Article Text

Abstract
Aim: To evaluate the relationship between vision-related quality of life (VR-QOL) and visual function in patients undergoing vitrectomy, gas tamponade and cataract surgery for macular hole (MH).
Methods: The 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) was self-administered by 32 patients with MH (age 66.2 (SD 5.4) years) preoperatively and at 3 months postoperatively. Clinical data were collected, including logarithm of minimum angle of resolution (logMAR) best corrected visual acuity (BCVA), severity of metamorphopsia and letter contrast sensitivity. The severity of metamorphopsia was evaluated by the M-Charts. MH index was measured using optical coherence tomography. The presence and severity of cataract were graded using the Lens Opacities Classification System III reference standards. Multiple regression analysis was performed to investigate the relationship between various explanatory variables and VFQ-25 questionnaire scores. Explanatory variables tested were the severity of metamorphopsia, visual acuity, letter contrast sensitivity, MH index and grade of cataract.
Results: Vitrectomy for MH significantly improved VFQ-25 composite score as well as subscale scores, including general vision, near activities, distance activities, social functioning, mental health and dependency (p<0.05, Wilcoxon signed-rank test). Multiple regression analysis revealed that, both preoperatively and postoperatively, the severity of metamorphopsia had a significant correlation with VFQ-25 composite score (p<0.05), whereas other explanatory variables did not. In addition, changes in the severity of metamorphopsia was the single variable that was significantly related to changes in VFQ-25 composite score (p<0.01).
Conclusion: Vitrectomy for MH significantly improved VR-QOL. The severity of metamorphopsia was significantly associated with both preoperative and postoperative VR-QOL.
Statistics from Altmetric.com
Visual acuity improves in many patients after successful closure of macular hole (MH) by vitrectomy,1 2 whereas some patients still complain of remaining metamorphopsia after surgery. Metamorphopsia is one of the most common conditions that cause deterioration in visual functions in patients with macular diseases. Relatively little attention has been paid, however, to changes in visual functions, including metamorphopsia, caused by surgery and their relationship with vision-related quality of life (VR-QOL).
Recent studies using the 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) have reported that vitrectomy for MH appears to have a beneficial effect on patients’ subjective perception of quality of life.3 4 5 Tranos et al demonstrated that VFQ-25 score after MH surgery was significantly correlated with the severity of postoperative metamorphopsia.4 On the other hand, preoperative and surgery-induced changes in VFQ-25 composite score did not correlate with the preoperative severity of metamorphopsia or changes in the severity.4 They evaluated the severity of metamorphopsia using the Amsler chart, which has been widely used to detect and evaluate metamorphopsia in patients with macular diseases.6 7 With the Amsler chart, however, it is difficult to quantify the severity of metamorphopsia because the patients have to self-describe the degree of image distortion. Assessment with the M-Charts (Inami Co., Tokyo, Japan) can easily and quantitatively evaluate the degree of metamorphopsia associated with macular diseases, as the patients only have to state whether the line appears to be distorted or not.8 9 We conducted the current prospective study to evaluate the relationship between VR-QOL and visual function, including metamorphopsia, using the M-Charts in patients undergoing vitrectomy for MH.
Patients and methods
The current prospective, consecutive case series included 32 eyes of 32 patients with MH (13 men and 19 women) who underwent pars plana vitrectomy at Tsukuba University Hospital between June 2006 and February 2007. Patients with other ocular diseases, except for mild refractive error, were excluded. There were no significant ocular pathologies in the fellow eyes of the patients. Logarithm of minimum angle of resolution (logMAR) best corrected visual acuity (BCVA), the severity of metamorphopsia and letter contrast sensitivity were recorded preoperatively and at 3 months postoperatively.
The severity of metamorphopsia was evaluated by the M-Charts. The M-Charts consist of 19 dotted lines with dot intervals ranging from 0.2° to 2.0° of visual angle. If the straight line is substituted with a dotted line and the dot interval is changed from fine to coarse, the distortion of the line decreases with the increasing dot interval, until finally the dotted line appears straight.8 9
Letter contrast sensitivity was measured using the CSV-1000LV chart (Vector Vision, Columbus, Ohio, USA). Measurements with optical coherence tomography (OCT; Stratus OCT 3000, Carl Zeiss Ophthalmic Systems-Humphrey Division, Dublin, California, USA) were carried out preoperatively. Three MH parameters (MH base diameter, MH diameter and retinal thickness around the MH) were defined and the MH index (MHI) was calculated according to the methods of Kusuhara et al.10 For standardisation purposes, several OCT images were recorded on each occasion. The presence and severity of cataract were graded using the Lens Opacities Classification System III (LOCS III) reference standards.11
The patients were requested to answer VFQ-25 preoperatively and at 3 months postoperatively to assess VR-QOL.12 The research staff explained the questionnaire to the patients, and gave verbal instructions and provided assistance when required. The completed questionnaires were reviewed for missing data by the research staff. Prior to surgery, all missing data were added by the patients themselves. The VFQ-25 comprises 25 items wherein patients are expected to assess the level of difficulty of particular visual symptoms or day-to-day activities. Each item is assigned to one of the 12 subscales: general health, general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, colour vision and peripheral vision. The subscales are scored on a 0 to 100 point scale, where 100 indicates the highest possible function or the minimal subjective impairment. The VFQ-25 composite score is calculated as the unweighted average response to all items, excluding questions regarding general health. The VFQ-25 used in this study was a Japanese version, with modifications to suit the Japanese culture and way of life. The modified NEI VFQ-25 questionnaire has been assessed for reliability and validity, and it has been proven to accurately measure VR-QOL in Japanese individuals.13
Surgeries were performed by an experienced vitreoretinal surgeon (F O), using standard cataract surgery and pars plana vitrectomy with 20 gauge probes, peeling of the inner limiting membrane with subsequent instillation of a gas tamponade (20% sulphur hexafluoride; SF6) and postoperative instructions to lie face down for 1 week. Indocyanine green was used to peel the inner limiting membrane. Subjects were followed up for at least 3 months after surgery and any postoperative complications were documented.
Mean scores and standard deviations were calculated for VFQ-25 composite and subscale scores, visual acuity, severity of metamorphopsia, contrast sensitivity, MHI and LOCS III index. The significance of the differences between preoperative and postoperative values was assessed with the Wilcoxon signed-rank test. Preoperatively and postoperatively, multiple regression analysis was performed to investigate the relationship between various explanatory variables and VFQ-25 questionnaire scores. Variables tested were visual acuity, severity of metamorphopsia, letter contrast sensitivity, MHI and grade of cataract (LOCS III index). The relationship between changes in VFQ-25 composite score and changes in above-mentioned explanatory variables was also evaluated. All statistical tests were considered to be significant if p<0.05. Analyses were carried out using StatView (version 5.0; SAS Institute, Cary, North Carolina, USA). A prestudy power calculation using a significance level of 5% (α) and a power of 80% (1–β) revealed that a sample size of 27 eyes would be required to detect a mean VFQ-25 composite score difference of 6 points.
Results
Table 1 summarises the preoperative characteristics of patients. By the initial surgery, MH was successfully closed in all eyes. No significant intraoperative and postoperative complications were observed, such as retinal detachment, choroidal detachment, subretinal haemorrhage, cystoid macular oedema or infection. In six patients, intraocular pressure elevated to 25 mmHg or higher, but responded promptly to antihypertensive therapy.
Preoperative characteristics of patients with macular hole
All patients underwent MH surgery on their worse-seeing eyes. The surgery significantly improved the metamorphopsia score from 0.77 (SD 0.55) to 0.45 (SD 0.44) (p<0.005, Wilcoxon signed-rank test), logMAR BCVA from 0.76 (SD 0.47) to 0.48 (SD 0.35) (p<0.0001), and letter contrast sensitivity from 15.3 (SD 8.8) to 19.5 (SD 8.2) (p<0.005). Metamorphopsia was significantly improved by surgery, but did not resolve completely at 3 months after surgery.
The results of the pre- and postoperative VFQ-25 questionnaire are shown in table 2. Vitrectomy significantly improved VFQ-25 composite score (p<0.005), as well as subscales such as general vision (p<0.0005), near activities (p<0.001), distance activities (p<0.05), social functioning (p<0.01), mental health (p<0.05) and dependency (p<0.01).
The National Eye Institute 25-item Visual Function Questionnaire (VFQ-25) composite and 12 subscale scores in patients with macular hole
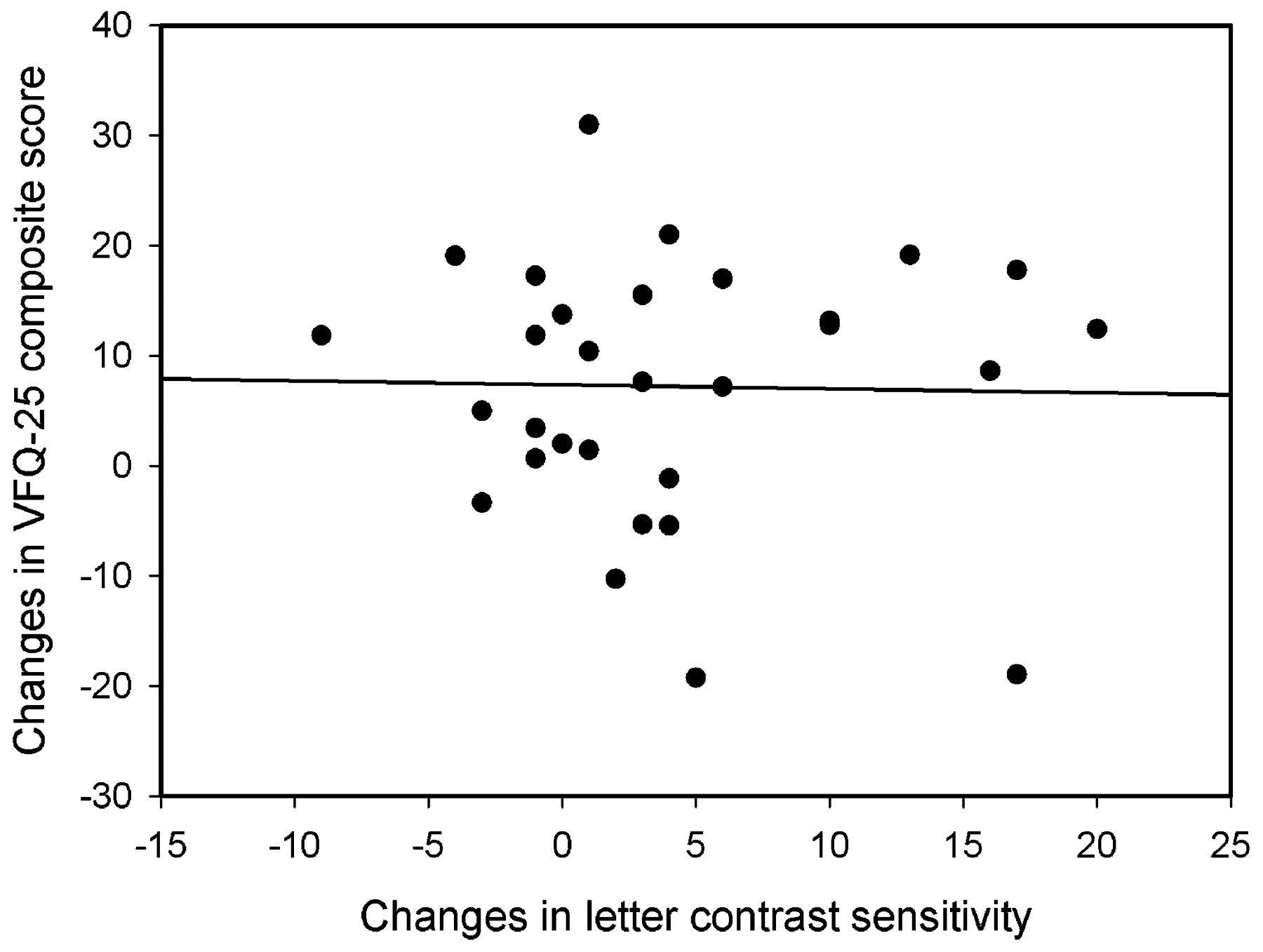
Table 3 summarises the results of multiple regression analysis on the relationship between VFQ-25 composite score and several explanatory variables, including visual function, MH morphology and grade of cataract. Both preoperatively and postoperatively, the severity of metamorphopsia exhibited significant positive correlation with VFQ-25 composite score (p<0.05), whereas other explanatory variables showed no relationship with VFQ-25 composite score. Similarly, changes in the severity of metamorphopsia were significantly associated with the changes in VFQ-25 composite score (p<0.01, fig 1), but changes in other variables were not, including logMAR BCVA (fig 2) and letter contrast sensitivity (fig 3).

Statistically significant correlation between changes in the severity of metamorphopsia and changes in the 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) composite score by vitrectomy for macular hole (p<0.01, multiple regression analysis).
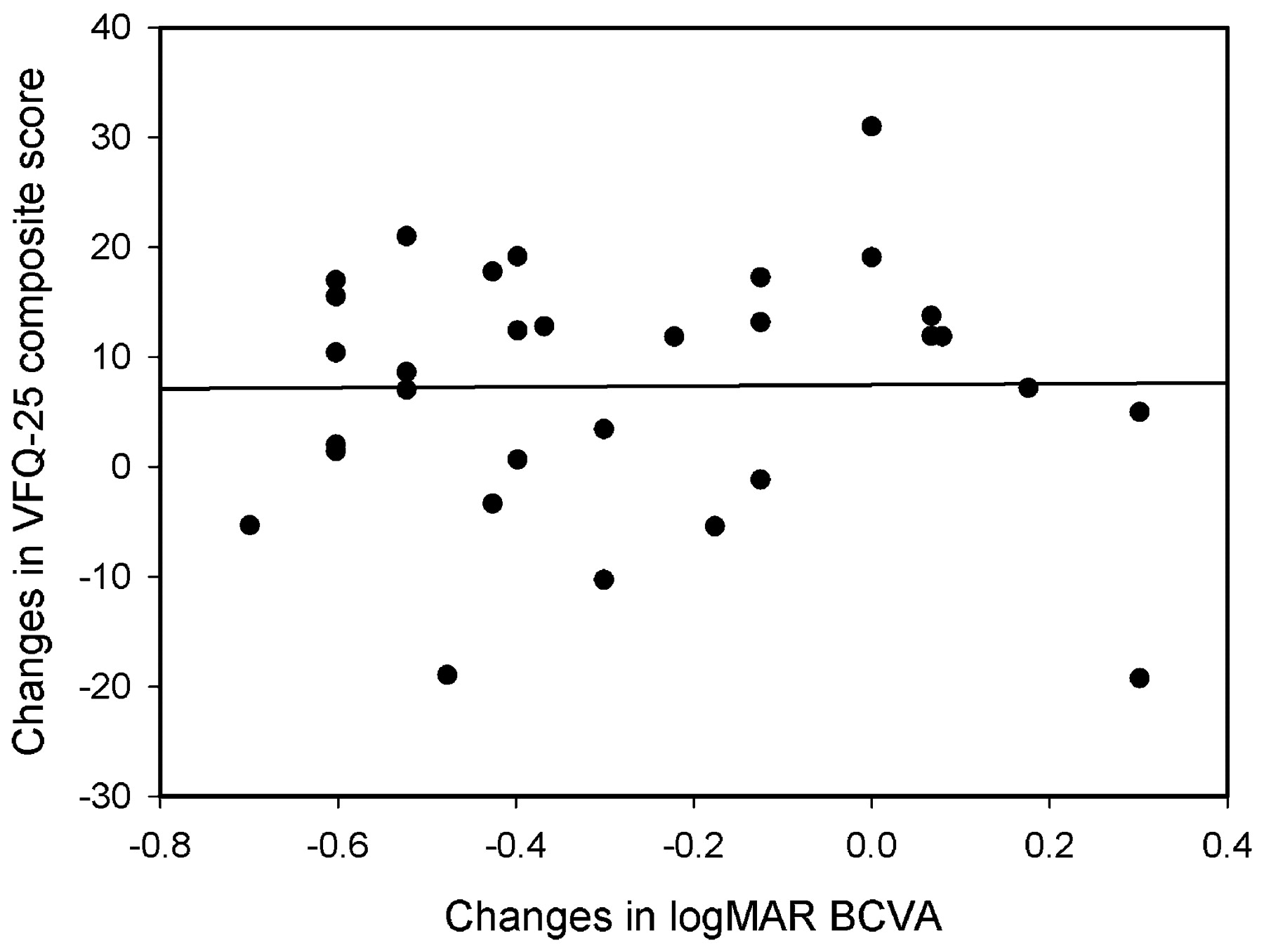
No significant correlation was found between changes in logarithm of minimum angle of resolution (logMAR) best corrected visual acuity (BCVA) and changes in the 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) composite score by vitrectomy for macular hole (p>0.05, multiple regression analysis).
{kind=link}
{kind=link}
{kind=link}
No significant correlation was found between changes in letter contrast sensitivity and changes in the 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) composite score by vitrectomy for macular hole (p>0.05, multiple regression analysis).
Results of multiple regression analysis on the National Eye Institute 25-item Visual Function Questionnaire (VFQ-25) composite score and explanatory variables
Discussion
As shown in the results, vitrectomy for MH significantly improved VFQ-25 composite score and subscale scores including general vision, near activities, distance activities, social functioning, mental health and dependency. This observation is consistent with the results of previous studies that also investigated VR-QOL in patients with MH.3 4 5
In the current study, multiple regression analysis revealed that the severity of metamorphopsia was significantly associated with VFQ-25 composite score, both preoperatively and postoperatively, while other variables were not related, such as visual acuity, letter contrast sensitivity, MHI and grade of cataract (LOCS III index). Further, changes in the severity of metamorphopsia were significantly correlated with changes in VFQ-25 composite score. These findings are not consistent with the results of a previous study.4 Tranos et al investigated VR-QOL in patients with MH and reported that postoperative VFQ-25 scores were significantly correlated with the severity of postoperative metamorphopsia recorded by measuring the number of squares representing distortion on the Amsler chart. However, preoperative and surgery-induced changes in VFQ-25 composite score were not associated with preoperative and changes in the severity of metamorphopsia.4 The discrepancy between our study and the previous studies may be attributable to the different methodology used to evaluate metamorphopsia. In previous studies, the severity of metamorphopsia was graded using the Amsler charts, which have been widely used to detect metamorphopsia in macular diseases.6 7 With the Amsler chart, however, precise and reproducible assessment of metamorphopsia is difficult because patients have to self-describe the degree of image distortion. On the other hand, the M-Charts can evaluate the degree of metamorphopsia quantitatively since patients need simply to answer whether the dotted line is distorted or not. With this chart, the degree of metamorphopsia is graded quantitatively from 0 to 2.0.8 9 It has been reported that the metamorphopsia score recorded by the M-charts increased depending on the severity of membrane proliferation classified by scanning laser ophthalmoscope images in patients with epiretinal membrane.8 Another study demonstrated that there was a significant positive correlation between the degree of retinal contraction obtained by using image-analysis software and metamorphopsia score quantified by the M-charts in patients with idiopathic epiretinal membrane.9
Preoperative, postoperative and surgery-induced changes in VFQ-25 scores did not correlate with visual acuity in both the better- and worse-seeing (operated) eyes. Miskala et al measured VFQ-25 in patients with subfoveal choroidal neovascularisation caused by age-related macular degeneration, and demonstrated that VFQ-25 subscale scores were significantly correlated with visual acuity in the better-seeing eyes, but not with visual acuity in the worse-seeing eyes.14 In patients with unilateral central retinal vein occlusion, Deramo et al reported that VFQ-25 responses were significantly correlated with visual acuity in the better-seeing eyes.15 In patients with early glaucoma with similar visual acuity bilaterally, Hyman et al demonstrated that VFQ-25 responses were significantly correlated with visual acuity in both the better- and worse-seeing eyes.16 Conversely, multiple regression analysis in the current study revealed that the severity of metamorphopsia was the single factor relevant to VR-QOL in patients with MH, while visual acuity was not included among the relevant factors. Moreover, the presence and severity of cataract were not associated with VR-QOL. Thus, metamorphopsia plays a key role in the deterioration of visual functioning and VR-QOL in patients with MH, even after successful closure of MH by vitrectomy. The severity of metamorphopsia after vitrectomy was actually 0.45 (SD 0.44), which is abnormally worse compared with normal controls.8 9
We found no association between letter contrast sensitivity and VFQ-25 composite score before and after surgery. Ghazi-Nouri et al reported that VFQ-25 responses correlated with visual acuity but not with contrast sensitivity obtained with the Pelli–Robson chart in patients with epiretinal membrane.17 In patients with proliferative diabetic retinopathy, VFQ-25 composite scores showed significant correlations with letter contrast sensitivity, as well as visual acuity.18 In patients after retinal reattachment surgery, VFQ-25 composite score was significantly correlated with contrast sensitivity and low-contrast visual acuity, whereas there was no correlation between the VFQ-25 composite score and BCVA.19 In a heterogeneous group of patients with multiple sclerosis, VFQ-25 composite scores were found to be modestly and significantly correlated with several clinical parameters, including visual acuity, contrast sensitivity, visual field, and 100-Hue colour vision.20 In patients with Bothnia dystrophy, a defined type of retinitis pigmentosa, age and low contrast visual acuity were significantly associated with the NEI-VFQ-25 composite score.21 Thus, factors contributing to VR-QOL are not uniform across different type of ocular diseases, and therefore it seems worthwhile to investigate individual diseases from the view point of VR-QOL.
We acknowledge certain limitations to our study. First, the sample size in our study was rather small. Second, postoperative follow-up was short. A previous study showed that VFQ-25 in patients with MH was more improved at 1 year postoperatively than at 3 months postoperatively.3 Moreover, metamorphopsia might have further improved with a longer follow-up. Tranos et al reported, however, that 65% of patients complained of metamorphopsia at 4 months after surgery.4 Future studies with a larger sample size and longer follow-up time will further facilitate our understanding of the relationship between VR-QOL and visual function, and other factors, in patients undergoing vitrectomy for MH.
In conclusion, the current study quantitatively indicated that MH surgery significantly improved VR-QOL, which was dependent on the improvement of metamorphopsia. The severity of preoperative and postoperative metamorphopsia was significantly correlated with preoperative and postoperative VFQ-25 scores, respectively. Metamorphopsia is an important factor not only in visual functioning, but also in the subjective QOL in patients with MH, both preoperatively and postoperatively.
REFERENCES
Footnotes
Funding Supported in part by Grants-in-Aid 19390439 for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan.
Competing interests None declared.
Ethics approval The research followed the tenets of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Tsukuba University Hospital.
Patient consent Obtained
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance