Article Text

Abstract
Background/aims To investigate the incidence of Nd:YAG-laser treatment for posterior capsular opacification (PCO) over a period of 5 years from phacoemulsification in an unselected population, comparing outcomes for three acrylic intraocular lenses (IOLs).
Methods Retrospective longitudinal cohort study comprising 900 eyes. Three subgroups of 300 eyes, receiving the AR40, AR40e (Abbott Medical Optics, Santa Ana, California), or BL27 (Bausch & Lomb, Rochester, New York) IOL respectively, were compared. Data on patient age, gender, IOL type, dates of cataract surgery, Nd:YAG-laser treatment and/or death, and visual acuities before/after cataract surgery/Nd:YAG-laser treatment were collected from five sources: cataract operation register, patient administration system, quality control system for cataract operations, Nd:YAG-laser treatment register and clinical patient records.
Results 216 eyes (24%) received Nd:YAG-laser treatment over a 5-year period. Statistically significant differences (p<0.001, χ2 test) were found between treatment rates for the three IOLs: AR40 73 eyes (24%), BL27 91 eyes (30%) and AR40e 52 eyes (17%). Eyes of patients who died during the follow-up period had fewer treatments (23/266, 8.6%) than eyes of patients living (193/634, 30%) at the end of the follow-up period.
Conclusion In comparison with a hydrophobic acrylic IOL with sharp posterior optic edge, a hydrophilic acrylic IOL was associated with almost twice the number of Nd:YAG-laser treatments over the 5-year period. The results are useful for discussing the economic long-term consequences of choosing an IOL with a design that makes PCO development more or less likely. Caution is advised when applying data from post-mortem PCO studies on living populations.
- Posterior capsular opacification
- phacoemulsification
- Nd-YAG lasers
- longitudinal survey
- retrospective study
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Posterior capsular opacification
- phacoemulsification
- Nd-YAG lasers
- longitudinal survey
- retrospective study
Introduction
Posterior capsular opacification (PCO) is arguably the most significant cause of visual problems after cataract surgery, the world’s most commonly performed operation. Visual acuity and subjective self-assessed visual function correlate to objective measurements of PCO and are improved by Nd:YAG-laser capsulotomy (hereinafter referred to as capsulotomy).1–3 Treatment, however, burdens the limited resources of healthcare systems. In 2007, 72 306 cataract operations were reported to the Swedish National Cataract Register.4 Publicly financed departments of ophthalmology in Sweden reported that year on average capsulotomies corresponding to 15% of their cataract operation volume (range 2–27%) (Swedish Ophthalmological Society: Verksamhetsberättelse för ögonsjukvården 2007, Annual report on ophthalmic healthcare 2007). Moreover, in developing countries, Nd:YAG-laser access can be limited. Reducing PCO development is therefore important. Proper surgical technique and intraocular lens (IOL) design—material, optic edge profile and haptic construction—stands out as a major factor in minimising PCO.5–9
For grading extent and monitoring successive development of PCO, computerised analysis of high-resolution digital photographs has replaced the previously common counting of capsulotomies, which, according to Buehl et al, should be avoided.10–12 In PCO research, a randomised prospective design is considered the gold standard and is chosen for meta-analyses in the field.10 13 14 Certainly reasonable when comparing PCO preventing measures, IOL designs, etc, this design has limitations when information is requested about the actual number of capsulotomies in a population undergoing cataract surgery. An attempt to model demand for capsulotomy based upon previous studies underestimated the actual need.15
In the central and western areas of the county of Östergötland, Sweden, the only care-provider offering cataract surgery (1400–2000 performed annually) and capsulotomy (250–360 performed annually) to approximately 250 000 citizens is the Department of Ophthalmology, Linköping University Hospital. These conditions make retrospective follow-up investigations relatively reliable regarding data completeness and/or description of dropouts. Patient cost for treatment/examination by a doctor within the public healthcare system is SEK 250 (€23, £19.50, $32, currency rates as of 18 June 2009), and the treating doctor is not reimbursed for capsulotomies. Over-/undertreatment for economic reasons is therefore unlikely. Instead, visual problems and posterior capsule appearance form the main basis for the decision to treat.
This epidemiological, longitudinal retrospective cohort study aims to describe the number of capsulotomies performed in a population of unselected cataract operated patients over a period of 5 years after phacoemulsification surgery and to examine the influence of mortality on the remaining number of eyes in potential need of future treatment. Three subpopulations receiving three different IOL types were investigated.
Materials and methods
Register data and patient record files for 900 phacoemulsification cataract surgeries performed between January 2000 and September 2002 at the Department of Ophthalmology, Linköping University Hospital, were retrospectively reviewed. During this period, three different acrylic IOL types were in common use at the clinic: Abbott Medical Optics (AMO) AR40, a hydrophobic three-piece IOL with rounded posterior optic edge (implanted January–November 2000), AMO AR40e, similar to AR40 except for a sharp posterior optic edge (implanted November 2001–September 2002) and Bausch&Lomb BL27, a hydrophilic 1-piece IOL with sharp posterior edge and two non-angulated loop haptics (implanted October 2000–April 2002). Figure 1 illustrates the IOL designs.
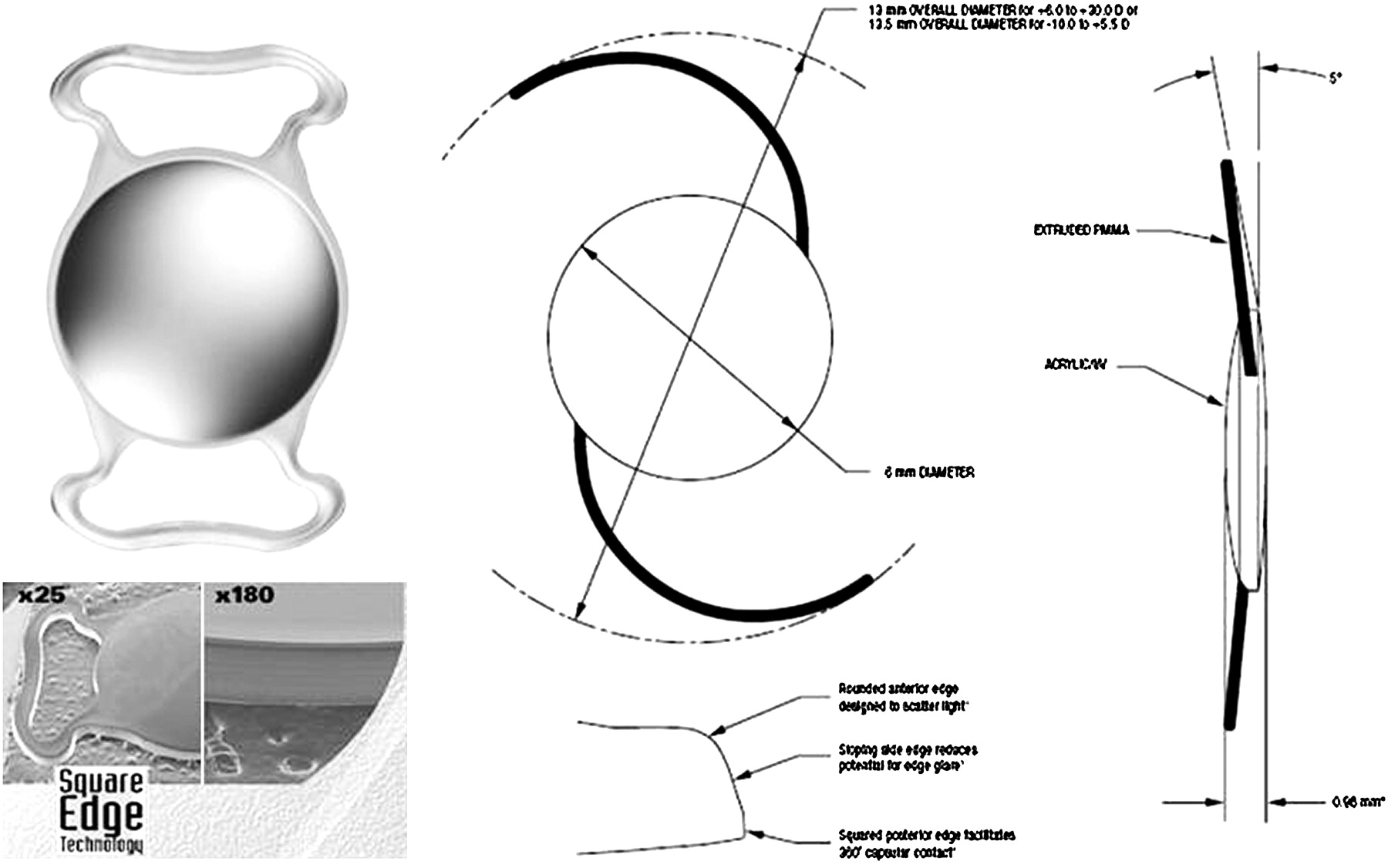
Top left: front photograph of BL27 (Bausch & Lomb, Rochester, New York) intraocular lens (IOL): hydrophilic acrylic single-piece IOL with two closed-loop non-angulated haptics. Bottom left: scanning electron microscope picture of the sharp (‘square’) posterior edge. Top centre and right: drawings of AR40e (Abbott Medical Optics, Santa Ana, California) IOL: three-piece IOL with hydrophobic acrylic optic and two angulated PMMA haptics. Bottom centre: bottom arrow indicates the sharp posterior edge. The AR40 (Abbott Medical Optics, Santa Ana, California) IOL design is identical to the AR40e except that the posterior optic edge is rounded. (Use of the illustrations has been granted by the two manufacturers.)
Several surgeons performed the phacoemulsification surgeries, all in topical anaesthesia except for a small percentage where general anaesthesia was indicated. Clear corneal incision, continuous curvilinear capsulorhexis created with microforceps and implantation of the IOL in the capsule using an injector were performed in all cases. The three IOLs in this study were all available as ‘standard IOLs’ at the clinic during different time periods. The BL27 was more commonly preferred by one surgeon (BJ), while the use of AMO IOLs was more evenly distributed among the surgeons (including BJ). Surgeon experience level and phacoemulsification technique were the same regardless of IOL. Several ophthalmologists, without correlation to which cataract surgeon performed the phacoemulsification, performed the capsulotomies.
The following data were extracted and transferred to an Excel database: patient age and gender, IOL type, dates of cataract surgery and—where applicable—date(s) of capsulotomy and/or death. Visual acuities (VA), in clinical practice measured with Snellens' letter chart at 5 m' distance, before and after cataract surgery, and, where applicable/retrievable, before and after capsulotomy were recorded.
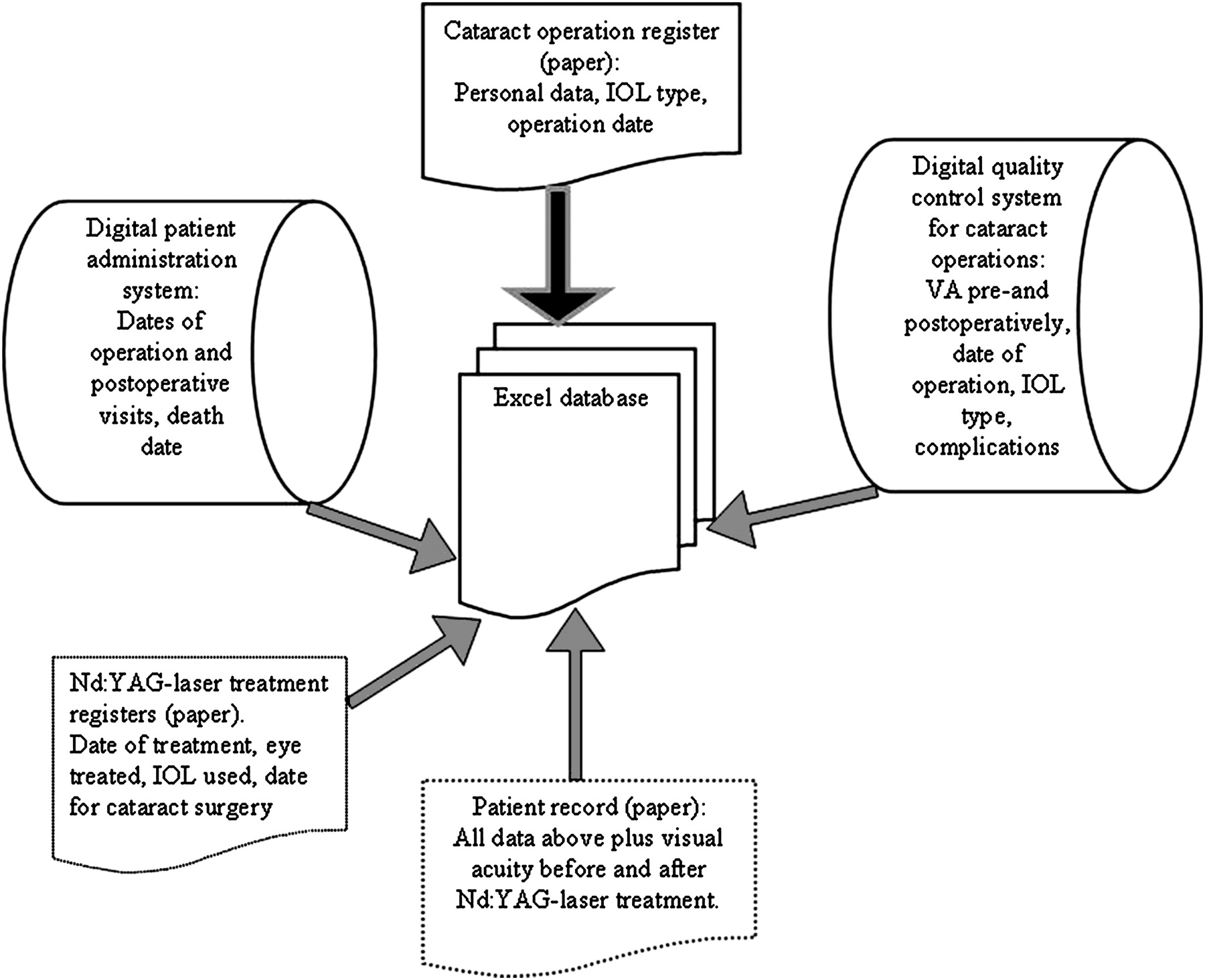
Patients and dates of operation were identified through the manual operation register, in which patient identification numbers and IOL identification labels were entered. For each IOL type, 300 operations were consecutively enrolled. The clinic’s digital quality control register for cataract operations provided information on visual acuity (VA) before and after surgery, and details of surgery were also recorded here. The digital patient administration system where each contact with the clinic was registered was used to track visits to the clinic after surgery. This system receives updates from the national population register as regards patient deaths. Clinical patient records (paper) and/or manual registers for capsulotomies were used to confirm and/or add data on capsulotomy and visual acuity (figure 2).

Data-acquisition flow chart. Study patients were enrolled (black arrow) through the manual operation register (top), which also provided basic information: date of birth, gender, date of cataract operation and type of intraocular lens (IOL). The digital databases (cylinders) and paper records provided additional data as indicated (grey arrows). Paper records were not retrieved in all cases (dotted contours), only if visits had been registered in the patient administration system after the postoperative control, or data on visual acuity (VA) before and after surgery had not been entered in the quality control system.
Cases were excluded if capsule damage during the surgery precluded secure placement of the IOL in the capsular bag. Minimal posterior capsular rupture or use of capsular tension ring did not prevent inclusion as long as the IOL could be placed completely in the bag with an intact anterior capsulorhexis. Cases with inconclusive data regarding capsulotomy were excluded.
The Regional Ethical Review Board in Linköping approved the study.
Statistical methods
For power calculation, pilot samples of 100 eyes per IOL were used for a computerised simulation of the logrank test. Five hundred simulations were performed for 11 sample sizes, n=20 to n=500. A sample size of 300 cases for each IOL was chosen for an estimated power of 84.6%, in order to establish differences between groups on the level p<0.05.
For comparison of survival curves, the logrank test feature of the statistical software Minitab v.15 was applied.
The Student t test and χ2 test were used to evaluate the statistical significances of differences between groups in the cross-sectional data, age, etc. A p level of <0.05 was considered statistically significant.
Results
Of 900 eyes included in the study 571 (63%) belonged to females, and 329 (37%) to males. The mean age at surgery was 76.7, median age 78.9. Figure 3 (top) shows the age/gender distributions at surgery. Two hundred and sixteen eyes (24%) had been treated with Nd:YAG-laser 5 years after the phacoemulsification surgery. Of the treated eyes, 148 (69%) belonged to females and 68 (31%) to males. The mean age at capsulotomy was 76.8, median age 78.8 (figure 3, bottom).

Top: age and gender distribution for patients whose eyes (n=900) were operated on for cataract with clear corneal incision phacoemulsification surgery, with implantation of foldable acrylic intraocular lens (IOL). The overall mean age was 76.7 (females 77.4, males 75.5), median age 78.9 (females 79.2, males 78.0). For the separate IOLs, the mean ages were 77.9 (AR40), 77.6 (BL27) and 74.5 (AR40e). The mean age was significantly lower for AR40e (p<0.01, t test), but there was no statistically significant difference in gender distribution between the three subgroups. Bottom: age and gender distribution for patients whose eyes received Nd:YAG-laser treatment for visually disturbing posterior capsular opacification (PCO) during the 5-year follow-up period after cataract surgery (n=216). In this group, the overall mean age was 76.8 (females 78.0, males 74.0), median age 78.8 (females 79.0, males 77.1).
In figure 4, the incidence of capsulotomy during the study period is shown for all eyes (thickest curve) and for the three different IOL subgroups. Five years after cataract operation, capsulotomy had been made in 73 eyes with the AR40 IOL, in 91 eyes with the BL27 IOL and in 52 eyes with the AR40e IOL, a statistically significant difference (p<0,001, χ2 test).

Kaplan–Meier graph showing how the number of untreated posterior capsules in 900 eyes operated on with phacoemulsification declines over time. Top curve (thick): The total incidence of capsulotomy during a 5-year period after phacoemulsification with implantation of an acrylic foldable intraocular lens (IOL), in an unselected cataract population (n=900 intact posterior capsules at start of follow-up). Approximately 1.5 years after phacoemulsification, the capsulotomy rate increases slightly. At 5 years after cataract surgery, 216 eyes had been treated with Nd:YAG-laser. The second top curve (less thick) shows the number of eyes with untreated posterior capsules remaining in alive patients. With capsulotomies and patient deaths included, 441 eyes remain eligible for future capsulotomy 5 years after cataract surgery. The three curves at the bottom of the graph show the rates of capsulotomies for the three IOL subgroups (n=300 intact posterior capsules for each subgroup at start of follow-up). With patient death included in the analysis, differences between the three survival curves are not statistically significant (logrank test, p=0.11). Of 300 eyes receiving an AR40e, 52 were treated with Nd:YAG-laser during the follow-up period, compared with 73 in the AR40 group and 91 in the BL27 group, a statistically significant difference (p<0.001, χ2 test).
In 266 (30%) of the 900 cases, the patient died before the end of the 5-year follow-up period. Figure 4 also shows the number of eyes remaining with intact capsules in living patients (second thickest curve). Four hundred and forty-one eyes were thus still eligible for capsulotomy at the end of the follow-up period. With both capsulotomy and death included in the analysis of the survival curves, there is no statistically significant difference between the three IOLs (p=0.11, logrank test).
Of the 266 eyes belonging to patients who died during the study period, 23 (8.6%) had received a capsulotomy, a clearly lower proportion than in the population still alive 5 years after cataract operation where 193 of 634 eyes (30%) received treatment.
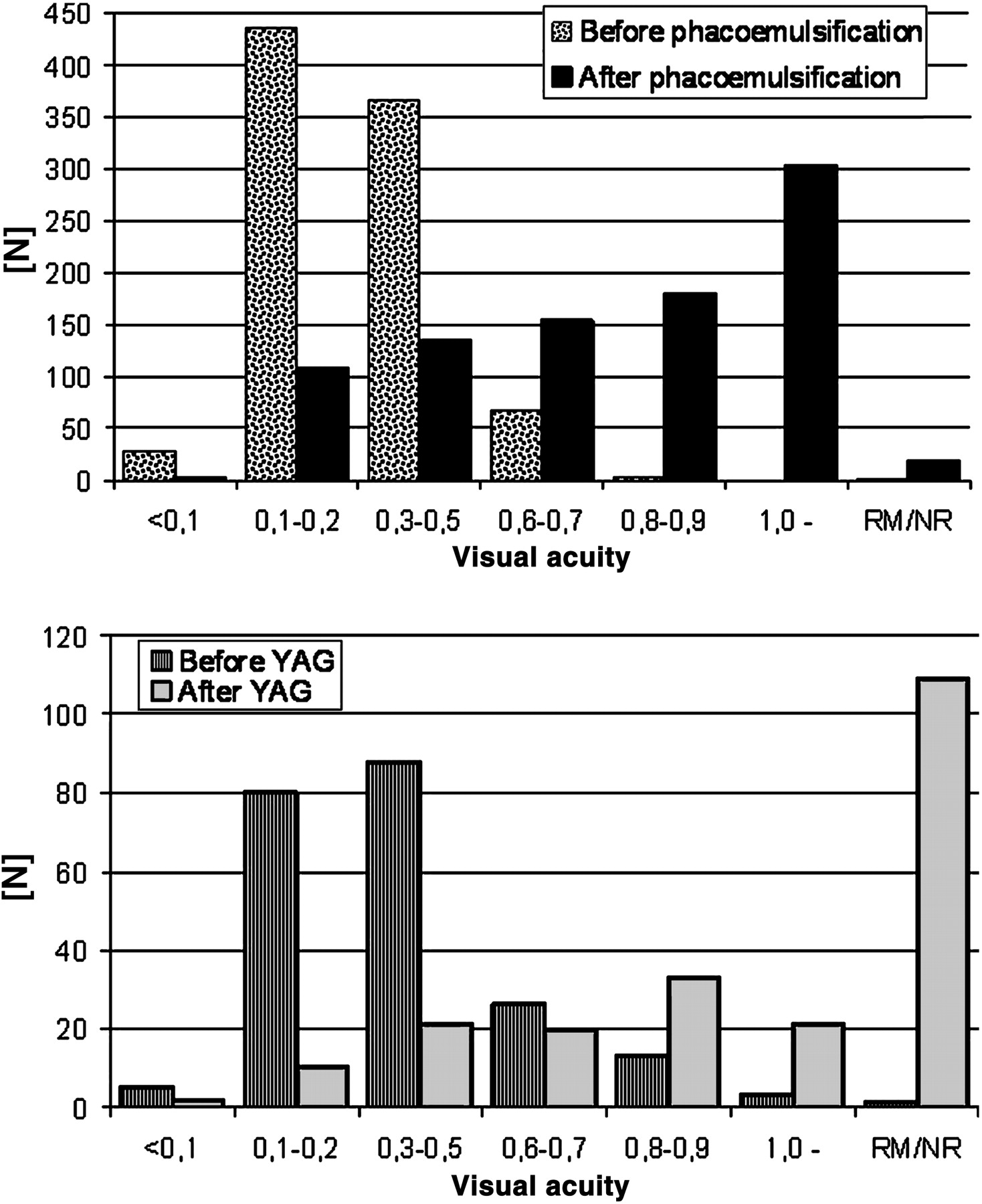
Data on VA before phacoemulsification were retrievable for all eyes operated on except one, and before capsulotomy for 215 of 216 treated eyes. After phacoemulsification, VA was not recorded in six cases, and in 13 cases postoperative records were unretrievable. VA after capsulotomy was recorded for 107 of 216 eyes, and for one eye no record was retrievable. Figure 5 shows VA distributions before and after phacoemulsification and capsulotomy respectively. Although some cases returned with worse VA due to PCO compared with VA before phacoemulsification, a larger proportion of eyes had a higher VA before PCO treatment than before phacoemulsification.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar graphs showing distributions of visual acuities (VA, horizontal axis) before and after phacoemulsification (top) and capsulotomy (bottom). NR, not recorded; RM, record missing. VA outcome was not followed up after capsulotomy in 108 of 216 eyes. It can be presumed that the majority of these cases regained a good subjective and objective VA.
Discussion
This study describes the demand over time for Nd:YAG-laser capsulotomy against visually disturbing PCO, during a follow-up period of 5 years after phacoemulsification cataract surgery in a non-selected population. Of 900 eyes operated on, 216 had capsulotomy. Patients who died before the end of follow-up were not excluded, in order to optimally describe the clinical outcomes in a group undergoing cataract extraction. During the follow-up period, 266 eyes left the study because the patient died. Of these, 243 had intact posterior capsules. After 5 years, 441 eyes thus remained eligible for potential future capsulotomy.
The 5-year mortality in this cataract-operated population is similar to the findings of a British study where 933 patients operated on in 2000 were followed up to the end of 2006, at which time 298 had died.16 Cataract patients have a high mean age, and consequently a limited expected remaining lifetime. Relatively few of those who died during the study period received capsulotomy in comparison with the significantly higher proportion in the subgroup surviving 5 years after cataract surgery. Apart from the obviously shorter follow-up time in patients who died before 5 years had passed after the phacoemulsification, and the previously shown correlation between increasing age and less PCO formation both in vivo and in vitro, this finding might be explained by elderly and/or sickly patients probably being less eager to seek medical help for deteriorating vision due to PCO.11 17 The data obtained here could be one explanation for the difference between estimated and real need for capsulotomy found by Cleary et al, as their model was built partially on figures from post-mortem studies.15
At 2.5 years after surgery, the three IOLs were equal regarding the number of performed capsulotomies. After 5 years, significant differences were evident, indicating that a hydrophobic acrylic IOL with sharp posterior edge is superior for long-term prevention of visually disturbing PCO. Differences between the two AMO IOLs have been shown in prospective randomised studies.18 19 The hydrophilic material of the BL27 appears less favourable in terms of PCO-preventing properties. This is in accordance with the conclusions of a study by Kugelberg et al, where the BL27, compared with the hydrophobic acrylic IOL Alcon AcrySof SA60AT, was associated with significantly more PCO formation and capsulotomies.20 Although it is tempting to attribute this to differing IOL material, methods using high magnification (500–1000×) scanning electron microscope photographs have recently shown that hydrophilic acrylic IOLs marketed as having sharp edges show significantly rounder optic edges than sharp-edged hydrophobic acrylic and silicone IOLs.21 22 Haptic design also differs between AR40 and AR40e on the one hand and BL27 on the other, which may have consequences for PCO development (figure 1).8
Although the three IOLs differed in cross-sectional data at 5 years, the survival curves were not significantly different with patient death included in the analysis. This means that at any given time during the study period, the probability that an eye with a certain IOL will be the next to come for a capsulotomy has not been shown to differ from a random outcome. This can decrease detectability in clinical practice of whether eyes with a certain IOL are more or less prone to require capsulotomy.
Retrospective non-randomised studies are usually attributed a less favourable scientific status. In a recent review article, Buehl and Findl included only prospective, randomised trials, where participants had age-related cataract without prior sight-threatening ocular disease (glaucoma, corneal disease, uveitis, traumatic or complicated cataract (eg, zonular weakness), retinal disease or history of diabetes mellitus with diabetic retinopathy).13 While this approach is defensible for a review article, one cannot avoid noticing the difference in characteristics between these prospectively studied populations and the non-selected population that cataract surgery centres handle in clinical practice. Therefore, duly recognising the value of well-designed prospective randomised studies, it seems reasonable to study outcomes retrospectively in non-selected populations. This will provide relevant information on the actual long-term impact of PCO in clinical practice, also with possibilities to compare different IOLs.
Studies such as this epidemiological, longitudinal retrospective cohort study with capsulotomy as primary endpoint can have difficulties tracking down every patient that has undergone capsulotomy, especially with more than one care-provider in the area. Patients with PCO on waiting lists or not seeking medical help will not be detected.23 Availability of, and reimbursement for, laser treatments can also influence the outcomes.12 When these issues can be controlled, retrospective studies may however provide valuable information that is impossible to access by means of randomised prospective studies of selected patient materials.24 The ophthalmic healthcare infrastructure in Linköping, as outlined in the Introduction, offers favourable conditions for retrospective research. It is also reasonable to optimally utilise the vast amounts of data fed into the various information systems used in healthcare.
For data quality, a study like this depends on the functionality of the public healthcare system within which it has been carried out: limited availability of Nd:YAG-laser treatment and the consequently long waiting lists could lead to falsely low capsulotomy rates, at least temporarily. The long follow-up period along with the commonly short waiting lists for capsulotomy (maximum 3–4 months) should compensate for this, and the absolute numbers of capsulotomies detected are not below what should be expected from previous literature. Kugelberg et al admittedly describes a 2-year capsulotomy rate in eyes with BL27 of 42% (24/57); but of these, 16 treatments were performed at the scheduled 2-year visit and only eight (14%) at the initiative of patients, analogously to this study.20 Strong features of this study are the large number of cases, few dropouts and a long study period, all comparing well with the studies Buehl and Findl included in their review, as well as the absence of significant economic obstacles and/or incentives.13 The results of this study should be generalisable for any healthcare system without significant economic bias from both a patient and a healthcare system perspective, and with good access to Nd:YAG-laser treatment.
As a consequence of a long follow-up time, other models have usually replaced the IOLs investigated at the time of study publication, which is the case for all three IOLs in this study. However, both the IOL materials and the sharp posterior optic edge design are used in presently marketed models. Therefore, these results can provide a basis for discussion about the long-term economic consequences of choosing an IOL whose design makes PCO development more or less likely.
In summary, this retrospective longitudinal follow-up study found an overall 5-year capsulotomy incidence of 24%. Hydrophobic acrylic IOL material and square posterior optic edge together were associated with significantly lower numbers of capsulotomies, compared with a hydrophilic IOL. The findings provide information about the strain on the ophthalmic healthcare system that different types of IOL may cause. The results also suggest caution when applying conclusions from post-mortem studies on living populations. Newer IOL models are currently being monitored for future comparison with this study.
Acknowledgments
The valuable assistance of O Eriksson, K Wahlin (statistical advice) and I Hutchinson (language check) is gratefully acknowledged.
References
Footnotes
Funding Kronprinsessan Margaretas Arbetsnämnd för synskadade (KMA), c/o Birgitta Lindgren, Fågelvägen 18, 645 40 Strängnäs, Sweden. Landstinget i Östergötland, SE 58185 Linköping, Sweden.
Competing interests The author is on the speaker’s list of Bausch & Lomb and as such has received reimbursement for expenses for several meetings. Bausch & Lomb provides financial and administrative support for research (not connected to the present paper). The author has no financial or other competing interests in any of the products or methods mentioned in the article.
Ethics approval Ethics approval was provided by The Regional Ethical Review Board in Linköping.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance