Article Text

Statistics from Altmetric.com
- internal limiting membrane peeling
- epiretinal membrane
- rhegmatogenous retinal detachment
- vitrectomy
- visual acuity
- optical coherence tomography
- dissociated optic nerve fibre layer
Introduction
Macular epiretinal membrane (ERM) formation is a common postoperative complication of pars plana vitrectomy (PPV). The incidence of ERM formation is reported between 6% and 48% following vitrectomy for rhegmatogenous retinal detachment (RRD) in different studies, with the time to ERM formation being around 3–6 months.1–11 ERM formation postvitrectomy is attributed to the migration of retinal pigment epithelium (RPE) cells from the retinal breaks on to the macular surface, where they transdifferentiate into fibroblasts and later proliferate to form a macular ERM.1 2 The internal limiting membrane (ILM) is believed to act as a scaffold for these cells to proliferate.1
Several studies have evaluated the role of adjuvant ILM peeling during primary vitrectomy and found a beneficial effect of ILM peeling in the prevention of postoperative macular ERM formation.3–12 However, the majority of these studies are retrospective.3 5–8 10 11 More importantly, only a single prospective randomised comparative study addresses this topic.9 The visual outcomes of adjuvant ILM peeling as compared with conventional vitrectomy without ILM peeling in RRD are controversial.3–11 While some studies report superior visual acuity in ILM peeled eyes,8 10 others report comparable outcomes.3–7 11 12 A few morphological changes on optical coherence tomography (OCT) following ILM peeling in RRD have been reported, such as retinal dimples and macular thinning,13 but the optic nerve fibre layer changes have rarely been studied and compared between ILM peeled and non-peeled groups.9 Since there were no clinical trials on the role of adjuvant ILM peeling during primary vitrectomy, we conducted a prospective randomised trial to investigate if the anatomical and visual outcomes are superior in patients who undergo PPV for RRD if ILM peeling is performed compared with the conventional PPV group.
Materials and methods
We conducted a single-centre, randomised clinical trial of patients presenting with primary RRD to the outpatient department or the vitreoretina clinic of our tertiary eye care centre. The patient recruitment was planned over a period of 24 months (June 2016–May 2018) as part of a postgraduate thesis.The trial was registered under the Clinical Trials Registry-India (CTRI) and can be accessed at the CTRI website (http://ctri.nic.in).
Recruitment and randomisation
The inclusion criteria for recruitment were patients aged 18–80 years with primary macula-off RRD with proliferative vitreoretinopathy (PVR) grade ≤C1 (Retina Society Terminology Committee classification, 1983)14 and suitable for vitreoretinal surgery and with a minimum follow-up of 6 months after PPV. The exclusion criteria included PVR grade ≥C2, prior vitreoretinal surgery, pre-existing macular pathology including cystoid macular oedema/ERM/macular hole, pre-existing cataract and glaucoma, patients with history of diabetes mellitus and collagen vascular disorders, patients on systemic corticosteroids, and patients unable to follow up.
This study was a parallel-group, two-arm superiority trial with patient enrolment performed by a single author (VK). The enrolled patients were randomised into two groups: group 1 with patients undergoing vitreoretinal surgery without ILM peeling and group 2 with patients undergoing vitreoretinal surgery with ILM peeling. The randomisation was performed using a computer-generated random sequence with a 1:1 allocation ratio by another author (DD) to avoid patient selection bias among investigators. No changes were made to the trial design after commencement of the study. A target sample size of 60 eyes was kept keeping in mind the availability of eligible cases and their follow-up during the study period as per the clinical expectations of the author (VK).
Preoperative evaluation
A detailed history of presenting complaints, including the duration of visual loss and past ocular diseases/treatment, was taken. Ophthalmic examination included corrected distance visual acuity (CDVA), intraocular pressure (IOP), complete anterior and posterior segment evaluation (slit lamp and indirect ophthalmoscopy), and RRD chart drawings noting the configuration of RRD and the location and number of breaks.
Surgical technique
A 25-gauge vitrectomy was performed by a single surgeon (VK) in all cases using Constellation Vitrectomy System (Alcon, USA). An on-site computer system was used to allocate the intervention (done by author DD). The patients were blinded to the allocated treatment. Three standard 25-gauge ports were made through the pars plana, and infusion was started. Port site vitrectomy was done, and this was followed by core vitrectomy. Triamcinolone acetonide was used in all cases to either aid in the induction of posterior vitreous detachment or to confirm the same if already present. Peripheral vitrectomy was completed. ILM peeling was done in group 2 cases with 25-gauge ILM forceps (Grieshaber, Alcon) in the detached retina after staining with Brilliant Blue G dye (0.05%) for 30 s. Approximately 2 disc diameters of ILM centred on the fovea were peeled. A posterior drainage retinotomy, preferably superonasal, was made to drain the subretinal fluid completely and to achieve homogeneity in the surgical steps. Fluid–air exchange was done. Breaks and retinotomy were lasered. A 360° peripheral laser (2–3 rows) was also done in all cases, and 25% sulfur hexafluoride (SF6) gas was used to provide short-term tamponade. Ports were removed, and the port site was sutured with 7–0 vicryl sutures, if required. The patients were advised to be in prone position for 1 week. In the postoperative period, patients were prescribed a combination of topical steroid and antibiotics along with mydriatic-cycloplegic drugs in a tapering fashion for 4 weeks.
Follow-up
Each patient was followed up for at least 6 months, starting from day 1 postoperatively. Each patient was followed up on day 7, and at 1, 3 and 6 months, and 6-monthly thereafter.
At the postoperative visits, the evaluation included CDVA, IOP, lens status (in phakic patients), retinal status (attached/detached), macular status (ERM present or not), presence of dissociated optic nerve fibre layer (DONFL) on en-face macular OCT, and foveal contour, ERM and central macular thickness (CMT) on transverse macular OCT. The follow-up evaluation was performed by another author (DK) who was masked to the randomisation and allocation of treatment.
Outcomes
The primary outcome was the development of macular ERM (diagnosed on OCT) noted until the last follow-up. The secondary outcomes were CDVA, retinal attachment and CMT at last follow-up. The patients who developed cataract (nuclear sclerosis or posterior subcapsular cataract on slit lamp examination) during follow up-were not included in the final outcome analysis as it would confound the visual acuity assessment and need additional surgery.
Macular imaging
Macular imaging (colour fundus photograph and macular OCT) was performed using either a swept-source platform (DRI Triton, Topcon, Oakland, New Jersey, USA) or a confocal scanning laser ophthalmoscope-based imaging system (Spectralis HRA, Heidelberg, Germany) at each follow-up starting at 1 month after surgery. An experienced optometrist performed the imaging in all patients. Both the raster line scans and the en-face images at the level of the inner macular surface were evaluated (DK) for the presence of ERM, morphological changes and CMT. ERM was diagnosed based on the presence of a highly reflective line on the inner macular surface. To avoid differences in CMT measurement by the swept-source-based and confocal laser-based OCT systems, the CMT was measured manually at the fovea from the innermost retinal layer to the outer portion of RPE with the help of an inbuilt calliper. DONFL was diagnosed as concentric macular dark spots on en-face images. The outcomes were finally recorded in an Excel spreadsheet (by author DD) as per the allocated groups.
Statistical analysis
Statistical analysis was performed using IBM SPSS V.22 software. Qualitative data were expressed as frequency as well as percentages. The Snellen visual acuity was converted into logarithm of the minimum angle of resolution (logMAR) units with counting fingers vision at a distance of 33 cm and hand movements corresponding to 2.3 units and 3.0 units, respectively, as per the criteria given by Holladay.15 Intergroup analysis was done using two-sample Student’s t-test for parametric data and Mann-Whitney test for non-parametric data. Categorical data were subjected to Pearson’s χ2 test or Fisher’s exact test for comparison between the groups. χ2 test was used if the cell value was ≥5 in all the cells of the contingency table. If any cell had value <5, Fisher’s exact test was used. Freeman-Halton extension of Fisher’s exact test was used for analysis of any cell value <5 in larger than 2×2 contingency tables. Comparison of continuous data over follow-up was done using paired t-test for parametric data and two-samples Wilcoxon signed-rank test for non-parametric data. A p value ≤0.05 was considered statistically significant.
Results
Out of a total of 214 eyes assessed for recruitment, 68 eyes of 68 patients were found to be eligible. The rest of the patients either had PVR grade ≥C2 or had pre-existing macular or systemic diseases. Seven patients (four in group 1 and three in group 2) were either lost to follow-up or refused further involvement due to reasons unrelated to adverse effects (personal). One patient in group 1 developed cataract on follow-up and was excluded from analysis. The rest (60 patients) completed the minimum 6-month follow-up, with 30 cases in each group (online supplementary file 1). The last recruitment was performed in April 2018, and the last follow-up was completed in October 2018.
Supplemental material
The two groups were statistically comparable in terms of baseline parameters such as sex distribution, age, duration of RRD, baseline CDVA and lens status (table 1). Although the median number of breaks and quadrant of RRD involvement was greater in the ILM peeled group, the difference was not statistically significant. One patient (group 1) had vitreous haemorrhage. The median follow-up in groups 1 and 2 was 15.5 (range 6–24) months and 14 (range 6–24) months, respectively, with no significant difference (p=0.37). The outcomes are shown in table 2.
Baseline demographics and clinical parameters of eyes undergoing vitrectomy with or without ILM peeling for primary RRD
Visual and anatomical outcomes in eyes undergoing vitrectomy with or without ILM peeling for primary rhegmatogenous retinal detachment
Primary outcome
Twenty per cent (n=6) of the eyes in the non-ILM peeling group developed macular ERM as noted on OCT on follow-up, while none of the eyes in the ILM peeling group developed macular ERM, with a statistically significant difference (p=0.002). However, resurgery (ERM plus ILM peeling) was required in only one eye out of six eyes developing ERM in the non-ILM peeling group due to poor visual acuity (figure 1). ERM was noted and resurgery was performed for this case at 6 months, and the visual acuity before repeat surgery was used for outcome analysis. Also, six of the eyes in the ILM peeling group developed extramacular ERM (just outside the area of ILM peeling) on follow-up (figure 2).

Six-month follow-up fundus imaging of a case of macula-off rhegmatogenous retinal detachment that underwent vitrectomy and gas tamponade without internal limiting membrane peeling. (A) The fundus photograph shows the presence of a thick epiretinal membrane causing wrinkling of the macula. (B) The swept-source optical coherence tomography line scan along the black arrow in ‘A’ shows a hyper-reflective line at the macular surface suggestive of epiretinal membrane (white arrows), inner retinal disorganisation and relative preservation of the outer retinal bands.

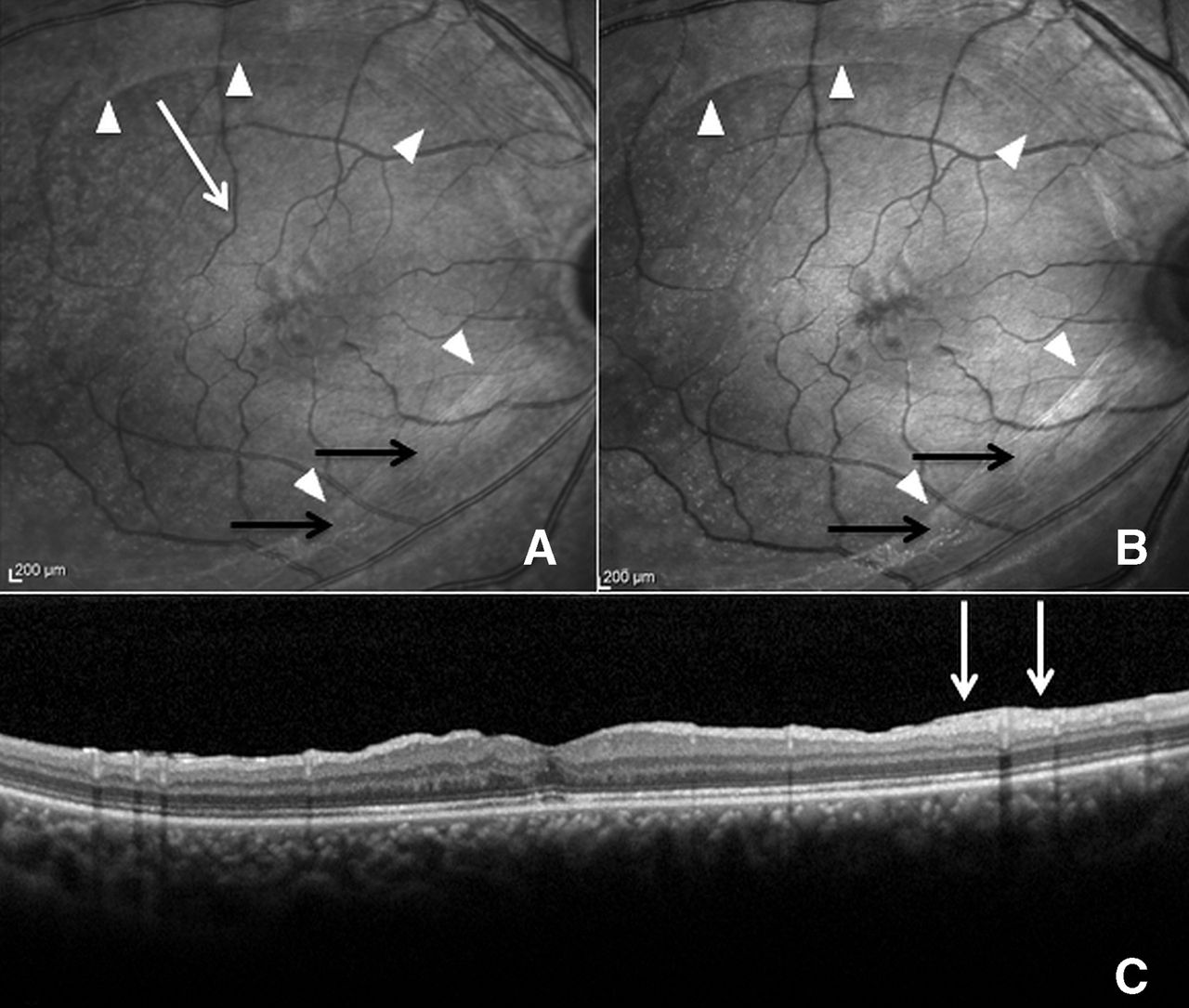
Fundus imaging of a case of macula-off rhegmatogenous retinal detachment that underwent vitrectomy and gas tamponade with internal limiting membrane (ILM) peeling. (A) The fundus photograph shows epiretinal membrane (black arrows) outside the area of ILM peeling with a sharp junction (white arrowheads) between the two regions. (B) The red-free image delineates the membrane (black arrows) as well as the junction (white arrowheads) better. (C) The spectral domain optical coherence tomography line scan along the white arrow in ‘A’ shows a normal foveal contour, normal retinal architecture and a thick hyper-reflective membrane on the surface on the right side of the scan (white arrows) suggestive of extramacular epiretinal membrane as seen in ‘A’.
Secondary outcomes
Retinal reattachment was attained in all eyes of both groups. None of the eyes developed iatrogenic hole formation or PVR or redetachment. None of the eyes had high IOP at last follow-up or required antiglaucoma medications. CDVA improved in both groups significantly from baseline following retinal reattachment surgery to 0.59±0.46 logMAR units (median 0.55, range 0.18–2.3) in the non-ILM peeling group and to 0.68±0.48 logMAR units (median 0.5, range 0.18–2.3) in the ILM peeling group at last follow-up (p<0.0001 and p<0.0001, respectively). However, there was no significant difference in the final CDVA between the groups (p=0.43).
Concentric retinal dark spots, that is, DONFL, were found in 40% of the eyes (n=12/30) in the ILM peeling group (figure 3), while none of the eyes in the non-ILM peeling had DONFL, with a statistically significant difference (p=0.0001). DONFL appeared as early as 1 month of follow-up and persisted until the last follow-up. The mean final CMT of the non-ILM peeling group was 266.0±37.5 µm and that of the ILM peeling group was 270.0±73.7 µm, with no significant difference in the two groups (p=0.62).

{kind=link}
{kind=link}
{kind=link}
En-face imaging at the level of the macular surface of a case of macula-off rhegmatogenous retinal detachment that underwent vitrectomy and gas tamponade with internal limiting membrane peeling. Multiple concentric macular dark spots/lines are seen suggestive of dissociated optic nerve fibre layer (black arrows).
On univariate analysis, none of the baseline factors such as sex, age, duration of RRD and baseline CDVA significantly affected the occurrence of DONFL in the ILM peeling group (online supplementary file 2). Also, the appearance of DONFL in the ILM peeling group did not significantly affect the final CDVA and CMT (online supplementary file 2).
Supplemental material
Discussion
Several retrospective studies have evaluated the benefits and limitations of ILM peeling during PPV in RRD eyes (online supplementary file 3).3 5–8 10 11 Only two prospectively conducted studies have evaluated and compared the visual and anatomical outcomes between ILM peeled eyes and non-ILM peeled eyes (online supplementary file 3).4 9 The prospective randomised comparative study by Eissa et al9 was limited by its smaller sample size. The authors used silicone oil tamponade in all their cases despite the detachments being fresh.9 It is believed that silicone oil tamponade affects the retinal ultrastructure by causing degeneration of the inner retinal layers and therefore may have confounded the results.16 Also, a statistically significant difference existed in the duration of RRD between the ILM peeled and the non-peeled group.9 The increased duration of detachment in the ILM peeled group may have been responsible for the inferior visual outcomes in this group as compared with the non-ILM peeled group.9 The second prospective non-randomised study, by Odrobina et al,4 included cases with severe PVR which required retinectomy and silicone oil tamponade. The results from these two prospective studies may not be generalised and compared with other studies evaluating the role of ILM peeling in fresh RRD managed with vitrectomy and gas tamponade.
Supplemental material
The incidence of postoperative ERM formation following PPV for RRD has been reported between 6% and 47.7% of eyes in the non-ILM peeling group and between 0% and 10% in ILM peeled eyes in previous studies.1–12 The incidence in our study is in accordance with the existing literature, with ERM formation in 20% of non-ILM peeled eyes and none of the ILM peeled eyes developing macular ERM. Previous studies have not reported the occurrence of extramacular ERM in ILM peeled eyes (online supplementary file 3). The incidence of extramacular ERM in the ILM peeled group in our study was similar to the incidence of macular ERM formation in non-peeled group (20% in each group). Since the two groups were comparable in all baseline characteristics, our prospective study confirms that the ILM peeling prevents postoperative ERM formation in the ILM peeled area in RRD eyes. ILM normally provides a scaffold for RPE and glial cells to settle and proliferate.1 2 Macular ILM peeling removes this scaffold and therefore prevents macular ERM formation. However, the ERM did develop outside the peeled area where the ILM scaffold was still persisting. This again strengthens the ‘ILM scaffold’ concept for ERM formation. Extramacular ERM formation even after ILM peeling is a novel finding which previous studies have not highlighted. This also guides us to the size of ILM peeling needed in such cases. Perhaps an ILM peel in the entire macular area (2 disc diameters all around the fovea) will be more beneficial than a smaller-sized peel.
The majority of previous studies reported comparable CDVA in ILM peeled and non-peeled eyes at the final follow-up (range 6–30 months),3–7 11 while a few reported superior CDVA in ILM peeled eyes (online supplementary file 3).8 10 In our study, the final CDVA did not differ significantly between the two groups. The macular ERM in the non-peeled group was not clinically significant until the final visit except in one case. It is plausible that with a longer follow-up, ERM may become thicker and lead to outer retinal distortion, and then the visual outcome difference may reach significance.
The peeling of ILM in a detached retina does pose a surgical challenge. In RRD, the Muller cell growth increases onto the retinal surface, and their forced avulsion during ILM peeling is more likely to disturb the retinal structure.13 17 DONFL is thought to occur after ILM peeling due to Muller cell end-feet loss in the peeled area.18 19 DONFL occurred in 40% of ILM peeled eyes in our study as compared with 100% incidence reported by Eissa et al.9 The higher incidence in the previous study may be due to the use of perfluorocarbon liquid (PFCL) during ILM peeling.9 Okamoto et al reported a higher incidence of DONFL during primary ERM surgery in PFCL-assisted peeling group as compared with conventional peeling group.20 It is possible that under the influence of PFCL, the displacement angle of peeling increases with a stronger tractional force and damage to the Muller cell foot processes.20 DONFL is usually thought to be clinically insignificant.18 19 21–24 Similar to existing literature, the presence of DONFL did not affect the final CDVA in our study.
The present study was the first prospective randomised trial performed in RRD cases without significant PVR, which were managed only with short-term gas tamponade. Other strengths of this study were its design (prospective trial), comparatively longer follow-up (median follow-up of around 15 months), matched baseline parameters (sex, age, duration of RRD and baseline CDVA), standard and similar intraoperative procedure (25-gauge vitrectomy, triamcinolone-assisted vitrectomy, posterior retinotomy and 360° peripheral endolaser in all cases) between the two groups, and single retinal surgeon which prevented surgeon bias. Since cataract may develop or progress following vitrectomy with gas tamponade and affect final visual acuity, and cataract surgery may also affect the final visual acuity and risk of ERM formation, we excluded patients with pre-existing cataract or those who developed cataract on follow-up.
The study had a few limitations. Advanced PVR cases were excluded to achieve homogeneity in SF6 tamponade. Such cases often require silicone oil tamponade and encirclage element which might have confounded the results. However, this led to a smaller number of cases allocated to each group. Although the sample size is smaller as compared with most of the retrospective studies, the study has the advantage of being a prospective randomised trial. The CMT was measured on two different OCT platforms; we believe manual measurement with the inbuilt callipers may have reduced the bias. The peeling of ILM does cause some amount of mechanical trauma to retinal microstructures, which might affect the quality of vision, if not visual acuity.13 Other than visual acuity, the functional outcomes were not assessed in terms of the presence of metamorphopsia and retinal sensitivity. The eyes with DONFL may have been further assessed with functional imaging such as microperimetry or 10–2 Humphrey visual field testing. The minimum follow-up of 6 months may have been short to detect any difference in visual acuity between the two groups. As mentioned previously, fine ERM detected only on OCT at final follow-up may not be visually significant and needs further evaluation. The total surgical time was not recorded for the patients, and it may be possible that with longer duration of surgery there happens greater ocular inflammation which confers a higher risk of postoperative ERM formation.
A meta-analysis of existing studies by Fallico et al12 shows that while ILM peeling during vitrectomy for RRD is effective in preventing macular ERM formation and recurrence of detachment postoperatively, a corresponding superior visual outcome is not achieved. Based on the benefit of ILM peeling in preventing ERM formation and the inconspicuous nature of DONFL arising out of ILM peeling, we believe that ILM peeling may be routinely performed in macula-off RRD to prevent postoperative ERM formation. The key aspect is that the peel should be gently performed, preferably without PFCL use and be of size just enough to cover the macular area.
To conclude, this prospective randomised controlled trial confirms the beneficial role of ILM peeling in the prevention of ERM formation in the peeled area in eyes undergoing PPV for RRD, but with similar visual outcomes as compared with conventional treatment. However, extramacular ERM may still develop after macular ILM peeling. This signifies the role of ILM as a scaffold for ERM development and the need for an ILM peel of adequate size. Macular ERM may grow over time, and a longer follow-up is required to determine if visual outcomes worsen in the non-peeled eyes in the long run.
Acknowledgments
Our research institute and hospital provided monetary and material support.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work: VK, DD, DK. Acquisition, analysis or interpretation of data: VK, DD, DK, AM, PC, MC, AK. Drafting the work: VK, DD, DK, AM. Revising it critically for important intellectual content: VK, PC, MC, AK. All authors approved the final manuscript and agree to be accountable for all aspects of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study adhered to the tenets of the Declaration of Helsinki. Institutional ethics committee approval was obtained. All enrolled patients gave written informed consent for participation in the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.