imputation of data was performed.
Corneal and refractive astigmatism measures
Preoperative astigmatism was described using keratometry (corneal astigmatism). The most recent cylinder measures within the 2 years prior to cataract surgery were used.
Astigmatism is with-the-rule (WTR) when the corneal curvature is steepest in the vertical meridian; conversely, astigmatism is against-the-rule (ATR) when the steepest corneal meridian is horizontal.14 In this study, using the positive cylinder, corneal astigmatism was defined as WTR when the steepest meridian was 90°±30° and ATR when it was between 1° and 30° or 150° and 180°, inclusive; all the rest (ie, steepest meridian >30° and <60°, or >120° and <150°) were considered as oblique astigmatism.15 Incision axis was available in degrees within the EMR. When the steepest meridian for astigmatism was not recorded, the astigmatism type was defined as unknown. Corneal topography was not available and thus regularity of astigmatism was not included in the study.
While keratometry is a required assessment prior to cataract surgery, refraction is used more frequently to measure astigmatism following surgery. In this retrospective study, auto refraction and subjective refraction records were used to describe postoperative astigmatism in eyes with the most recent refractive measure recorded between 2 months and 12 months inclusive after cataract surgery. This was to ensure that stable refraction measures following cataract surgery were evaluated. The results were stratified by presence of co-pathologies and by surgery performed on the steepest meridian (defined as the main corneal incision axis falling within ±15° from the corneal astigmatism steepest meridian). All other surgeries were considered 'off the steepest meridian’.
In order to describe levels of astigmatism severity, the distribution of astigmatism across increments of 0.5 D was reported both presurgery and postsurgery. Clinically relevant thresholds were set at 0.5 D, which was considered the minimal clinically relevant astigmatism, and at 1.0 D and 2.0 D, which have been previously used as thresholds for co-correction of astigmatism during cataract surgery.4 8
Power vector analysis
For the prevalence analysis, astigmatism was defined as cylinder ≥0.5 D. A power vector analysis was performed to evaluate how this pre-existing astigmatism changed following cataract surgery with implantation of standard monofocal IOLs. To describe this change, the corneal and refractive astigmatism of eyes with ≥0.5 D preoperative astigmatism were converted from cylinder into vector notations. Eyes which did not have both corneal and refractive axis and cylinder recorded prior to and following cataract surgery were not included in this analysis.
A power vector is the geometrical representation of spherocylindrical refractive errors in three dioptric components: spherical lens with power M, cylinder power J0 and cross-cylinder power J45, which are mathematically independent of each other.16 17 For the purpose of this study, we looked at changes in the astigmatic component of the power vector, that is the two-dimensional vector (J0, J45), defined as in Thibos et al (2001). This vector has been used in previously published studies to describe age-related trends in refractive and corneal astigmatism,17 18 to evaluate changes in astigmatism caused by refractive surgery16 or cataract surgery with implantation of toric IOLs,19 and to associate spectacle dependence to residual, postoperative astigmatism.5
J0 refers to cylinder power set at 90° and 180° meridians and is positive when astigmatism is WTR and negative when it is ATR; J45 refers to a cross-cylinder set at 45° and 135°, representing oblique astigmatism, and is positive when the axis of the negative cylinder is closer to 45° and negative when it is closer to 135°.17 18
When using power vector analysis, multivariate statistics can be applied to compare population means and variances of directional measures such as astigmatism.16 In this study, the preoperative and postoperative J0, J45 vector values were compared using the unadjusted paired Hotelling’s T2 test. A multivariate linear regression analysis was also performed to adjust for potential confounders such as the steepest meridian of surgery and presence/absence of any co-pathology.
Postoperative VA
VA was determined in terms of uncorrected distance visual acuity (UDVA) and best-measured distant visual acuity (BDVA), defined as the best measure out of corrected distance VA, UDVA and pinhole VA.20 Only the most recent UDVA and BDVA measures between 2 months and 12 months following cataract surgery were used to ensure vision stability. Postoperative UDVA and BDVA were expressed in logMAR Scale and were also converted to the Snellen Scale for presentation purposes. The results were stratified by presence/absence of any co-pathology and by the steepest meridian of surgery.
Effect of residual astigmatism on postoperative VA
In order to describe the effect of postoperative residual astigmatism on postoperative UDVA, the correlation between UDVA and refractive astigmatism was analysed using Spearman’s correlation coefficient (ρ) with significance set at P<0.05. Astigmatic eyes with preoperative astigmatism ≥0.5 D and with postoperative refraction and UDVA measurements recorded within 2 months and 12 months after surgery, were analysed. A sensitivity analysis was performed in a population of eyes without co-pathologies and intraoperative or postoperative complications and with postoperative spherical equivalent ±0.25 D and ±1.00 D to exclude potential external factors (other than astigmatism) that may impact VA.
Postoperative UDVA at different levels of astigmatism severity was also explored and presented using a box plot. Astigmatism severity was defined according to Lyall et al (2014),3 as follows: mild when cylinder is <1.5 D, moderate when the cylinder is between 1.5 D and <2.5 D and severe when it is between 2.5 D and <5.5 D. Eyes with ≥5.5 D were considered as potentially pathological corneas.
Statistical software
All analyses were performed using SAS software V.9.4.
Results
Population attrition and baseline characteristics
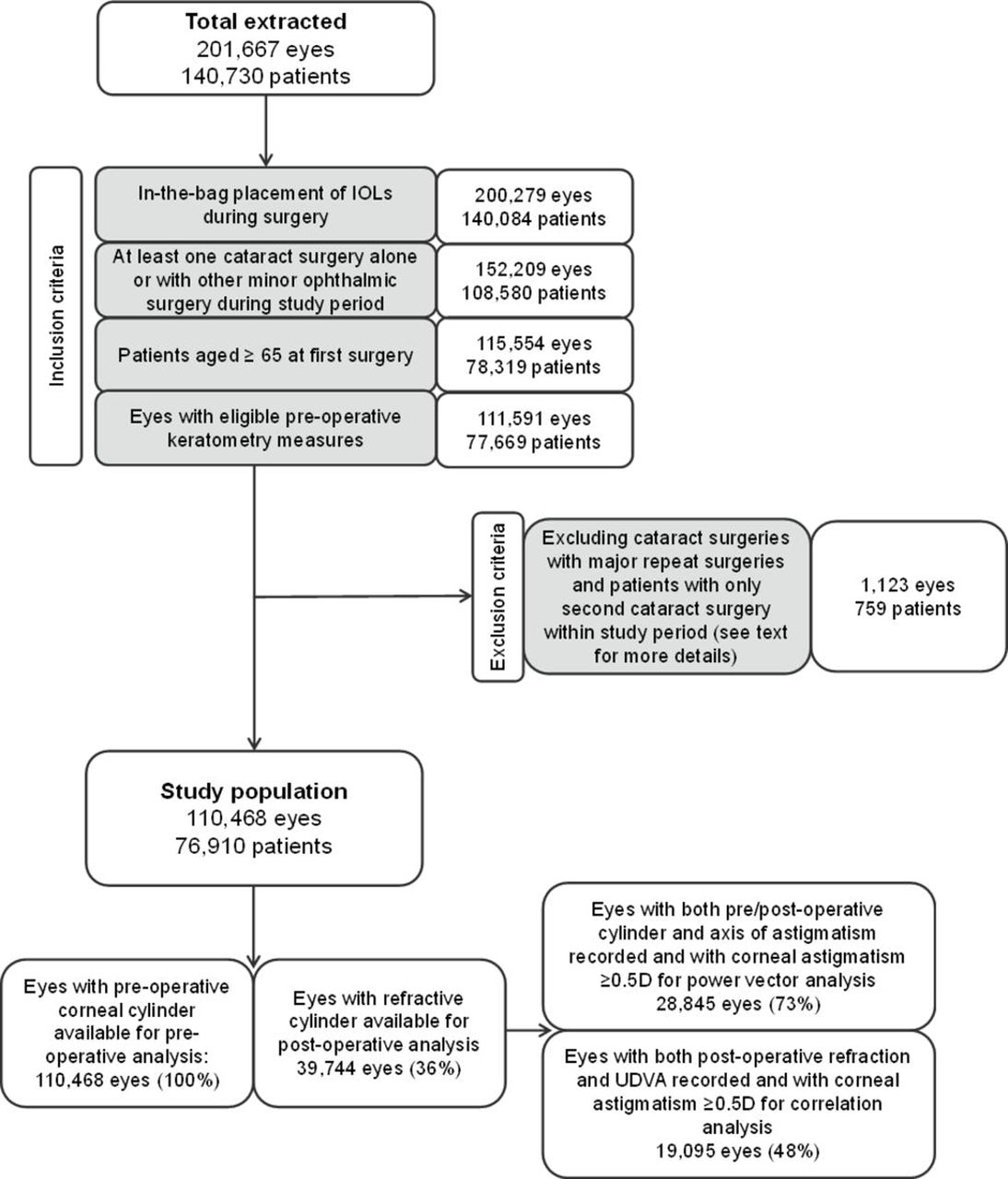
After applying the selection criteria, 110 468 eyes from 76 910 patients were identified (figure 1). A total of 43 352 patients (56%) had one eye operated and 33 558 (44%) had two eyes operated within the study period.

Population selection and attrition for eyes included in the study population. IOL, intraocular lens; UDVA, uncorrected distance visual acuity.
The study population had a mean (±SD) age of 79 (±7) years and the majority of the included eyes (N=70 094, 63%) did not have ocular co-pathologies (table 1). A small proportion of the included eyes recorded intraoperative (N=2608, 2.4%) or postoperative (N=3642, 3.3%) complications during the 12 months follow-up.
Baseline characteristics for the 110 468 study eyes
Representativeness of the selected population
The median age and gender distribution in our study population was compared with those reported in the National Ophthalmology Database (NOD) Audit 2016 Annual Report (using data from 34 NHS cataract surgical centres across the UK) to determine any potential selection biases. Patients in the NOD Audit (aged ≥18 years, N=43 606) recorded their first cataract surgery at a median age of 77 years. Similarly, in this study, median age was 77 years before applying the age limit of 65 years. From these patients, only those aged at least 65 years were included in the analyses to ensure the population comprised only age-related cataract surgeries rather than secondary cataracts, which may have an impact on the astigmatism levels. Patients aged 65 years and over accounted for 96% (N=1 35 101) of the extracted population. The gender distribution in this study was also similar to the NOD audit: 57% (N=35 396) of the NOD cataract population was female, compared with 60% (N=46 019) of our study population.1
Preoperative and postoperative astigmatism
Preoperative keratometry was described for all 110 468 eyes. Presurgery, the average corneal cylinder power was 1.06 D at a steepest meridian that in most eyes (N=46 999, 43%) was oriented ATR, in 31% eyes (N=33 878) was WTR and in 17% eyes (N=18 826) was oblique. In 10 765 eyes (10%) the steepest meridian was unknown (table 2).
Corneal astigmatism cylinder for the 110 468 eyes, according to astigmatism type
Overall, 78% (N=85 650) of the study eyes presented at the NHS clinics for cataract surgery with preoperative corneal astigmatism ≥0.5 D; 42% (N=46 003) had ≥1.0 D and 11% (N=11 651) had ≥2.0 D (figure 2, solid line). Figure 3A shows the distribution of astigmatism levels across the different astigmatism types. There was a lower proportion of eyes with corneal astigmatism ≥0.5D, ≥1.0 D and ≥2.0 D in the group of eyes with oblique astigmatism (66%, N=12 369; 25%, N=4695; 5%, N=882, respectively) compared with those with ATR (81%, N=38 069; 48%, N=22 438; 13%, N=5916) and WTR (79%, N=26 767; 42%, N=14 291; 11%, N=3678) astigmatism. However, the proportion of eyes with oblique astigmatism was smaller than those with WTR and ATR.

Distribution of preoperative (corneal) (solid line) and postoperative (refractive) astigmatism (dashed line). The preoperative population includes all eligible eyes (N=110 468), while the postoperative population contains all eyes with monofocal intraocular lens (IOLs) and an eligible refractive measurement (N=39 744).

Distribution of preoperative (corneal) astigmatism according to type (A) and the distribution of postoperative (refractive) astigmatism according to co-pathology (B). The preoperative population includes all eligible eyes (N=1 10 468), while the postoperative population contains all eyes with monofocal intraocular lens (IOLs) and an eligible refractive cylinder value (N=39 744). Proportions reflect cases exceeding a certain level of preoperative and postoperative astigmatism.
On the day of cataract surgery, over 99% of eyes (N=1 10 338) were implanted with monofocal IOLs and the majority (74%, N=81 731) of the surgeries were performed off the steepest meridian. Very few eyes had a record of astigmatism-correction procedures performed during surgery: 92 (0.1%) had a toric lens implanted (excluded from further analyses), 267 (0.24%) eyes received LRI and 196 (0.18%) received OCCI.
Measurements of postoperative (refractive) astigmatism were available for a total of 39 744 eyes, accounting for 36% of the study eyes that received monofocal IOLs (figure 1). Of these eyes, 90% (N=35 907) had ≥0.5 D, 58% (N=22 886) had ≥1.0 D and 16% (N=6477) had ≥2.0 D of refractive astigmatism after surgery (figure 2, dashed line). For eyes with or without a history of co-pathologies, the distribution of astigmatism was similar (figure 3B).
Comparison of preoperative and postoperative astigmatism
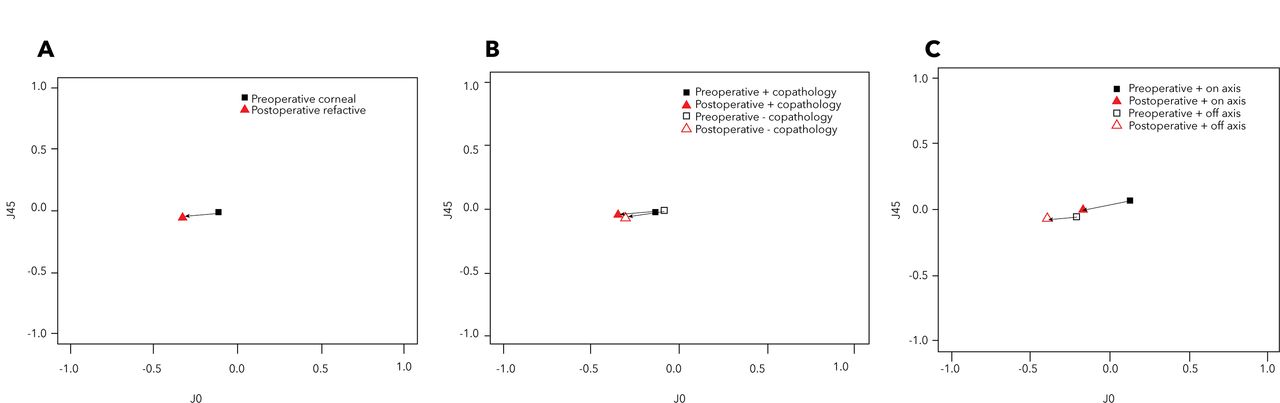
In order to describe the change in pre-existing astigmatism (≥0.5 D) after cataract surgery with implantation of standard monofocal IOLs, preoperative keratometry measures and postoperative (refractive) measures were converted into the two-dimensional preoperative and postoperative vector (J0, J45). A total of 28 845 eyes were eligible to be included in the analysis (figure 1). In order to visualise the change in astigmatism before and after surgery, figure 4A–C shows the presurgery and postsurgery mean vector values. While the mean J45 value remained near zero both presurgery and postsurgery (−0.016±0.38 D and −0.052±0.40 D, respectively) (figure 4A), the mean J0 value became more negative postsurgery (−0.107±0.63 D vs −0.326±0.57 D, respectively). In the graphs in figure 4, the origin represents an eye free of astigmatism.16 19 Therefore, if the astigmatism is improved after surgery we would expect to see a shift towards the origin. In this study we observed the opposite, suggesting that astigmatism may have worsened postsurgery. The difference between preoperative and postoperative vector values was statistically significant (figure 4A) and was not significantly affected by the presence or absence of co-pathologies (figure 4B). However, the change was significantly associated with the steepest meridian of surgery: the vector (J0, J45) of eyes operated off the steepest meridian was significantly more negative after surgery, than the vector of those operated on the steepest meridian (figure 4C).

Power vectors for all eyes implanted with monofocal intraocular lens (IOL) with both refractive cylinder and steepest meridian recorded 2–12 months postsurgery and preoperative astigmatism ≥0.5 D (n=28 845) for (A) all eyes, (B) eyes with and without co-pathologies and (C) eyes operated with and off the steepest meridian. Each point indicates the mean vector value. The arrow indicates the direction of change between presurgery and postsurgery (and not the magnitude). The P values represent the result of Hotelling’s T2 test (A) and the multivariate linear regression adjusted for presence of co-pathologies (B) and steepest meridian of surgery (C).
Effect of postoperative residual astigmatism on VA
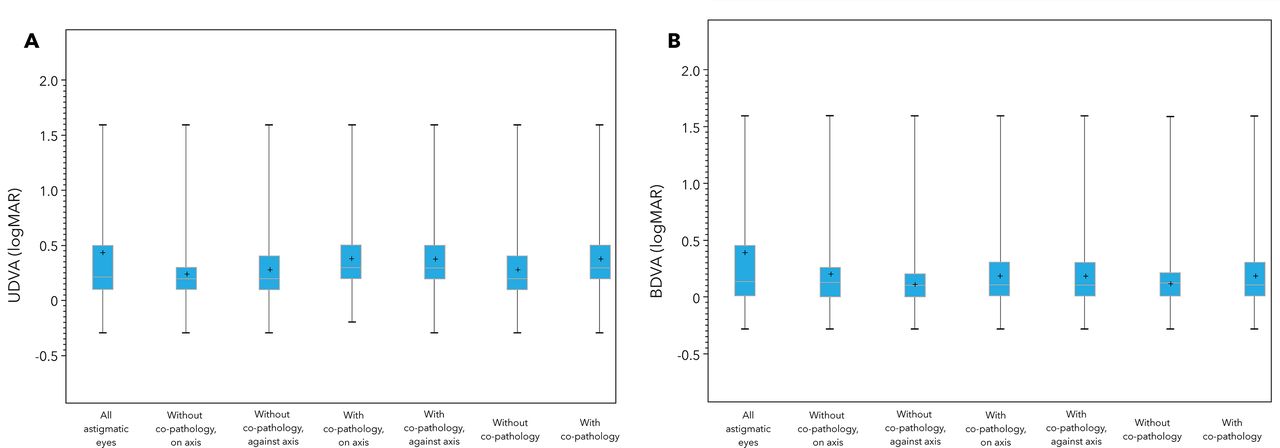
Postoperative BDVA and UDVA measures were available for 65% (N=55 268) and 39% (N=33 219) of the eyes implanted with monofocal IOLs and with preoperative corneal astigmatism ≥0.5 D. The average of LogMAR BDVA and UDVA was poorer for eyes with co-pathologies than for those without co-pathologies (table 3; figure 5A,B). Overall, VA was 20/25 (≤0.10 logMAR) or better in only 26% (UDVA, N=8600) and 51% (BDVA, N=28 204) of eyes. UDVA was compared between eyes with and without refraction measures with no difference seen (0.29 vs 0.26 (logMAR)).
Proportion of eyes with UDVA/BDVA ≤0.10 (logMAR)

Box plot of UDVA (A) and BDVA (B) scores according to surgery axis and presence of co-pathologies. Note that eyes with preoperative corneal astigmatism <0.5 D were excluded.
For 19 095 eyes, both UDVA and refractive astigmatism measures were available postsurgery and were included in the correlation analysis (figure 1). The higher postoperative residual astigmatism was moderately (ρ=−0.44) but significantly correlated with poorer UDVA (P<0.01), suggesting that VA significantly worsens as the severity of astigmatism increases. Figure 6 shows UDVA levels at different categories of astigmatism severity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Uncorrected distance visual acuity (UDVA) levels at different categories of astigmatism severity for eyes with refraction and UDVA measured after surgery (N=19 095). Mild astigmatism:<1.5 D, moderate: 1.5 -<2.5 D and severe: 2.5 -<5.5 D.3 Eyes with ≥5.5 D were considered as potentially pathological corneas.
The correlation strengthened, as expected, after excluding eyes with co-pathologies and complications, and limiting to those with postoperative spherical equivalent ±0.25 D (N=4848, ρ=−0.56, P<0.01) or ±1.00 D (N=10 992, ρ=−0.49, P<0.01).
Discussion
In this large, multicentre, retrospective analysis, we described the prevalence and severity of astigmatism both prior to and following age-related cataract surgery in a large population of eyes derived from eight NHS ophthalmology clinics across the UK. The results indicated that the large majority of the eyes (78%) present at cataract surgery with at least minimal clinically relevant astigmatism of 0.5 D and a substantial proportion of eyes have more severe astigmatism of at least 1.0 D (42%) and 2.0 D (11%). The most common type of astigmatism in the study population aged ≥65 years was ATR, which is in line with studies showing that astigmatism tends towards ATR as age increases.17 21
The distribution of preoperative astigmatism in the large population reported in this study confirms evidence from previous smaller studies, both in the UK and worldwide. Similar to this study, corneal astigmatism of ≥0.5 D was 75% in Wales6 (N=1231 eyes). Astigmatism ≥1.0 D was found in 36% of eyes with cataract in Germany7 (N=15 448 eyes), 47% in China22 (N=12 449) and 35% in South Korea9 (N=2847 eyes). Recently, Curragh et al reported that 41% of eyes undergoing cataract surgery (N=2080) in Northern Ireland had >1.0 D of corneal astigmatism.10
A variety of treatment options exist for reducing corneal astigmatism at the time of cataract surgery, including LRI or OCCI,4 toric lens implantation23 or a combination of each,4 and now also femtosecond laser astigmatic keratotomies.24
In the present study, astigmatism corrective co-procedures such as LRI, OCCI or implantation of toric IOLs were infrequently performed (0.6% of cases overall). This finding is in line with the data from the NOD audit (0.6%).1 Although we cannot exclude potential under-reporting of this information by surgeons, these data seem to indicate that astigmatism correction is rarely combined with routine cataract surgery in clinical practice in the UK. We anticipate reasons are multifactorial and include predictability concerns and limited previous experience, possible additional patient consent requirements and potential side effects (eg, higher postoperative discomfort, infectious keratitis).25
Where postoperative refraction measures were available, our study demonstrated that postoperative (refractive) astigmatism of ≥0.5 D and ≥1.0 D were prevalent in the 90% and 60% of the study population implanted with standard monofocal IOLs, with or without corrective co-surgeries such as LRI or OCCI. For these eyes with available VA measurements, we also found UDVA worsens as residual astigmatism increases. A similar correlation was observed in previous studies26 27 and suggests that if left uncorrected, astigmatism can significantly affect patients’ visual outcomes limiting their quality of life and well-being.23 26 Furthermore, our results suggest that astigmatism may worsen (at least in some eyes) following surgery based on shifts away from the origin in power vector analysis.16 19
To our knowledge, this is the first report of the postoperative astigmatism distribution in a large, real world cohort of eyes undergoing cataract surgery, apart from a prospective study conducted in Sweden.11 Similar to our results, the Swedish authors showed that approximately 70% of the studied cases recorded ≥0.5 D of corneal astigmatism preoperatively and approximately a third had ≥1.0 D. Using postoperative keratometry measurements, the authors found that these proportions remained substantially unchanged after routine cataract surgery.11
It has been reported that mild corneal astigmatism up to 1.5 D can be corrected by operating with the steepest meridian.4 However, cataract surgery with the steepest meridian may be technically difficult and may require less comfortable positioning and therefore it is used less frequently by surgeons.4 This study indicates that surgery off the steepest meridian may have a negative impact on postoperative astigmatism, while those with the meridian did not worsen; therefore, even in cases of milder astigmatism where operating with the steepest meridian is inconvenient, surgeons should consider corrective methods to improve refractive outcomes after surgery.
The main strength of this study resides in the large sample size, reflecting real world clinical practice in terms of patient visits, treatment decisions and data collection and allowing for robust epidemiological data and strong statistical power in comparisons.
In addition, the large sample was taken from a high-quality data source, regularly used in the UK NOD audits.1 While the sample came from a pool of selected clinics, it appeared to be representative of the general cataract surgery patient population in the UK at that time.
Notwithstanding these strengths, we acknowledge some limitations to our study. Only 36% of eyes had postoperative refraction measured and so may not be representative of the entire sample. To investigate this possibility, we examined the preoperative astigmatism and the frequency of complications, co-pathologies and patient age for the 64% (N=70 713) eyes with no postoperative refraction values. These were similar to those of the entire population with regards to average cylinder, incidence of complications, existing co-pathologies and age (data not shown).
Keratometry is not commonly measured following cataract surgery in clinical practice in the UK NHS system. Therefore, different measurements of astigmatism, keratometry and refraction were available presurgery and postsurgery in this study, which limited direct comparison of presurgery and postsurgery astigmatism levels. Finally, only regular astigmatism will be amenable to correction at the time of surgery, and determination of regular versus irregular astigmatism requires corneal topography data that was not available to us.
In conclusion, there is a significant burden of preoperative corneal astigmatism in the UK population of eyes undergoing cataract surgery that is currently not addressed during routine cataract surgery in the UK NHS system. Residual astigmatism may have an impact on the postoperative visual outcomes and quality of life of these patients and therefore, there is a need to improve access to astigmatism-correcting treatment options during cataract surgery.
Acknowledgments
The authors thank the clinicians who contributed data to the study: Mr Gervase Dawidek from the Barking, Havering and Redbridge University Hospitals NHS Trust; Professor Andrew McNaught from the Gloucestershire Hospitals NHS Foundation Trust; Mr Atul Varma from Mid Yorkshire Hospitals NHS Trust; Mrs Rebecca Turner from the Oxford University Hospitals NHS Foundation Trust; Mr Sumit Dhingra from the Peterborough and Stamford Hospitals NHS Foundation Trust; Mr Imran Akram from the St Helens and Knowsley Teaching Hospitals NHS Trust; Mrs Christina Rennie from the University Hospital Southampton NHS Foundation Trust; and Miss Clare Bailey from the University Hospitals Bristol NHS Foundation Trust. The authors specially thank Christine Bouchet, Aldo Martinez, Leighton Morris and Monia Zignani from Alcon, Shoshannah Kalson-Ray, Melissa Myland and Ian Bonzani from Quintiles IMS, and Christian Martin from Medisoft, for their valued contributions to the study design, analyses and interpretation of the results.
References
Footnotes
Presented at The results described in this manuscript were presented at the American Society of Cataract and Refractive Surgery Annual Meeting (Los Angeles, USA, 5–9 May 2017) and the Annual Congress of the Royal College of Ophthalmologists (Liverpool, UK 22–25 May 2017). An additional encore poster was presented at the European Society of Cataract and Refractive Surgery Annual Meeting (Lisbon, Portugal 7–11 October 2017).
Contributors ACD, MD, MSK, FE, CPV, CM, LZ and DFA were involved in the conception and design of the work. CM and LZ were involved in the acquisition and analysis of data for the work. ACD, MD, MSK, FE, CPV, CM, LZ and DFA were involved in the interpretation of data. CM drafted the manuscript. ACD, MD, MSK, FE, CPV, CM, LZ and DFA critically reviewed the manuscript.
Funding This study was sponsored by Alcon (Fort Worth, Texas, US).
Competing interests IQVIA received funding from Alcon Laboratories, Inc to conduct this study. ACD and DFA declare no competing interests. MD and MSK were employees of Alcon Laboratories Inc at the time of research. FE and CPV are employees of Alcon Management SA. CM and LZ are employees of IQVIA.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance