Article Text

Statistics from Altmetric.com
Intraocular pressure (IOP) is dependent on the rate of aqueous production, facility of outflow, and episcleral venous pressure. Increased IOP and visual field loss may result from an elevation of episcleral venous pressure, the causes of which include large vessel venous obstruction (venous sinus thrombosis and superior vena cava syndrome), arteriovenous shunts or fistulas, Sturge-Weber syndrome, scleritis, thyroid related orbitopathy, and orbital tumours.1 Increased episcleral venous pressure may result in elevated IOP and optic neuropathy, even in the absence of these entities. We report a 34 year old man with idiopathic dilated episcleral veins (IDEV) and increased IOP, with visual field loss.
CASE REPORT
A 34 year old man presented for neuro-ophthalmic evaluation because of decreased vision in the right eye and injection of both eyes. His intraocular pressure (IOP) had been elevated in the right eye more than the left for the past 13 years, reaching 32 mm Hg in the right eye. His eyes appeared red for as long as he could remember, but details of his previous ophthalmic examinations were unavailable. Because of the bilateral injection he saw two other neuro-ophthalmologists, who suspected an arteriovenous fistula. One year before presentation he underwent magnetic resonance imaging (MRI) of the head and orbits and catheter arteriography on two occasions, which were both normal. He had no other previous medical problems, was taking no drugs, and had no recent history of trauma to the head or neck.
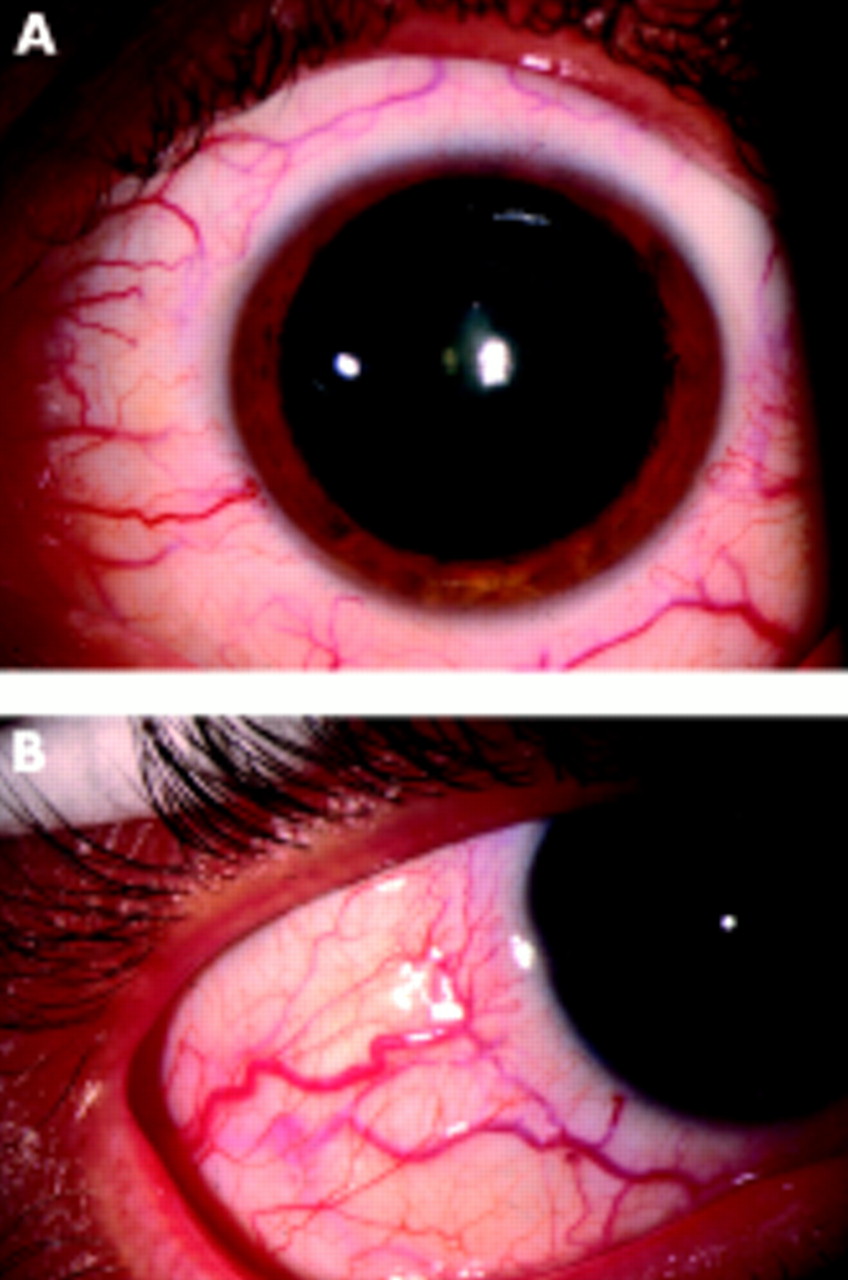
External examination revealed no evidence of cutaneous angiomatosis. Best corrected visual acuity was 20/25 in the right eye and 20/20 in the left eye. Although he correctly identified eight of eight Ishihara pseudoisochromatic colour plates with each eye, he had a 35% subjective red desaturation on the right, with a right relative afferent pupillary defect (RAPD). There was no exophthalmos and no increased resistance to retropulsion of the globes into the orbits. Dilated episcleral veins were apparent in each eye (Fig 1), while the conjunctival vessels were normal. Intraocular pressure was 22 mm Hg on the right and 16 mm Hg on the left, and the mires of the Goldmann applanation tonometer were normally pulsatile. Gonioscopy revealed bilaterally open iridocorneal angles to the ciliary body band for 360 degrees with blood in the canals of Schlemm in both eyes, greatest within the inferior 90 degrees, but without evidence of neovascularisation or angle recession. Automated perimetry revealed a nasal step on the right and decreased sensitivity inferiorly on the left. Asymmetric cupping of the optic disc, with vertical elongation on the right, was noted on funduscopy (Fig 2).

External examination shows dilated episcleral veins of each eye. (A) Right eye, (B) left eye.

The left optic disc (A) is normal and the right optic disc (B) shows a vertically elongated cup. The retinal vessels are of normal calibre.
Orbital colour Doppler imaging revealed normal flow parameters in the ophthalmic and central retinal arteries of each eye. The superior ophthalmic vein was of normal calibre and there was no evidence of reversal of flow in either orbit (Fig 3).

{kind=link}
{kind=link}
{kind=link}
Orbital colour Doppler imaging shows a normal calibre of the superior ophthalmic veins in the right (A) and left (B) orbits. The blue colour represents normal retrograde flow of the orbital veins.
COMMENT
Arteriovenous fistula is the most frequent cause of ocular injection with increased IOP due to elevated episcleral venous pressure.1–3 The ocular injection results from engorged, arterialised conjunctival vessels,4,5 which is different from the injection seen in IDEV. Traumatic high flow fistulas may present with proptosis, eyelid oedema, and conjunctival chemosis, and are often easily identified clinically. Spontaneous, frequently low flow fistulas may present with progressive unilateral or bilateral injection, and may be more difficult to diagnose.
There is, however, an infrequent syndrome of ocular injection and increased IOP which is idiopathic. Although originally described by Minas and Podos,6 the same entity is termed the Radius-Maumenee syndrome7 in the German literature.1,8,9 In one report 10 of 64 patients with glaucoma due to elevated episcleral venous pressure had this syndrome.1 In another report of six patients with unilateral dilated episcleral veins and one patient with bilateral involvement, the IOP in the affected eyes ranged between 21 and 44 mm Hg.10 In all six patients with apparently unilateral involvement the IOP was higher in the eye with the dilated vessels. Episcleral venous pressure was measured to be twice the normal value in the affected eyes of these patients.
Catheter arteriography in these patients is normal, without abnormal arteriovenous communications.10,11 Other adjunctive testing, including neuroimaging, orbital venography, and fluorescein angiography are also normal.9 Although abnormalities in ocular blood flow have been suggested, the pathogenesis of this condition remains unclear.
Orbital colour Doppler imaging provides a non-invasive means of imaging orbital and ocular blood flow and, in patients with fistulas, characteristically shows reversal of blood flow in a dilated superior ophthalmic vein.12 The superior ophthalmic veins were of normal calibre in our patient, and both orbits showed normal retrograde flow in the orbital veins. Similar findings were reported in the only other patient with this syndrome who underwent orbital colour Doppler imaging, and increased arterial and venous flow in the episcleral vessels was noted in the eye with dilated episcleral vessels; however, the images of the ultrasonography were not published.11 We did not measure the episcleral blood flow in our patient.
Although the cause of this disorder remains elusive it should be distinguished from other disorders, most commonly the arteriovenous fistula (Table 1), which can result in dilated episcleral vessels and increased IOP. In patients with IDEV a congenital abnormality in vasculature and familial predisposition have been suggested as the cause7; however some reports suggest that the ocular injection is acquired.10
Differentiating features of arteriovenous fistula and IDEV and increased IOP
Treatments have focused on reducing IOP with aqueous suppression. Filtration surgery has been favoured by some, and in one patient who underwent trabeculectomy the IOP was reduced but the dilated episcleral veins remained unchanged.11 Presumably an alteration in aqueous outflow would preclude the use of IOP lowering agents which increase uveoscleral outflow; however, the earlier reports of IDEV preceded the availability of these agents.
Although no clear aetiology has been identified for IDEV, the findings in this syndrome have been characterised well enough to obviate the need for catheter angiography in patients with the clinical features of this syndrome who have normal orbital colour Doppler imaging, and to avoid delaying the treatment of elevated IOP.
Acknowledgments
Dr Foroozan is supported by the Heed Ophthalmic Foundation, Cleveland, Ohio, USA. The authors have no proprietary interest in any contents within this manuscript.