Article Text

Abstract
Aims To determine myopia progression in children who continued to wear the defocus incorporated multiple segments (DIMS) lenses or switched from single vision (SV) to DIMS lenses for a 1-year period following a 2-year myopia control trial.
Methods 128 children participated in this study. The children who had worn DIMS lenses continued to wear DIMS lenses (DIMS group), and children who had worn SV lenses switched to wear DIMS lenses (Control-to-DIMS group). Cycloplegic spherical equivalent refraction (SER) and axial length (AL) were measured at 6-month interval. Historical controls were age matched to the DIMS group at 24 months and used for comparing the third-year changes.
Results Over 3 years, SER and AL changes in the DIMS group (n=65) were −0.52±0.69D and 0.31±0.26 mm; these changes were not statistically significant over time (repeated measures analysis of variance, p>0.05).
SER (−0.04±0. 38D) and AL (0.08±0.12 mm) changes in the Control-to-DIMS group (n=55) in the third year were less compared with the first (mean difference=0.45 ± 0.30D, 0.21±0.11 mm, p<0.001) and second (0.34±0.30D, 0.12±0.10 mm, p<0.001) years.
Changes in SER and AL in both groups over that period were significantly less than in the historical control group (DIMS vs historical control: mean difference=−0.18±0.42D, p=0.012; 0.08±0.15 mm, p=0.001; Control-to-DIMS versus historical control: adjusted mean differences=−0.30±0.42D, p<0.001; 0.12±0.16 mm, p<0.001).
Conclusions Myopia control effect was sustained in the third year in children who had used the DIMS spectacles in the previous 2 years and was also shown in the children switching from SV to DIMS lenses.
- clinical trial
- child health (paediatrics)
Data availability statement
Data are available on reasonable request. The primary and secondary outcomes and the baseline demography of the participants in the 2-year RCT and the third year study can be made available. Please contact CSYL at carly.lam@polyu.edu.hk.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The prevalence of myopia is growing alarmingly worldwide, especially in East Asian populations.1–3 High myopia is associated with an increased risk of sight-threatening eye disease4–6 creating a long-term burden on economies and public healthcare.7 8 There is no doubt that myopia is a significant public health issue and a global concern.8 Effective interventions for myopia management and reduction would alleviate this problem.
Currently, a variety of modalities are used for myopia control in children.9–11 High-dose (1%) atropine eye-drops seem the most effective in myopia control, but the associated side effects, such as photophobia and blurred near vision, hinder its wide clinical application.12 In recent years, some studies have reported that low-dose (0.01%) atropine treatment has yielded positive results with minimal side effects and low myopic rebound.13–15 Optical treatments, including orthokeratology,16–18 executive top bifocal spectacles19 and multifocal soft contact lenses incorporating myopic defocus20–24 have also shown promising results in slowing myopia progression. However, each method has limitations.11
The defocus incorporated multiple segments (DIMS) spectacle lens is designed to control myopia in children, based on the principle of myopic defocus and simultaneous vision. It is a dual-focus spectacle lens consisting of a central optical zone for correcting distance refractive error, and a batch of tiny circular segments with a relative positive power of 3.50D equally distributed throughout the mid-peripheral area in a honeycomb pattern.25 Thus, the DIMS lens imposes myopic defocus while providing clear vision for the wearer simultaneously at all viewing distances. A 2-year double-masked randomised controlled trial (RCT) (ClinicalTrials.gov: NCT02206217) showed that DIMS lens wear slowed childhood adjusted myopia progression significantly by 52% and axial elongation by 62% compared with regular single vision (SV) spectacle lenses wear over 2 years.25
Our aims here are to determine (1) if myopia retardation (as measured by changes in spherical equivalent refraction (SER) and AL) continues in the third year of DIMS wear and (2) if myopia retardation is exhibited in the first year of DIMS wear by the original SV control group; both groups will be compared with a new historical control group.
Materials and methods
Study participants
Ethnic Chinese children who had completed the 2-year RCT25 (NCT02206217, between August 2014 and July 2017) were invited to participate in this third-year follow-up study. Written assent and informed consent were obtained from the children and their parents respectively before participation.
Children who had worn DIMS lenses in the RCT continued to wear DIMS lenses in the third year (DIMS group). The children in the original control group were offered the DIMS treatment and this gave us the opportunity to evaluate if the DIMS lenses could provide myopia control in the Control-to-DIMS group similar to that observed in the original DIMS group.
Study procedures and data collection
The primary and secondary outcomes were the changes in SER and axial length (AL). The procedures of data measurement followed those in the trial of DIMS lenses.25 SER and AL were measured at 6-month intervals. SER was measured by cycloplegic autorefraction using an open-field autorefractor (Shin-Nippon NVision-K5001, Ajinomoto Trading Inc.). AL was measured by partial coherence interferometry using an IOL Master (Carl Zeiss Meditec). Cycloplegia was induced by instillation of one drop of alcaine 0.5%, followed by one to two drops of cyclopentolate HCL 1%. The measurements were taken 30 min after the instillation of eye drops, and cycloplegia was considered achieved when the amplitude of accommodation was less than 2.00D as measured using an RAF rule. An average of five autorefractions and AL measurements for each eye was used for data analysis.
The historical control group
Since the children originally in the control group switched to wear DIMS lenses in the third year, they could not be used as the ‘control’ to assess effectiveness on myopia control. Therefore, we obtained a historical control group by reviewing clinical records from the Optometry Clinic, PolyU for 2017–2019. The criteria for selection were based on the inclusion and exclusion criteria in the original RCT. Subjects were healthy myopic ethnic Chinese children who attended eye examinations in the clinic with at least 12-month follow-up data. They had not received any myopia interventions and were matched for age (between 10 and 15 years) and SER ranges (−1.00 to −5.50D) with the DIMS subjects at the end of the 2-year RCT. Annual myopia progression and AL changes in this group of children were calculated and compared with the third-year changes in the DIMS and Control-to-DIMS groups.
Statistical analysis
All statistical analyses were performed using SPSS V.20.0. Baseline characteristics and the changes in SER and AL are presented as mean±SD. The right eye data only were used for analysis as there was no statistically significant difference between the left and the right eye data.
Following Kolmogorov-Smirnov tests for distribution, unpaired t-tests, Mann-Whitney U tests or repeated measures analysis of variance (ANOVA) tests were used as appropriate. Pearson’s correlation coefficient analyses were used to determine relationships between continuous variables and χ2 tests for categorical data.
For both the DIMS group and Control-to-DIMS group, myopia progression and changes in AL in years 1, 2 and 3 were calculated and compared by repeated measures ANOVA and post hoc pairwise comparisons using Bonferroni corrections were performed for determining where the differences laid. Myopia progression and change in AL were calculated for the historical control group, for which we had one (12 months) set of data, and were compared with the third-year changes of two experimental groups by multiple linear regression approach with adjusting confounding covariates, such as age, sex, SER and AL.
Results
Subject profile and baseline data
Figure 1 shows the number of subjects recruited and those lost to follow-up over 3 years. One hundred and sixty Chinese children completed the 2-year RCT and 128 of these agreed to participate in the third-year study. We compared the data between the subjects who joined and those who declined to join the third-year study for both the DIMS and Control-to-DIMS groups. No significant differences were found in terms of their age, gender, baseline myopia or AL, myopia progression or axial elongation in the previous 2-year trial (p>0.05) (online supplemental eTable 1).
Supplemental material

Subject numbers over 3 years. DIMS, defocus incorporated multiple segments; SV, single vision.
At the end of the third year, 120 children (DIMS, n=65; Control-to-DIMS, n=55) completed the data collection. The mean age at enrolment (mean±SD) was 10.15±1.52 years and 10.24±1.42 years in the DIMS and the Control-to-DIMS groups, respectively. The baseline SER of the DIMS group and the Control-to-DIMS were −2.98±0.96D and −2.73±0.99D, respectively. The baseline AL of the DIMS and the Control-to-DIMS were 24.68±0.82 mm and 24.57±0.88 mm. There were no statistically significant differences between the two groups with respect to age at enrolment, gender proportion, baseline myopia or baseline AL (p>0.05).
Changes in SER and AL
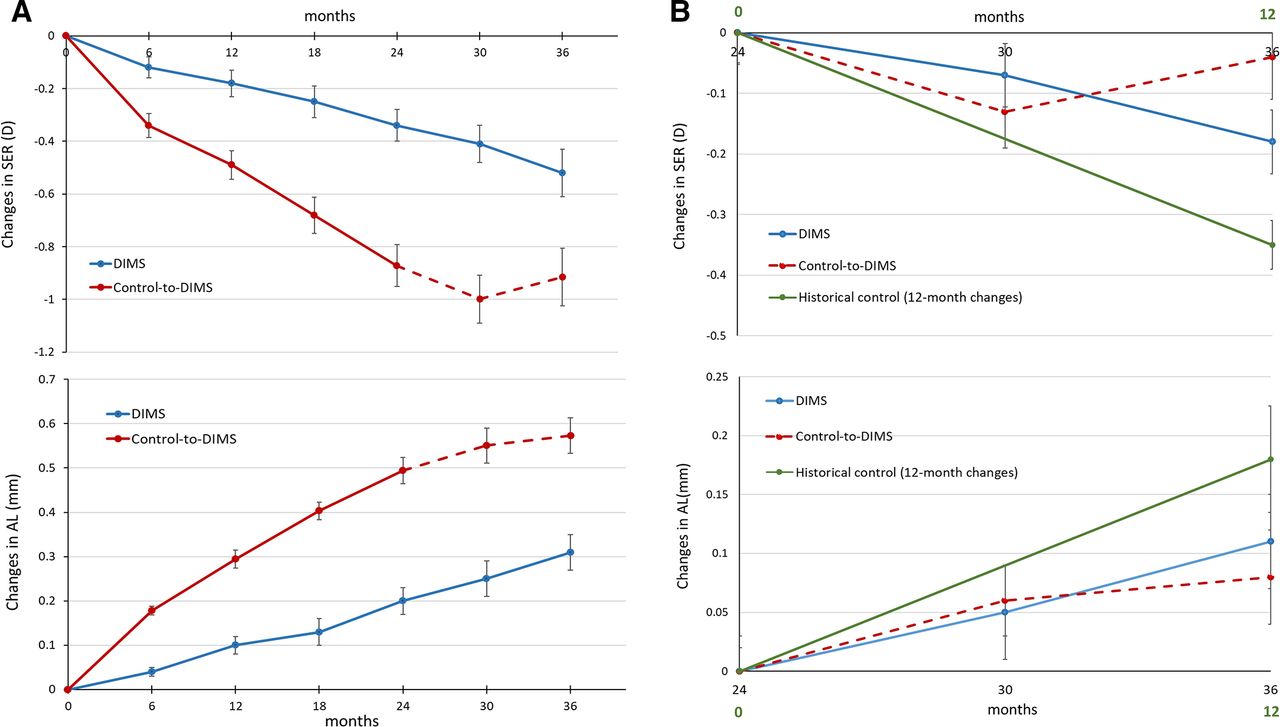
Figure 2A and table 1 present the mean and cumulative changes in mean SER and AL from baseline to 36 months in both groups. Figure 2B shows the trend in changes in SER and AL changes in the third year.

(A) Changes in spherical equivalent refraction (SER) and axial length (AL) from baseline to 36 months. The red dotted line represents the period (24–36 months) during which the previous single vision control group wore defocus incorporated multiple segments (DIMS) lenses. (B) The third-year changes in SER and AL in the DIMS and Control-to-DIMS groups. The green line shows the 12-month changes in SER and AL in the historical control group.
Mean and cumulative changes in the cycloplegic SER and AL from baseline to 36 months in the DIMS group and Control-to-DIMS group
The DIMS group
The mean changes in SER and AL in the DIMS group (n=65) were −0.52± 0.69D and 0.31± 0.26 mm over 3 years (table 1). The myopia progression and axial elongation did not change significantly over time (repeated measures ANOVA, p>0.05). The mean annual changes in SER and AL in the DIMS group were −0.18± 0.25D and 0.10± 0.09 mm over 3 years.
The Control-to-DIMS group
In the Control-to-DIMS group (n=55), myopia progression and axial elongation were significantly different between the 3 years (repeated measures ANOVA, p<0.001). Post hoc analyses indicated that their myopia progression and axial elongation in the third year were significantly decreased compared with the first (mean difference=0.45±0.30D, 0.21±0.11 mm, p<0.001) and second years (mean difference=0.34±0.30D, 0.12± 0.10 mm, p<0.001) (figure 2A).
DIMS compared with Control-to-DIMS in SER and AL changes
There were no statistically significant differences in myopia progression and axial elongation in the third year between the Control-to-DIMS group and the DIMS group ((p>0.05) (figure 2B).
The myopia of 80% of the subjects in the DIMS group progressed by less than 0.5D in the third year, compared with 87% in the Control-to-DIMS group. Only 5% and 2% in the DIMS and Control-to-DIMS groups, respectively, had myopia progression more than 1D. 52% and 58% in the DIMS and Control-to-DIMS groups had axial elongation less than 0.1 mm (figure 3).

{kind=link}
{kind=link}
{kind=link}
Distributions of myopia progression and axial elongation in the third year. DIMS, defocus incorporated multiple segments.
DIMS compared with the historical control group in SER and AL changes
The historical control group (n=76, 39 males and 37 females) had a mean age of 12.19±0.71 years, baseline SER and AL were −2.93± 1.33D and 24.77± 0.91 mm. Baseline characteristics of the historical control group did not differ statistically significantly from those of DIMS groups at 24 months (p>0.05) (online supplemental eTable 2).
The 12-month changes in SER and AL in the historical control group were −0.35± 0.40D and 0.18± 0.14 mm. The myopia progression in the DIMS group in the third year was significantly less than in the historical control group (mean difference=−0.18±0.42D, p=0.012). Axial elongation in the DIMS group was also less than in the historical control group (mean differences=0.08±0.15 mm, p=0.001).
Control-to-DIMS compared with the historical control group in SER and AL changes
There were no significant differences between the baseline data of the historical control group and the 24-month data in the Control-to-DIMS group, in terms of age, sex or AL, however, SER was significantly less in the historical control group than in the Control-to-DIMS group (p=0.003), the historical control group having been matched to the DIMS group (online supplemental eTable 3).
The children in the Control-to-DIMS group switched to wear DIMS spectacles in the third year. After adjusting for baseline SER, their myopia progression over that period was significantly slower than in the historical control group (mean differences=−0.30±0.42D, p<0.001). A similar result was found in the AL changes after controlling the cofounding factor (mean differences=0.12±0.16 mm, p<0.001).
Discussion
Myopia progression and axial elongation were less in the subjects wearing DIMS lenses throughout the 3 years, first compared with the initial control group (which subsequently became the Control-to-DIMS group), and then in the last 12 months compared with the historical control group. In the DIMS group, myopia progression and axial elongation in the third year were similar to those in the first and second years (figure 2A—blue line).
Overall myopia progression
The mean changes in SER and AL in the DIMS treatment group over the 3-year period were −0.52±0.69D and 0.31±0.26 mm. These findings are comparable with the corresponding findings in the 3-year trial with dual power contact lenses by Chamberlain et al 24 (-0.51±0.64D and 0.30±0.27 mm) and the 3-year trial with multifocal soft contact lenses by Walline et al 26 (-0.60D, range −0.72 to −0.47D and 0.39 mm, range 0.32–0.46 mm). Our progression findings were nearly 50% less than reported by Cheng et al 19 in a 3-year trial with bifocal and prismatic bifocal spectacle lenses which included subjects with fast myopia progression (−1.25±0.10D for the bifocal treatment group, and −1.01±0.13D for the prismatic bifocal treatment group).
Myopia retardation in DIMS and Control-to-DIMS groups
The mean changes in SER and AL in the DIMS group were −0.18±0.37D and 0.10±0.14 mm in the first year and, −0.17±0.31D and 0.10±0.11 mm in the second year. In the first 2 years, myopia progression and axial elongation in the DIMS group were retarded by 0.53D and 0.29 mm compared with the original control group.
The mean annual SER and AL changes in the historical control group aged from 10 to 15 years were −0.35D and 0.18 mm; when compared with the DIMS group’s third year changes in SER and AL, myopia progression and axial elongation in the DIMS group were retarded by 0.18D and 0.08 mm, respectively (figure 2B). The overall 3 years control effect in the DIMS group would be myopia retardation by 0.71D and AL decrease by 0.37 mm.
Cheng et al 19 reported that in a selected group of fast progressing myopic children wearing executive top bifocal spectacles with and without prisms, lowered myopia progression by 0.81D and 1.05D compared with SV spectacle lenses wearing children. Chamberlain et al 24 showed that a dual power soft contact lens significantly slowed myopia progression by 0.73D in children of various ethnicity aged 8–12 years. Walline et al reported in their BLINK clinical trial that children wearing high add power (+2.50D) multifocal contact lenses had 0.46D less myopia progression over 3 years.26 The reduction of myopia progression by the wearing of DIMS lenses is comparable to the findings from these studies using bifocals, dual focus and multifocal soft contact lenses.
The subjects in the Control-to-DIMS group showed significant reductions in myopia progression and axial elongation after switching from SV to DIMS lenses wear (figure 2B). Their changes in SER and AL in the third year were comparable to the first-year changes in the DIMS group, even though these subjects were 2 years older. In comparison to the historical control group, their myopia progression and axial elongation in the third year, after adjustment were reduced by 86% and 61%, respectively.
In the third year, more than 80% of the Control-to-DIMS children had myopia progression less than 0.5D, and approximately 70% showed progression less than 0.25D. All these findings suggested that the myopia control effect was achieved even though the subjects started to wear DIMS lenses at an older age.
Limitations
A limitation of this study was that the cohort used in the analyses comprised the DIMS plus the Control-to-DIMS groups of children so that the study was no longer randomised. This follow-up study, however, did benefit from the comparison of the third-year myopia progression findings in the DIMS group with the Control-to-DIMS group. While there were no statistically significant differences between the DIMS group and the historical control group at the start of the third year, there was a statistically significant difference in SER between the historical control group and the Control-to-DIMS group at baseline. This was because the historical control group was matched with the DIMS group at 24 months for age and SER and as the Control-to-DIMS group had no treatment in the first 2 years it could be expected to have more myopic SER. Although adjustment was made in the comparison, this approach does not eliminate the effect that can result from known or unknown factors, such as different examiners, the number of myopic parents and time spent on near and outdoor activities, and potentially could lead to selection bias for estimating the treatment efficacy of the DIMS lens.
Conclusions
The DIMS spectacle lens slowed myopia progression and axial elongation in children throughout the 3 years of study and the myopia control effect was also demonstrated in the Control-to-DIMS group. These findings provided further evidence that DIMS lenses slowed myopia progression and axial elongation in children. The optimal age at which treatment should commence is still to be determined and further monitoring is required to ascertain the treatment effect over a longer period. We also plan to follow up on those children who discontinued wearing the DIMS lenses to determine if rebound occurs.
Data availability statement
Data are available on reasonable request. The primary and secondary outcomes and the baseline demography of the participants in the 2-year RCT and the third year study can be made available. Please contact CSYL at carly.lam@polyu.edu.hk.
Ethics statements
Patient consent for publication
Ethics approval
The study obtained the human ethical approval from the Departmental Research Committee of the School of Optometry, The Hong Kong Polytechnic University. The reference number is HSEAR20140630003-03. All aspects of the study met the tenets of the Declaration of Helsinki and were approved by the Human Subjects Ethics Subcommittee of the Hong Kong Polytechnic University (PolyU).
Acknowledgments
HOYA provided the frames and lenses for the study. We are grateful for advice from Professor Marion Edwards. We would like to thank the employees of Hoya for assisting the ordering and manufacturing of the lenses and Ms Yee Mui Kwok for liaison with the parents.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Writing—Original Draft: CSYL, WCT; Writing—Review and Editing: CSYL, WCT, PHL; Conceptualisation: CHT, CSYL, HQ; Project administration: CSYL, CHT, KH; Investigation: WCT, HYZ; Methodology: CSYL, CHT, WCT; Visualisation: CSYL, CHT, WCT. All the authors listed have been involved in the undertaking of the clinical trial and follow up study including the conception of the lens design, fabrication of the lens, registration of the clinical trial, preparation of clinical protocol, data collection and analysis, interpretation of the findings and conclusions. A number of manuscripts are now in preparation by the author team.
Funding This was a collaborative research project supported by HOYA, Tokyo, Japan (PolyU grant numbers ZG5N), other PolyU grants: ZVN1, ZVN2, ZE1A, 8-8475, and by an RGC Research Impact Fund: R5032-18. The sponsor also provided specially manufactured spectacle lenses and frames.
Competing interests This collaborative research was supported by HOYA Corporation, Tokyo, Japan. Patents titled ‘Spectacle Lens’ in China (CN104678572 B) and USA (US10268050 B2) were issued on 27 April 2018 and 23 April 2019 respectively.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- At a glance