Article Text

Abstract
Background The 0.2 µg/day fluocinolone acetonide (FAc) implant delivers continuous, low-dose, intravitreal corticosteroid for the treatment of diabetic macular oedema (DMO). This ongoing, 3-year, observational clinical trial provides long-term, ‘real-world’ safety results for the FAc implant in DMO.
Methods This 24-month interim analysis of a prospective, observational study investigated patients with DMO receiving the commercially available intravitreal 0.2 µg/day FAc implant. The primary outcome was incidence of intraocular pressure (IOP)-lowering procedures. Other IOP-related signals and their relationship to previous corticosteroid exposure, best-corrected visual acuity, central subfield thickness (CST), ocular adverse events and frequency of other treatments were also measured.
Results Data were collected from 95 previously steroid-challenged patients (115 study eyes) for up to 36 months pre-FAc and 24 months post-FAc implant. Mean IOP for the overall population remained stable post-FAc compared with pre-FAc implant. IOP-related procedures remained infrequent (two IOP-lowering surgeries pre-FAc; two trabeculoplasties and four IOP-lowering surgeries post-FAc). Mean visual acuity was stable post-FAc (mean improvement of 1–3 letters) and fewer DMO treatments were required per year following FAc implant. Mean CST was significantly reduced at 24 months post-FAc implant (p<0.001) and the percentage of patients with CST ≤300 µm was significantly increased (p=0.041).
Conclusion Few IOP-related procedures were reported during the 24 months post-FAc implant. Positive efficacy outcomes were noted after treatment, with stabilisation of vision and reduction in inflammation, demonstrated by CST. The FAc implant has a favourable benefit–risk profile in the management of DMO, especially when administered after a prior steroid challenge.
Trial registration number NCT02424019.
- inflammation
- intraocular pressure
- macula
- retina
- treatment other
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes mellitus is a complex disease; approximately 35% of patients develop diabetic retinopathy, and 7% progress to diabetic macular oedema (DMO), a severe vision-threatening stage of diabetic retinopathy.1 Hyperglycaemia is a major contributing factor to the pathogenesis of DMO; it leads to neuroinflammation, oxidative stress and vascular dysfunction within the retina. Emerging evidence suggests that low-grade chronic intraretinal inflammation serves as a critical early contributor to the development of oedema and pathogenic vascularisation.2
Currently, intravitreal antivascular endothelial growth factor (anti-VEGF) agents are the first-line treatment for eyes with central-involved DMO.3 Administration of anti-VEGF treatments is commonly required at intervals as frequent as monthly.4–6 A post-hoc analysis of the Diabetic Retinopathy Clinical Research Network (DRCR.net) Protocol T trial found that 32%–66% of eyes had persistent DMO at 24 weeks, despite three to six consecutive monthly injections, and 60%–71% of these eyes required rescue laser treatment at 1 year.7 These data suggest that anti-VEGF therapies may not always provide complete resolution of oedema or improvement in vision, even after multiple injections and years of treatment. Furthermore, two real-world datasets (Vestrum and IRIS) have shown that in clinical practice, patients with DMO are commonly dosed less frequently than in pivotal trials, often resulting in less visual acuity (VA) improvements.8 9 In addition, patients with diabetes have a higher rate of non-adherence to anti-VEGF intravitreal treatments than those without diabetes10 and previous publications have indicated that the efficacy of anti-VEGF is directly related to the frequency of injections.11
The use of corticosteroid intravitreal implants is currently second-line treatment for DMO because of steroid-related side effects, such as intraocular pressure (IOP) elevation and cataract formation.12 Corticosteroids can target inflammatory molecules involved in the pathological process of DMO, including angiopoietin-2, tumour necrosis factor-alpha and various other chemokines.13 The fluocinolone acetonide (FAc; ILUVIEN, Alimera Sciences, Alpharetta, Georgia, USA) intravitreal implant releases submicrogram levels (0.2 µg/day) of the corticosteroid into the vitreous for approximately 36 months.14
The Fluocinolone Acetonide for Diabetic Macular Edema (FAME) studies previously demonstrated the efficacy of the 0.2 µg/day FAc implant for patients with DMO, with significant improvement in best-corrected visual acuity (BCVA) compared with sham control over a 36-month period. However, IOP-related adverse events (AEs; 4.8% vs 0.5% for IOP-related surgery, FAc implant vs sham, respectively) and incidence of cataracts were higher in the FAc implant group than in the sham group.15 In a post-hoc analysis, the FAME investigators found that patients with evidence of prior steroid exposure did not require IOP-lowering surgery compared with patients who were corticosteroid naive (0% and 6.1%, respectively, p<0.03).16 The FAc implant was approved in the USA in 2014 ‘for the treatment of DMO in patients who have been previously treated with a course of corticosteroids and did not have a clinically significant rise in IOP’.17
The US Retrospective Chart Review in Patients Receiving ILUVIEN (USER) study showed improvements in treatment frequency and retinal thickness, and maintenance of VA following the FAc implant, in a real-world patient population. IOP outcomes were similar pre-FAc and post-FAc implant, suggesting that the US prescribing indication requiring all patients eligible for the FAc implant to have received prior corticosteroids without a clinically significant rise in IOP, markedly reduced IOP-related events compared with the results in the FAME studies.18
Patients with DMO already have a considerable overall treatment burden, with an average of more than two healthcare-related appointments per month and one ophthalmology-related visit every other month.19 As such, there is a great need for a DMO treatment that provides long-term control of DMO, but with reduced frequency of treatments and an acceptable side-effect profile.
The PALADIN study (NCT02424019) is being conducted to assess the long-term safety of the FAc implant in patients with DMO over 36 months, with the primary focus on IOP. It is the first postcommercialisation, prospective trial to assess safety in a real-world population treated according to the US prescribing indication requirement for patients to have received previous corticosteroid treatment without a clinically significant rise in IOP. The results of the 24-month interim analysis are presented here.
Methods
The PALADIN study is a phase IV, real-world, prospective, non-randomised, open-label and uncontrolled trial across multiple sites in the USA. The observation phase is ongoing, with a planned duration of follow-up of 3 years, with patients recruited from May 2015 onwards. The study assesses the safety outcomes of the 0.2 µg/day FAc implant in patients with DMO who have previously received ocular corticosteroids without a clinically significant rise in IOP (based on the treating physician’s judgement).20 Eligibility criteria and FAc implant administration are described in online supplementary appendix S1. Patient assessments are outlined in online supplementary table S1. All patients provided written consent prior to their participation.
Supplemental material
The primary objective was to determine the incidence of IOP-lowering procedures (incisional surgery for ocular hypertension) in patients treated with the FAc implant according to the US prescribing label. The secondary objectives of the study were to evaluate the incidence of other IOP-related signals, determine if the IOP-related signals observed post-FAc implant are correlated to any IOP-related signals noted after previous corticosteroid exposure and measure the incidence of other safety signals not related to IOP. Additional analyses examined the effect on VA and central subfield thickness (CST), with post-hoc analyses also assessing treatment frequencies pre-FAc and post-FAc implant; a study protocol amendment allowed collection of data, up to 36 months prior to the FAc implant treatment, including IOP, VA and CST, to be used to compare pre-FAc and post-FAc implant. Further details regarding investigation methods are described in online supplementary appendix S2.
Results
Baseline demographics
A total of 95 patients with 115 study eyes were analysed at the 24-month interim analysis for the PALADIN study; baseline demographics are shown in table 1.
Baseline demographics of patients from the PALADIN study
Intraocular pressure
Mean IOP (and SD) over time for the overall study population remained stable post-FAc compared with pre-FAc (figure 1A).

(A) The mean intraocular pressure (IOP) (SD) over time pre-fluocinolone acetonide (FAc) and post-FAc and (B) best-corrected visual acuity (BCVA) post-FAc in patients with baseline BCVA ≥20/40 and BCVA <20/40.
Although the number of incisional IOP-related procedures due to intraocular steroid use increased post-FAc implant compared with pre-FAc implant, it was not statistically significant (3.5% and 1.7%, respectively, p=0.414; table 2).
Intraocular pressure (IOP) events pre-fluocinolone acetonide (FAc) and post-FAc implant (24-month cut-off, n=115 eyes)
There was a significantly greater proportion of individual patients with peak IOP elevations above 25 mm Hg post-FAc compared with pre-FAc (23.5% vs 12.1%, respectively, p=0.007), and the number of patients requiring any IOP-lowering medication significantly increased post-FAc compared with pre-FAc implant (40% and 9.6%, respectively, p<0.001; table 2); nevertheless, 76.5% of patients did not exceed the predefined thresholds for IOP elevation. The percentage of patients who had an elevation to >30 mm Hg was 7.9% and 4.0%, post-FAc and pre-FAc implant, respectively (p=0.132).
In the overall population, for patients who had previous corticosteroid treatments without significant rise in IOP, the positive predictive value (PPV) of the maximum observed IOP remaining ≤25 mm Hg (95% CI) was calculated as 79.6% (online supplementary table S2). The PPVs for maximum observed IOP were 85.7%, 84.1% and 60.0% for patients previously treated with a single intraocular dexamethasone (DEX) implant treatment (29 eyes), >1 previous DEX implant treatment (45 eyes; mean 3.3 treatments) or sub-Tenon triamcinolone acetonide injections (5 eyes), respectively. The PPV for the last observed IOP post-FAc implant remaining ≤25 mm Hg was 97.8%.
Cataract-related events
Of the 12 phakic eyes that completed the study through to month 24, 8 (66.7%) required cataract extraction. Of the 12 eyes that were phakic at baseline, a mean increase of 3.7 letters was observed in BCVA 24 months post-FAc compared with baseline.
Visual acuity
Retrospective VA data collection during the 36 months pre-FAc implant showed a steady rate of deterioration in VA for all patients. There was a mean reduction of 8 and 10 letters in patients with baseline VA ≥20/40 and baseline VA <20/40, respectively. Prospective BCVA data collected 24 months post-FAc implant showed BCVA remained stable in all patients, regardless of baseline VA (figure 1B). There was a mean improvement of 1 letter and 3 letters in patients with baseline BCVA ≥20/40 and patients with baseline BCVA <20/40, respectively.
Patients with a worse baseline BCVA score (<20/40) had a greater deterioration pre-FAc implant compared with patients with a better baseline BCVA score (−10 compared with −8, respectively) and a greater improvement post-FAc implant (+3 compared with +1, respectively).
Treatment frequency shift
The number of DMO treatments required per year was reduced in the 24 months after FAc implant compared with the 24 months prior to FAc (figure 2A). After the FAc implant, the proportions of eyes with a treatment frequency per year of 0–1 treatment, >1–4 treatments or >4 treatments were 51%, 34% and 15%, respectively, favouring fewer treatments. In contrast, before the FAc implant, the proportions of eyes with a treatment frequency per year of 0–1, >1–4 or >4 treatments were 16%, 55% and 29%, respectively.

Treatment frequency shift data assessed by (A) yearly treatment frequency shift and (B) time to rescue treatments. FAc, fluocinolone acetonide.
In the Kaplan-Meier time-to-rescue analysis, the majority of patients in the full population did not require rescue treatment for at least 1 year following the FAc implant (figure 2B). At 358 days post-FAc implant (~1 year), 48.1% of patients had received some form of rescue treatment but at 24 months post-FAc implant, 43.7% of patients had still not required any rescue treatment.
Retinal thickness
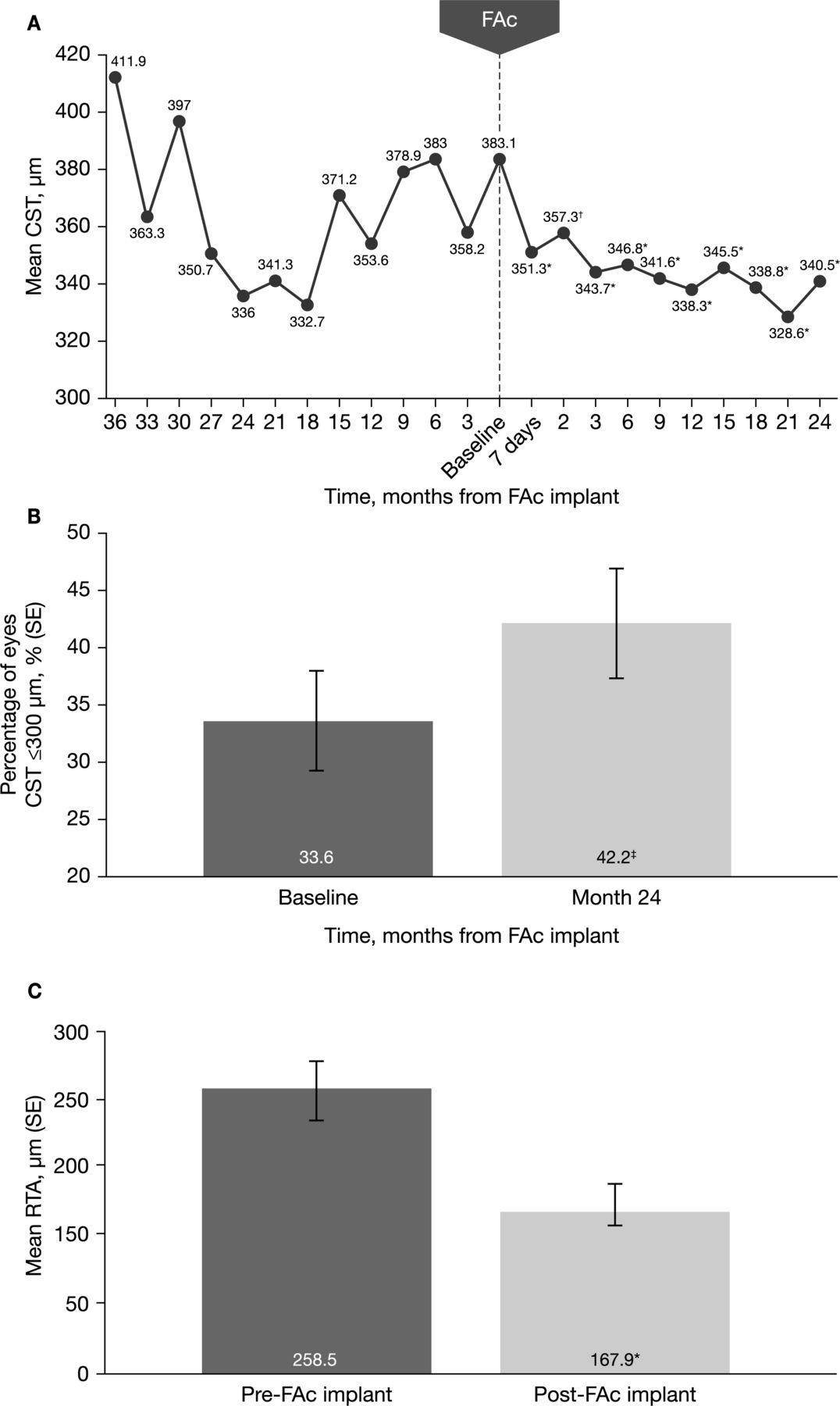
A continuous, gradual reduction in mean CST was demonstrated over 24 months post-FAc compared with 36 months pre-FAc (figure 3A). The reduction was significant from day 7 post-FAc implant (p<0.001) and remained so for all timepoints to month 24 post-FAc implant (p<0.001). The mean CST range was 332.7–411.9 µm and 328.6–357.3 µm for pre-FAc and post-FAc implant, respectively.

{kind=link}
{kind=link}
{kind=link}
Central subfield thickness (CST) outcomes in 113 eyes measured by (A) mean CST pre-fluocinolone acetonide (FAc) and post-FAc implant, (B) the percentage of eyes with CST ≤300 µm (SE) at baseline and 24 months post-FAc implant and (C) mean retinal thickness amplitude (RTA) of CST (SE) pre-FAc and post-FAc implant. *p<0.001, †p=0.013, ‡p=0.041.
The percentage of patients with CST ≤300 µm significantly increased post-FAc compared with baseline (figure 3B). The percentage of eyes with CST ≤300 µm was significant at 12 months (46.3%, p=0.009) and 24 months (42.2%, p=0.041).
A significant reduction in the mean retinal thickness amplitude (RTA) of CST was observed post-FAc implant compared with pre-FAc (167.9 µm and 258.5 µm, respectively, p<0.001), accompanied by a reduction in retinal thickness fluctuations (figure 3C).
Discussion
The PALADIN study has demonstrated improved control of macular oedema after FAc implantation, as evidenced by the stabilisation and improvement in BCVA, the increased percentage of eyes with CST ≤300 µm, the reduced RTA and the decreased need for additional therapies. The safety results of this study are consistent with known side effects of intravitreal steroids,15 18 showing an elevation in IOP and cataract formation in some patients. However, the changes in IOP were predominantly mild and manageable with topical IOP-lowering therapy. These results indicate that the benefit–risk evaluation of the FAc implant is well defined and potentially favourable for patients who have been previously treated with a course of corticosteroids without a clinically significant rise in IOP.
IOP outcomes
In this study, the number of IOP-related procedures increased post-FAc implant. This increase was partially due to other aetiologies of high IOP, independent from steroid-induced pressure elevations. One patient required laser therapy post-FAc implant for acute angle closure glaucoma and two of the four patients requiring incisional IOP-lowering surgery post-FAc implant were treated for neovascular glaucoma (a known complication of progressive diabetic retinopathy21). Therefore, the number of steroid-induced IOP-related surgical glaucoma procedures remained similar pre-FAc and post-FAc implant.
Overall, the mean IOP following FAc implant administration was stable over time, demonstrating that the majority of patients had manageable IOP. The number of patients requiring IOP-lowering medications did significantly increase post-FAc treatment (40.0% post-FAc compared with 9.6% pre-FAc, respectively), which is comparable with previous studies.15 18 The Macular Edema: Assessment of Implantable Dexamethasone in Diabetes (MEAD) study demonstrated a similar rate of patients requiring IOP-lowering medications with serial dosing of intravitreal DEX 0.7 mg over 39 months (41.5% of patients requiring IOP-lowering medication for DEX implant compared with 9.1% for sham).22 Despite the increase in IOP-lowering medications post-FAc implant in the current study, the percentage of patients who had an IOP elevation >30 mm Hg remained stable pre-FAc and post-FAc implant, and the number of IOP-related AEs requiring surgical intervention did not increase significantly post-FAc compared with pre-FAc implant, suggesting that overall, patients were successfully managed without surgery.
In the FAME studies, overall IOP-related AEs were more frequent in the FAc implant group than in the sham group.15 The USER study found a numerical but non-statistically significant decrease in the incidence of IOP-related events post-FAc implant compared with pre-FAc implant; however, the mean follow-up after administration was only approximately 12 months.18 In the current study, no statistically significant increase in IOP-related AEs requiring surgery was observed. The variation in the results between these three studies can be accounted for by the use of the FAc implant according to treatment indication in the USER and PALADIN studies; the indication specifies FAc implant administration following prior treatment with a corticosteroid without a significant rise in IOP.
The PPV of IOP remaining ≤25 mm Hg if the patient had prior intraocular corticosteroid treatment without clinically significant elevation in IOP (79.6%) further supports previous intraocular steroid use as an important risk indicator when considering prescribing the FAc implant, as originally reported in the USER study.18 Furthermore, the PPV for the last observed IOP post-FAc implant remaining ≤25 mm Hg was 97.8%; this demonstrates that even for that minority of patients who developed elevated IOP post-FAc implant (~20%), almost all of these had their ocular hypertension effectively managed. Using intraocular DEX as the prior corticosteroid treatment produces similar PPVs for FAc implant outcome, regardless of the number of previous treatments (85.7% and 84.1% for one treatment and more than one treatment, respectively). Additionally, the low predictive value for FAc implant outcome with prior sub-Tenon’s injection (60.0%) could indicate that a sub-Tenon’s challenge may not be as good an assessment for potential steroid IOP response as intraocular steroid use; however, the sample size was very small (n=5). No topical steroid challenge was listed by the PALADIN investigators.
Cataract-related events
The very small population of phakic eyes at baseline still had an overall good outcome post-FAc implant, with an increase in mean BCVA compared with baseline. This is consistent with good results in phakic patients undergoing cataract surgery in intravitreal DEX trials.15 22
VA outcomes
All eyes had received DMO treatment prior to enrolment in this study; however, despite these previous therapies, only a third of the study eyes had BCVA ≥20/40. The retrospective observation of patients prior to the FAc implant showed a gradual decline in VA over the 36-month period and an associated increase in frequency of treatments. BCVA stabilised for the 24 months post-FAc implant, with substantially reduced recurrence and fluctuation of oedema, as measured by the reduced frequency of treatments to achieve this. The current findings of the change in BCVA post-FAc implant in this study show comparable outcomes to previous studies15 18; however, these previous results are now demonstrated in a real-world setting over an extended, 24-month period.
Treatment burden
Patients with diabetes and DMO have a significantly higher diabetes-related comorbidity burden than matched patients with diabetes without DMO.19 The PALADIN study demonstrated the FAc implant results in a meaningful reduction of DMO-associated injection burden for patients, and this may also result in improved patient adherence for all aspects of their diabetes management. Despite the ongoing visit burden associated with any intravitreal steroid therapy (assessing IOP and cataract advancement in phakic patients), there is a significant practical benefit to reducing the injection burden. In addition to injection-related risks from intravitreal treatment (eg, endophthalmitis), approximately 75% of patients reported anxiety about receiving their most recent intravitreal injections, and >40% of respondents indicated that receiving fewer injections, to achieve similar visual results, would improve the treatment regimen.23
Other DMO therapies have been shown to provide improvement in vision and macular oedema24 25; however, the injection protocol for anti-VEGF agents, for example, is up to five consecutive monthly administrations during the induction phase followed by monthly or bimonthly injections.24 There are data supporting a reduction in the frequency of anti-VEGF monotherapy over time on average, but induction therapy requires frequent injections for 1 to 2 years on average,4 25–27 and some patients require frequent, ongoing suppression of VEGF to maintain macular anatomy and VA. This has implications for an increased treatment burden on patients.26 27 Moreover, real-world studies have shown worse therapeutic outcomes for anti-VEGF therapies compared with results from randomised controlled trials.8
The PALADIN study demonstrated a reduction in yearly injection frequency post-FAc implant, and the percentage of patients who were treatment free (ie, no additional anti-VEGF treatments, steroid injections or laser) for the 24 months post-FAc implant was 43.7% in the full population. In addition, the percentage of patients who required a higher number of treatments (>4 treatments per year) reduced from 29% pre-FAc to 15% post-FAc implant. Contrastingly, a systematic review of real-world studies of DEX implants indicated that an average of 37% of eyes required retreatment before 6 months from first injection and that the mean retreatment time was approximately 5 months.28 The difference in time to retreatment between the DEX implant and the FAc implant may be accounted for by differing release kinetics, as well as FAc being approximately 50% less water soluble than DEX and consequently, has a longer half-life in the vitreous.29 30
Retinal thickness outcomes
The significant reduction in mean CST from 7 days post-FAc implant shows the anti-inflammatory properties of the FAc implant target a significant pathological component of DMO quickly in some patients.
The significant increase in the percentage of eyes with CST ≤300 µm (42.2% post-FAc compared with 33.6% pre-FAc, p=0.041) demonstrates that, in this group of patients, the steroid effect has a positive and long-lasting anatomic benefit, ongoing at 24 months after implantation. These data, along with the reduced fluctuation in CST post-FAc implant, demonstrate that, in this group of patients, long-term steroidal treatment reduces recurrences of oedema, possibly through its anti-inflammatory effect, which may lead to long-term visual improvement and stability.31 In PALADIN, the mean RTA of CST, an additional measure of oedema control, was significantly reduced post-FAc compared with pre-FAc implant (167.9 µm and 258.5 µm, respectively, p<0.001), with previous studies showing similar findings.32
An important limitation to this study is that the pre-FAc implant VA measurements were retrospectively obtained values, and not necessarily consistently measured; this should be considered when interpreting the greater consistency in BCVA results following the FAc implant. A further limitation of this analysis involves the interim data collection; 3-year outcome data will be helpful to confirm these initial findings for all endpoints.
Conclusion
This study demonstrates that long-term treatment with the 0.2 µg/day FAc implant is well tolerated and that the anticipated, predictable side effects are manageable in real-world dosing. Appropriate patient selection is encouraged by the US Food and Drug Administration labelling of the FAc implant, and the data from this study support that the label is effective in mitigating the risk of uncontrolled IOP. Most patients who developed an increase in IOP did not require surgical interventions and treatment with topical medications was typically sufficient to control IOP. The efficacy outcomes suggest that the long-term, continuous microdosing with FAc leads to fewer recurrences of oedema, as measured by the reduced need for rescue treatment post-FAc implant and the reduction in mean RTA. The consistent control of macular oedema was demonstrated by the reduction of retinal thickness and stable BCVA over the duration of therapy. These real-world data indicate that the FAc implant is a valuable tool in the management of DMO for selected patients.
Acknowledgments
The authors would like to thank all the participants of the PALADIN study. Medical writing support for this article was provided by Catherine Sidaway, MBChB, Helios Medical Communications, Alderley Edge, Cheshire, UK, which was funded by Alimera Sciences.
References
Footnotes
Contributors SEM assisted with the design of the study and interpretation of data. DE and DBR assisted with the interpretation of data. DFK, NMH and EW assisted with the acquisition, analysis and interpretation of data. SK assisted with the analysis and interpretation of data. All authors were involved in writing and critically appraising the manuscript and approving the final version to be published.
Funding Sponsorship for this study and article processing charges were funded by Alimera Sciences.
Competing interests SEM has received clinical trial research funds from Alimera Sciences, Chengdu Kanghong Biotechnology, Clearside Biomedical and Genentech. DFK has received research support from Adverum, Alimera Sciences, Allergan, EyePoint and Graybug Pharmaceuticals, received consultant fees from Adverum, Alimera Sciences, Allergan, BVI, EyePoint, Genentech, Mallinckrodt, Notal Vision, Novartis, Physician Recommended Neutriceuticals and Regeneron, and participated in speakers bureau for Alimera Sciences, Allergan, EyePoint, Genentech, Mallinckrodt, Notal Vision, Physician Recommended Neutriceuticals, Regeneron and Spark Therapeutics. DBR has received personal fees from Alimera Sciences, Allergan and Genentech. DE has received personal fees from Alimera Sciences, Allergan, Clearside, EyePoint, Genentech, Gyroscope, Kodiak, Network Eye, Notal Vision, Novartis and Regeneron, received research support from Alimera Sciences, Allergan, Chengdu, Clearside, DORC, Genentech, Gyroscope, Kodiak NGM, Mylan, Network Eye, Novartis, Ophthotech, Ophthea and Recens Medical and received equity from Boston Image Reading Center, Hemera Biopharmaceuticals and US Retina. NMH has received research support from Gemini, Gyroscope, Roche and Genentech, received consultant fees from Acucela, Alimera Sciences, Allegro, Allergan, Clearside, Genentech, Katalyst, Lineage Cell Therapeutics, Notal Vision, Novartis, Regeneron, and Spark, and has patents and stock ownership with Katalyst. SK and EW are employees of Alimera Sciences.
Patient consent for publication Not required.
Ethics approval Sterling IRB (ID 5020). The study was conducted in compliance with the Pharmaceutical and Medical Device Act and Good Clinical Practice, and in accordance with the Declaration of Helsinki, following approval by the Institutional Review Board of the clinical study protocol and other documents, as well as of the appropriateness of conducting the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All deidentified participant data relevant to the study are included in the article or supplementary information.
Linked Articles
- At a glance