Article Text

Abstract
Background: Bimanual, three-dimensional robotic surgery has proved valuable for a variety of surgical procedures.
Aims: To examine the use of a commercially available surgical robot for ocular microsurgery.
Methods: Using a da Vinci surgical robot, ocular microsurgery was performed with repair of a corneal laceration in a porcine model. The experiments were performed on harvested porcine eyes placed in an anatomical position using a foam head on a standard operating room table. A video scope and two, 360°-rotating, 8-mm, wrested-end effector instruments were placed over the eye with three robotic arms. The surgeon performed the actual procedures while positioned at a robotic system console that was located across the operating room suite. Each surgeon placed three 10-0 sutures, and this was documented with still and video photography.
Results: Ocular microsurgery was successfully performed using the da Vinci surgical robot. The robotic system provided excellent visualisation, as well as controlled and delicate placement of the sutures at the corneal level.
Conclusions: Robotic ocular microsurgery is technically feasible in the porcine model and warrants consideration for evaluation in controlled human trials to deploy functioning remote surgical centres in areas without access to state-of-the-art surgical skill and technology.
- 10-0 MFN, 10-0 microfilament nylon
Statistics from Altmetric.com
Classic microsurgery of the eye is performed using an operating microscope. The structures of the eye anterior to the vitreous are operated on under direct vision, whereas posterior regions such as the retina and vitreous are operated on using specialised lens and viewing systems. Robotic surgery is a potential mode of ocular microsurgery that has not yet been reported.
Newer surgical robots have transcended the role of assistant to become the primary surgeon through a computer interface.1 The da Vinci Surgical System (Intuitive Surgical, Sunnyvale, California, USA) incorporates three-dimensional stereoscopic vision with three robotic slave arms that can be equipped with instruments and have 7 degrees of freedom and wrist-like motions.
Many surgical specialties are exploring the uses of robotic surgery. Cardiac surgeons,2 urologists3 and general surgeons have used it for minimally invasive surgery.4,5 Recently, surgeons have also used the robot for thoracic, eye, nose and throat, and plastic surgery.6,7 Robotic surgery has proved especially useful for surgical procedures that take place in tight anatomical confines.
The unique attributes of the da Vinci robot, which is suitable for minimally invasive surgery, make it an attractive option for performing ocular microsurgery, a discipline that demands optimal visualisation, minimisation of tremor, technical skill and precise surgical manipulations. The operating microscope has remained the preferred standard in ophthalmic centres throughout the world.
Using a porcine model, we established the application of robotic surgery on the eye using suturing of corneal lacerations with the da Vinci robot.
MATERIAL AND METHODS
The protocol was approved by the institutional review board, the Institutional Animal Care and Use Committee, UCLA.
We used five porcine eyes. The first step in the surgical procedure was a manual injection of saline into the vitreous cavity of the eye. The procedure was designed to maintain ocular volume and ocular tonus to mimic the dynamics of the eye in vivo. A horizontal corneal laceration 8 mm in length was made with a 2.7-mm keratome across the apex of the cornea in each eye to mimic a corneal laceration to a depth of 90% of the corneal thickness.
Each surgeon (AT, CM and ED) performed surgical closure of the laceration with three separate interrupted sutures using 10-0 microfilament nylon (10-0 MFN). The operating time for the closure was measured using a digital timer. All times were rounded up to the nearest second. The surgeons performing ocular microsurgery (AT and CM) then placed three sutures each across the corneal laceration of the two remaining eyes using standard ophthalmic instruments and an ocular microscope. These procedures were also timed and documented with still and video photography.
Ocular microsurgery technique
The prepared globe was placed in a human manikin head in the anatomical position and the operating room table was rotated 90° relative to the robotic cart. Visualisation of the eye was achieved with a 0°, upward-facing, three-dimensional endoscope placed above the globe in the mid-line, mimicking the axis of standard ocular surgery using the operating microscope. The arm ports for the 8-mm robotic instrumentation were placed on either side of the globe at about 45° angles from the axis created by the mid-line position of the endoscope. The surgeon was seated at the surgical console, about 15 feet from the surgical table and robotic cart. The surgeon viewed the operative field via a three-dimensional image while his hands held the master controls at a comfortable distance below the display. Each slave arm was equipped with sterile black diamond microforceps (Intuitive Surgical) (fig 1). In this study the first assistant were surgical loupes and cut the sutures.

Black diamond microforceps.
The forceps held the 10-0 MFN and the contralateral arm was used to manipulate the robotic Debakey forceps.
The procedure was performed in each globe by a different surgeon. One surgeon was an experienced robotic surgeon (ED) but had no experience with ocular surgery, whereas the other two surgeons (AT and CM) were ocular surgeons using the robot for the first time. The 8-mm instrumentation was used. Nine sutures were placed.
Once the trial using the porcine eyes was completed, a standard ophthalmic microscope and instrumentation were used to place sutures in the other two porcine eyes.
Robotic set-up
Figure 1 shows the black diamond forceps used. Figures 2 and 3 show the robotic set-up and control console.

The surgeon seated at the surgeon’s console with hands in the “masters” (master controls for the slave arms and camera).

Robot draped and positioned over the patient’s head and eye.
RESULTS
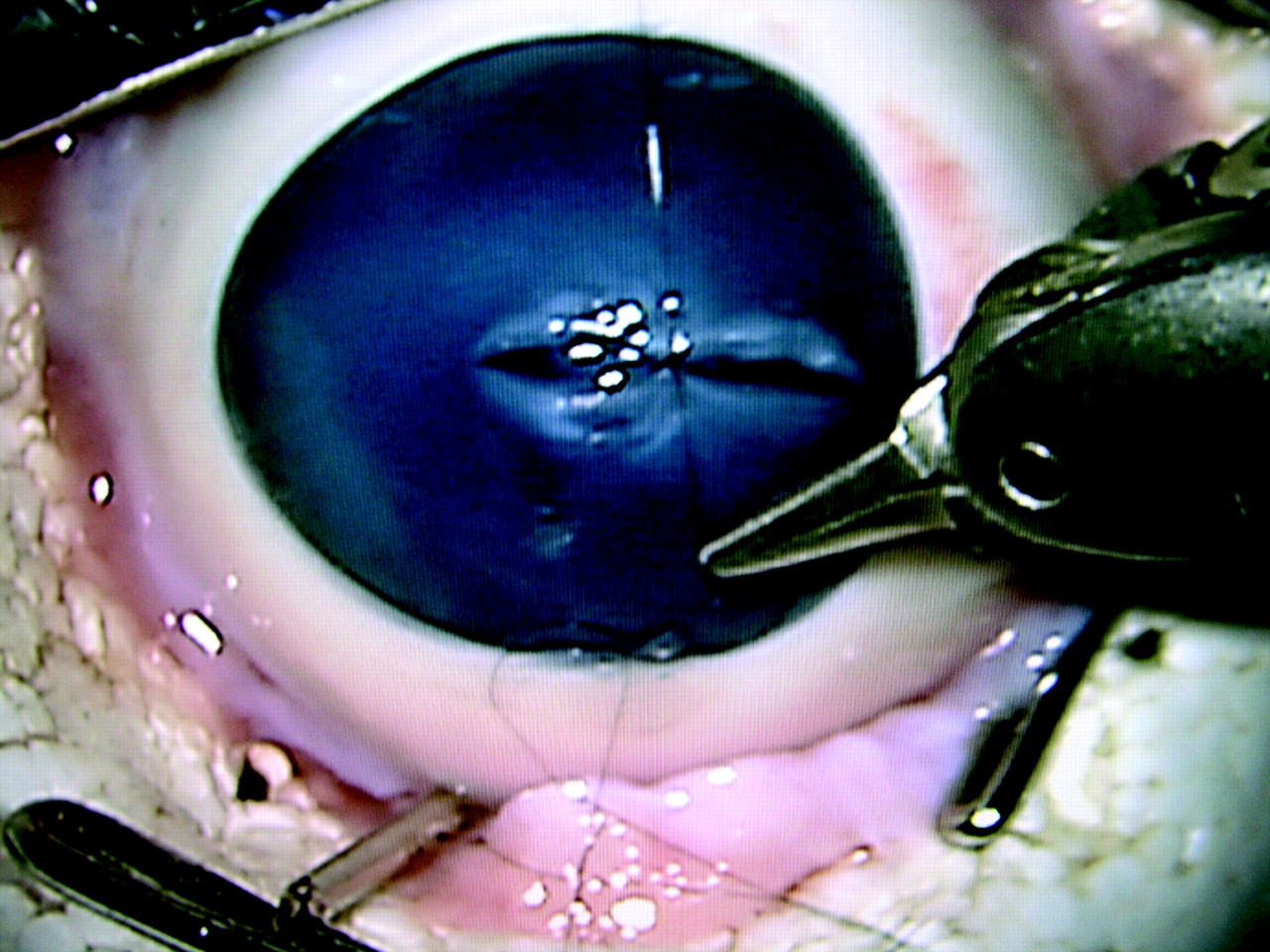
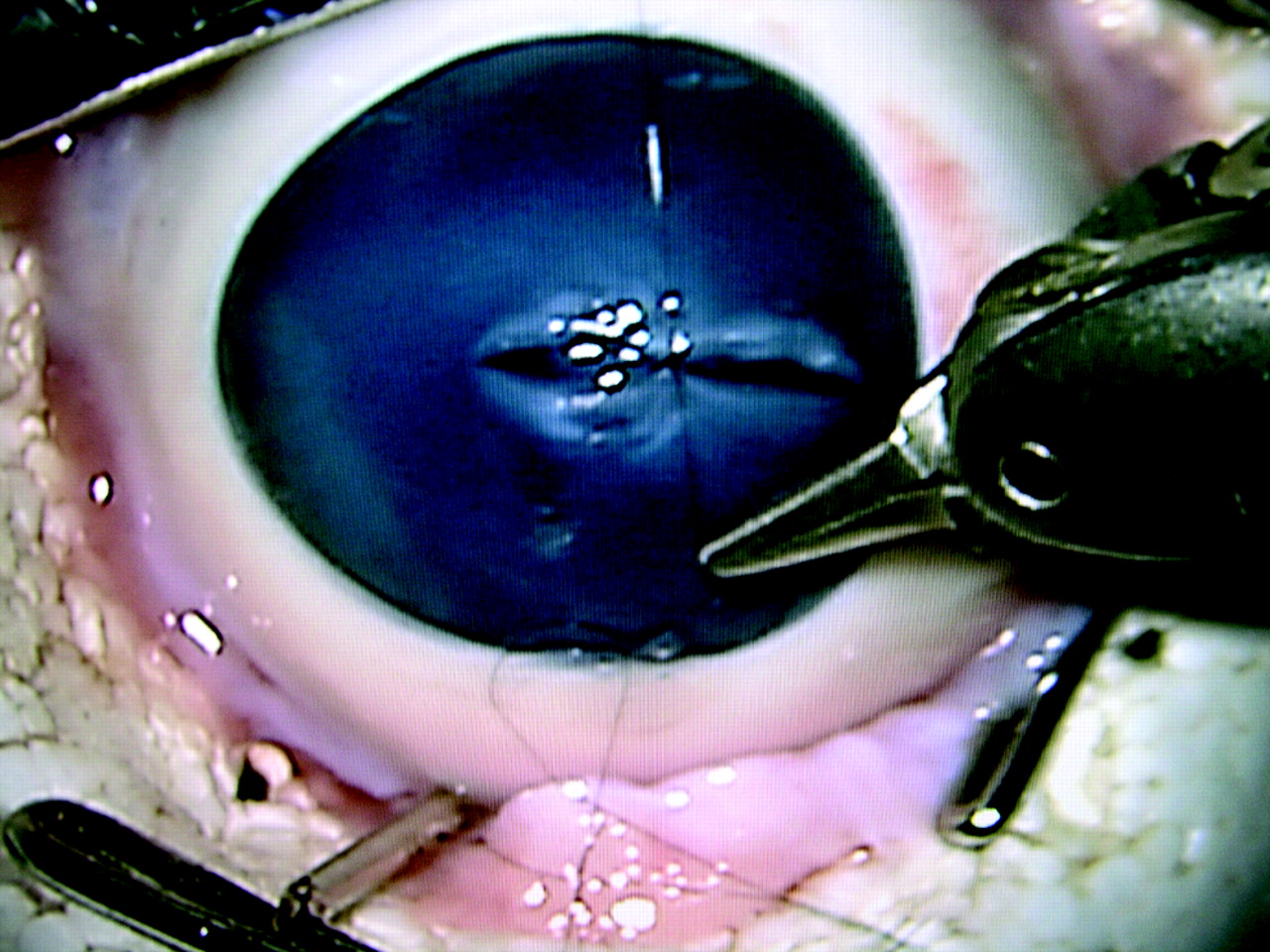
Figures 4–6 show the suturing technique.

Robotic microforceps grasping the wound as the suture is removed.

Robotic microforceps grasping the cornea and inserting the first suture.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Robotic tightening of the suture.
The ability to complete and tie the corneal suture was assessed by each surgeon and several variables were compared.
Operative time
The time taken to place the corneal sutures was compared with that taken to place the sutures using a conventional microscope. The durations for robotic surgery were 465, 655 and 750 s. The durations for suture placement with the operating microscope were 183 and 190 s. The average robotic surgical time for the placement of each 10-0 suture was 207 s versus 62 s with conventional microsurgery.
Postoperative evaluation of the eyes
Each eye was subjected to gross and microscopical evaluation of laceration closure and suture placement using a standard operative microscope.
Visualisation of operative field
The 0°, three-dimensional endoscope provided excellent depth perception for the surgeon and excellent lighting from the robotic endoscope. All key surgical landmarks including the depth of the suture placement were clearly and readily identifiable.
The robotic surgeon (ED) noted that the ultrafine scaling used on the robot provided a different feel to the surgery than standard scaling used for intra-abdominal surgery. It was also noted that finer surgical instrumentation would improve the control of suture placement. The use of the 5-mm effector arms would also facilitate finer movements. Currently, the microforceps are tailored towards placement of 7-0 sutures in cardiac surgery. A new instrument designed to act as a fine-toothed forceps would also help in everting wound edges and stabilising tissue for fine suture placement.
DISCUSSION
Robotic systems have been integrated into the surgical environment over the past 15 years. Probot, one of the first surgical robots, was developed by the Mechantronics in Medicine Laboratory at Imperial College London, UK, in the late 1980s. This system was designed to assist with transurethral resection of the prostate, and the first patient was treated in April 1991.1 This was the first time a robot was used to remove tissue from a patient.
One of the main advantages of robotic surgery is its ability to improve fine movement skills. Both the Zeus and the da Vinci systems have designs intended to compensate, at least partially, for many of the basic limitations of endoscopic surgery.8,9 Initially aimed at the minimally invasive cardiac surgery, both systems have found applications in gastrointestinal, gynaecological and urological surgery.8,9 By 2001, more than 40 Zeus and more than 50 da Vinci systems were being used in clinical practice worldwide.8 If we consider all computer-enhanced surgical systems, more than 2000 procedures have been performed between 1997 and 2001.9
Recently, Computer Motion (the manufacturer of the Zeus robotic system) has been acquired by its competitor, Intuitive Surgical. Intuitive Surgical has discontinued manufacture of the Zeus system. The only robotic system currently available is the da Vinci.
The feasibility of telesurgery was shown when Marescaux et al10 performed the first transatlantic robotically assisted remote laparoscopical cholecystectomy. Augmented reality systems exist that take modern imaging modalities and effectively give the surgeon “x ray vision”, allowing him to see through tissues to approach a target for biopsy or avoid a hazard.11 These applications for telesurgery would also have great appeal in ocular surgery. In this discipline, there is minimal chance of severe blood loss and hence a more controlled environment exists. The robotic surgery technique may also allow telementoring applications. This would also have advantages in ocular microsurgery that are mimicked in the general surgical field.
The potential use of robotic systems has expanded rapidly in all disciplines of surgery.12 Urologists have found applications for the robot in laparoscopical nephrectomy, pyeloplasty, adrenalectomy and radical prostatectomy.4 Laparoscopic gastrointestinal procedures that have been performed robotically include, but are not limited to, cholecystectomy, Nissen fundoplication, Heller myotomy, pancreatectomy, hepaticojejunostomy, gastric banding, distal gastrectomy, Roux-en-Y gastric bypass and colectomy.13–15
The use of robotic ocular surgery has not been previously explored. The benefits of improved ergonomics, motion scaling, tremor filtration and extensive instrument articulation are important in standard ocular surgery. The eye is a closed system and can be thought of as a miniature of the other surgical areas in which the robot is used, such as the abdomen and chest cavity. The issues of tactile feedback, which have been a concern with surgery in other areas, are not a drawback in ocular surgery, where visual feedback is used to gauge suture tightness or tissue manipulation. The intricate movements required in ocular surgery can be made with the robot, and problems with scaling and instrumentation are likely to be related only to finer engineering and variable computer programs for different anatomical areas and uses.
Integration of robotic assistance into the ocular arena has some major disadvantages.16,17 One major drawback is that the systems are expensive, usually costing >US$1 million. Also, the placement of sutures is much slower than with standard ophthalmic microsurgical instruments. It seemed, however, that the learning curve was fast and a lot of the issues were related to hardware. Technical innovations and surgical facility will undoubtedly improve with experience.
Ocular microsurgery is certainly possible and the da Vinci robot is able to execute the fine movements necessary for ocular surgery. The applications for robotic ocular surgery are extensive. Improved instrumentation and mastery of surgical skills using this novel modality will lead to further advances in cataract and vitreoretinal surgery. To this end, our laboratory is actively developing newer techniques and instruments for use in robotic intraocular surgery.
CONCLUSIONS
We report the first instance of robotic ocular microsurgery. The da Vinci surgical robot allowed for successful completion of the ocular microsurgery in the porcine model. Our findings support the use of a surgical robot for ocular surgery and establish a foundation for further investigation of the feasibility and applicability of robotic systems in controlled human trials.
REFERENCES
Footnotes
-
Competing interests: None.
-
Published Online First 4 October 2006
Linked Articles
- Editorial
- BJO at a glance