Article Text

Abstract
Background/aims To determine the potential efficacy and safety of combined verteporfin photodynamic therapy (PDT) with ranibizumab for the treatment of polypoidal choroidal vasculopathy (PCV).
Methods In this prospective, non-comparative, interventional study, 12 eyes from 12 patients that had active PCV were treated with PDT combined with three monthly intravitreal injections of ranibizumab. The patients were then monitored monthly with measurements of best-corrected visual acuity (BCVA) and central retinal thickness quantified by optical coherence tomography for 1 year. Indocyanine green angiography (ICGA) and fluorescein angiography were performed every 3 months. The eyes were re-treated with PDT and a ranibizumab injection, or with solely ranibizumab injection when indicated.
Results At month 12, the mean BCVA change from baseline was +12.3 letters (p=0.04). Eight patients (58.3%, p=0.02) had a BCVA gain of 15 letters or more. One patient (8.3%, p=1.0) had a BCVA loss of 15 letters or more. All patients underwent regression of polyps without recurrence. One patient experienced an insignificant subretinal haemorrhage. No other adverse event that could be attributed to the treatment was observed.
Conclusions This combination therapy showed encouraging results concerning improving vision, reducing the incidence of subretinal haemorrhage and reducing the recurrence of polyps when compared to previously published data that reported PDT monotherapy for PCV.
- Photodynamic therapy
- vascular endothelial growth factors
- choroidal neovascularisation
- retina
- treatment medical
Statistics from Altmetric.com
- Photodynamic therapy
- vascular endothelial growth factors
- choroidal neovascularisation
- retina
- treatment medical
Polypoidal choroidal vasculopathy (PCV) is a variation of choroidal neovascularisation (CNV), which is characterised by an abnormal-branching vascular network with polypoidal terminal bulbs in the inner choroids.1 Data from interventional case series indicate that photodynamic therapy (PDT) with veteporfin may be an effective treatment for PCV.2–9 When the best-corrected visual acuity (BCVA) was assessed 1 year after treatment, approximately 25–50% of eyes with active PCV that were treated with PDT had improved visual acuity of more than three lines.2 5 6 9 10 PDT also induced the regression of polypoidal bulbs in up to 90% of eyes.5 7 8 Subretinal haemorrhage and recurrence of the polyp are potential complications of PDT, with their respective incidences ranging from 4.7% to 30.8% 2 4–6 11 and from 4.5% to 50%2 5 6 8 9 11 over 1 year.
Vascular endothelial growth factor (VEGF) is an angiogenic signalling molecule triggered by tissue ischaemia and/or inflammation. It is overexpressed in the retinal pigment epithelial (RPE) cells of areas affected by CNV.12 The strong expression of VEGF has also been found in RPE and vascular endothelial cells in PCV lesions,13 and upregulation of VEGF has been demonstrated in the aqueous humour of eyes with active PCV.14 Another study, however, could not identify VEGF in vascular endothelial cells in PCV specimens, although VEGF was still found in RPE cells in these specimens.15
In two interventional case series,16 17 off-label intravitreal injections of bevacizumab, which is a full-length humanised antibody that inhibits all VEGF-A isoforms, were found to reduce the fluid leakage and exudative retinal detachment seen with PCV. This treatment, however, had only limited efficacy in inducing regression of the associated polyps, which were considered as mature vasculatures. In another small case series with a 4-month follow-up,18 three monthly injections of ranibizumab, a recombinant humanised IgG monoclonal antibody fragment that selectively binds to human VEGF-A, induced polyp regression in 9 out of 13 PCV lesions.
These data provide a rationale for combining an anti-VEGF agent with PDT for the treatment of PCV. In PDT monotherapy, the mechanism of selective photothrombosis19 causes regression of the polyp and allows pathological manifestations of PCV to improve gradually. Combining PDT with an anti-VEGF agent could create a synergistic effect, which induces polyp regression and reduces fluid leakage and inflammation. These effects would occur simultaneously, thereby enhancing the treatment benefits. Moreover, PDT was found to upregulate VEGF in eyes with CNV after treatment.20 This upregulation may also result to increased complications or the recurrence of disease in eyes after treatment with PDT.
We conducted the preliminary study reported herein to evaluate the potential efficacy and safety of combining ranibizumab with PDT for the treatment of PCV.
Methods
This prospective, consecutive, open-label, non-comparative, interventional study was conducted at the Eye Clinic of Rajavithi Hospital, Bangkok. The Ethical Committee on Research Involving Human Subjects of the same institution approved the study. The patients enrolled between June 2007 and March 2008. All patients gave written informed consent before they enrolled.
Patients and study design
Box 1 shows the inclusion and exclusion criteria for the study patients and eyes.
Box 1 Inclusion and exclusion criteria
The inclusion criteria
Patient criteria
(1) At least 50 years old.
(2) Willing to participate in monthly follow-up visits for at least 1 year.
Eye criteria
(1) Clinical presentation is compatible with neovascular AMD.
(2) Baseline BCVA ranges from a letter score of 34–73 after testing using the Early Treatment Diabetic Retinopathy Study chart protocol.
(3) Presence of polyps with or without an interconnecting vascular network identified using ICGA in the macular area, which is a characteristic of PCV. The presence of polyps identified on ICGA was described elsewhere.23
(4) Total lesion size identified by ICGA, including the vascular network and the terminal polyps, is less than 5400 μm in the greatest linear dimension.
The exclusion criteria
Patient criteria
(1) Previous systemic treatment with anti-angiogenic medications.
(2) Hypersensitivity to verteporfin, ranibizumab, fluorescein or indocyanine green.
(3) A diagnosis of porphyria.
(4) Severe systemic diseases, including hepatic diseases.
(5) Long-term (>6 months) use of systemic steroids (dose equivalent to 10 mg/day prednisolone or higher).
(6) Use of other medications with ocular toxicity, such as deferoxamine, chloroquine, hydroxychloroquine, tamoxifen, phenothiazine or ethambutol.
Eye criteria
(1) Previous treatment with anti-angiogenic medications, such as pegaptanib, ranibizumab, bevacizumab, anecortave or triamcinolone.
(2) Previous treatment with photodynamic therapy, radiation, laser photocoagulation in the macular area, vitrectomy, transpupillary thermotherapy, penetrating keratoplasty or glaucoma surgery.
(3) Previous complicated intraocular surgery less than 12 months ago or uncomplicated intraocular surgery less than 3 months ago.
(4) Other serious ophthalmic diseases such as diabetic retinopathy, uncontrolled glaucoma, vitreous haemorrhage, retinal detachment, macular hole, significant cataract, nasolacrimal duct obstruction or active intraocular inflammation.
(5) Specific diseases that cause choroidal neovascularisation such as angioid streaks, histoplasmosis, trauma and pathological myopia (>8.0 dioptres).
(6) An area of scar tissue that accounts for ≥50% of the lesion of PCV.
AMD, age-related macular degeneration; BCVA, best-corrected visual acuity; ICGA, indocyanine green angiography; PCV, polypoid choroidal vasculopathy.
We conducted a comprehensive examination of the study eyes of each patient at the baseline assessment and during each subsequent monthly visit for 1 year. The examination included a BCVA measurement, three-dimensional dilated fundus examination, colour fundus photography and central retinal thickness (CRT) quantified by optical coherence tomography (OCT; Zeiss OCT Model 3000, Dublin, California, USA). We measured BCVA using the standard Early Treatment Diabetic Retinopathy Study visual acuity testing protocol, using as the score the total number of correct letters identified at 4 m plus 30 letters. If the patients read fewer than five letters correctly at 4 m, we tested them again at 1 m. We then calculated the scores from the total number of correct letters identified at 1 m. We performed fundus fluorescein angiography and indocyanine green angiography (ICGA) using a digital fundus camera (Topcon 50IA, Topcon, Tokyo, Japan) or a scanning laser ophthalmoscope (Heidelberg Retinal Angiography II, Heidelberg, Germany) at the baseline examination and every 3 months thereafter.
Initial treatment
The initial treatment regimen consisted of a session of PDT (Visudyne; Novartis AG, Basel, Switzerland) guided by ICGA and an intravitreal injection of 0.5 mg ranibizumab (Lucentis; Genetech Inc, South San Francisco, CA) approximately 30 min after PDT, followed by additional intravitreal injections of ranibizumab each month over the next 2 months. The sequence of treatment on the first day, an injection of ranibizumab after a session of PDT, was based on the evidence that VEGF expression was enhanced in elderly human eyes after PDT.20
We administered PDT according to the Treatment of Age-Related Macular Degeneration with Photodynamic Therapy study protocol.21 We determined the diameter of the laser spot size by adding 1000 μm to the greatest linear dimension of PCV lesions determined by ICGA. We then asked the patients to wear protective sunglasses and avoid exposure to sunlight for 48 h after receiving PDT.
We gave the intravitreal injection using standard protocols.22 We also prescribed the application of topical antibiotics for 3 days after each intravitreal injection.
Re-treatment
We re-treated the study eyes during follow-up visits when the previously treated area had one of the following: (1) an area of hyperfluorescence suggesting an active polyp on ICGA (the criteria for defining active polyps on ICGA were described elsewhere23; an area of vascular network identified on ICGA was not re-treated if ICGA could not identify the associated active polyps and fluorescein angiography could not identify leakage); (2) an area of leakage demonstrated by fluorescein angiography although the polypoidal or the vascular network component of PCV could not be identified on ICGA; (3) a presence of intraretinal or subretinal fluid by OCT; or (4) an increase of CRT by OCT for 100 μm or more compared to the lowest previous CRT value. Only when these findings were not found did the ophthalmologists consider re-treatment of the eyes if they determined that re-treatment would be beneficial.
If the decision to re-treat was based on the ICGA or fluorescein angiography criteria, the re-treatment consisted of a session of PDT and an intravitreal injection of ranibizumab approximately 30 min after PDT. The PDT was guided by ICGA if polyps were identified, and by fluorescein angiography if fluorescein angiography leakage was found without polyp identified on ICGA. If the decision to re-treat was based on the OCT criteria only, the re-treatment consisted solely of an injection of ranibizumab.
These indications for re-treatment are summarised in an additional table A1 (available online).
Outcome measures and statistical analysis
Visual outcome measures included the mean BCVA change in letters from baseline and the categorical BCVA change. Concerning the categorical change, we defined moderate gain in, or loss of, vision as gaining or losing 15 letters of BCVA or more from the baseline.
We used Wilcoxon signed rank test to determine the significance of changes of the mean BCVA and CRT from the baseline. We used McNemar's test to analyse the proportion of patients who had moderate visual gain and loss, leakage demonstrated by fluorescein angiography, and polyp regression for significant changes from the baseline. We used a p value of <0.05 for statistical significance for both tests.
Results
We treated 12 eyes in 12 patients who were consecutively enrolled during the study period (table 1).
Patient demographics and baseline characteristics
Visual outcomes
The mean BCVA improved significantly from the baseline from month 2 (table 2) and continued to improve significantly until month 5, when the best BCVA was achieved (an average gain of 15.4 letters from the baseline, p=0.01). By month 6, there was a four-letter loss of the mean BCVA from that recorded during month 5. This was because four patients lost more than five letters in the BCVA. However, during month 7, the mean BCVA improved by three letters from month 6 and improved significantly from the baseline (14.7 letters, p=0.02). This significant gain from the baseline of the mean BCVA was maintained until month 12.
Visual acuity outcomes and re-treatment at each month
A significant proportion of patients had moderate gain in vision from month 4. Seven patients (58.3%, p=0.02) at months 4, 5 and 12, and 6 patients (50%, p=0.03) from months 6 to 11 had a moderate gain in vision. We did not define any patient as having moderate loss of vision until one patient (8.3%, p=1.0 (patient 11; see table 2)) showed such loss in month 12.
Angiographic and OCT outcomes
There were seven eyes that had associated retinal pigment epithelial detachment (RPED), four of which had haemorrhagic and three had fibrovascular RPED. All RPEDs were located in the macular area. The size of RPEDs ranged approximately from 0.5 to 4 disc area. We found no association between RPEDs and treatment outcomes.
We found that patients who had a polyp identified on ICGA all had leakage identified on fluorescein angiography, but patients who had polyp regression on ICGA might still have a leakage that can only be visualised on fluorescein angiography. During the third month of follow-up, we observed polyp regression without fluorescein angiography leakage in 10 patients (83.3%, p=0.002) and persistent polyps in two patients. By month 6, 11 patients had polyp regression (91.7%, p=0.001), and 8 had no leakage on fluorescein angiography (66.7%, p=0.008). Three patients had fluorescein angiography leakage without polyps, and one patient had persistent polyps. By month 9, 11 patients had polyp regression and 10 had no fluorescein angiography leakage (83.3%, p=0.002); one patient had fluorescein angiography leakage without polyps while another had persistent polyps. At month 12, all patients had evidence of polyp regression (p<0.0001), and 9 patients had no leakage on fluorescein angiography (75%, p=0.004). Patients 9, 10 and 11 had leakage on fluorescein angiography without polyps. We did not observe any recurrence of polyps in any of the patients over 12 months.
All eyes that had subretinal or intraretinal fluid before treatment showed complete resolution of the fluid by OCT within 2 months after the first day of treatment. No eye had recurrence of the fluid within 1 year. The mean CRT decreased significantly from the baseline from the first month of follow-up (a mean CRT of 215.8 or a 69 μm decrease from the baseline, p=0.002) and was maintained throughout follow-up with a mean CRT of 200.8 μm at month 12 (an 84 μm decrease from the baseline, p=0.01). The mean thicknesses found during month 8 (a mean CRT of 180.6 or a 104.2 μm decrease from the baseline, p=0.003) and month 1 were the thinnest and thickest, respectively. No eye had an increase of CRT for 100 μm or more compared to the lowest previous CRT value at any point within the follow-up period.
The mean CRT of each patient at each month is displayed in an additional table A2 (available online). Fundus photographs, fluorescein angiography, ICGA and OCT of patient 6 before and after treatment are shown in figure 1.

Fundus photos, fluorescein angiography, indocyanine green angiography (ICGA) and optical coherence tomography (OCT) of patient 6 before the combination therapy, at months 6 and 12 after the treatment. (A) Fundus photo, at baseline, showing haemorrhagic retinal pigment epithelial detachment (RPED) involving the fovea with subretinal scar tissue at the superotemporal macular. The patient's best-corrected visual acuity (BCVA) was 40 letters. (B) Fluorescein angiography showing leakage with staining of the scar. (C) ICGA showing focal hyperfluorescence indicating an active polyp. (D) OCT showing RPED with subretinal fluid. (E) Fundus photo, at month 6, after only one session of the combination therapy, showing resolution of the haemorrhagic RPED. The patient's BCVA was 76 letters. (F) Fluorescein angiography showing no leakage with the staining of the scar. (G) ICGA showing disappearance of the polyp with vascular branching network identified at the temporal macular. (H) OCT showing resolution of the RPED and no subretinal fluid. (I) Fundus photo, at month 12, showing no recurrence of PCV. The patient's BCVA was 80 letters. (J) Fluorescein angiography still showing no leakage with the staining of the scar. (K) ICGA showing no recurrence of the polyp with the vascular network identified. (L) OCT still showing resolution of the RPED and no subretinal fluid.
Re-treatments
Table 2 outlines the re-treatments that we gave to the study patients over the follow-up period. Of the 12 episodes of re-treatments, 7 were due to leakage identified by fluorescein angiography without an identified coexisting polyp. At month 12, there were three patients who were re-treated due to this fluorescein angiography leakage. Table 3 summarises the number of patients that we treated with PDT and ranibizumab over 12 months. The mean episodes of PDT and mean injections of ranibizumab over 12 months, including the treatments in the initial regimen, were 1.9 and 4.2, respectively.
Number of patients treated with verteporfin photodynamic therapy (PDT) and ranibizumab
Adverse events
A small subretinal haemorrhage of 1 disc area, without a coexisting polyp detected on ICGA, occurred at month 12 in patient 7, who had a persistent polyp from the baseline until month 9. This patient had a total of four episodes of PDT and seven injections of ranibizumab. We did not observe any other adverse event, either systemic or ocular, in any other patient over 12 months.
Discussion
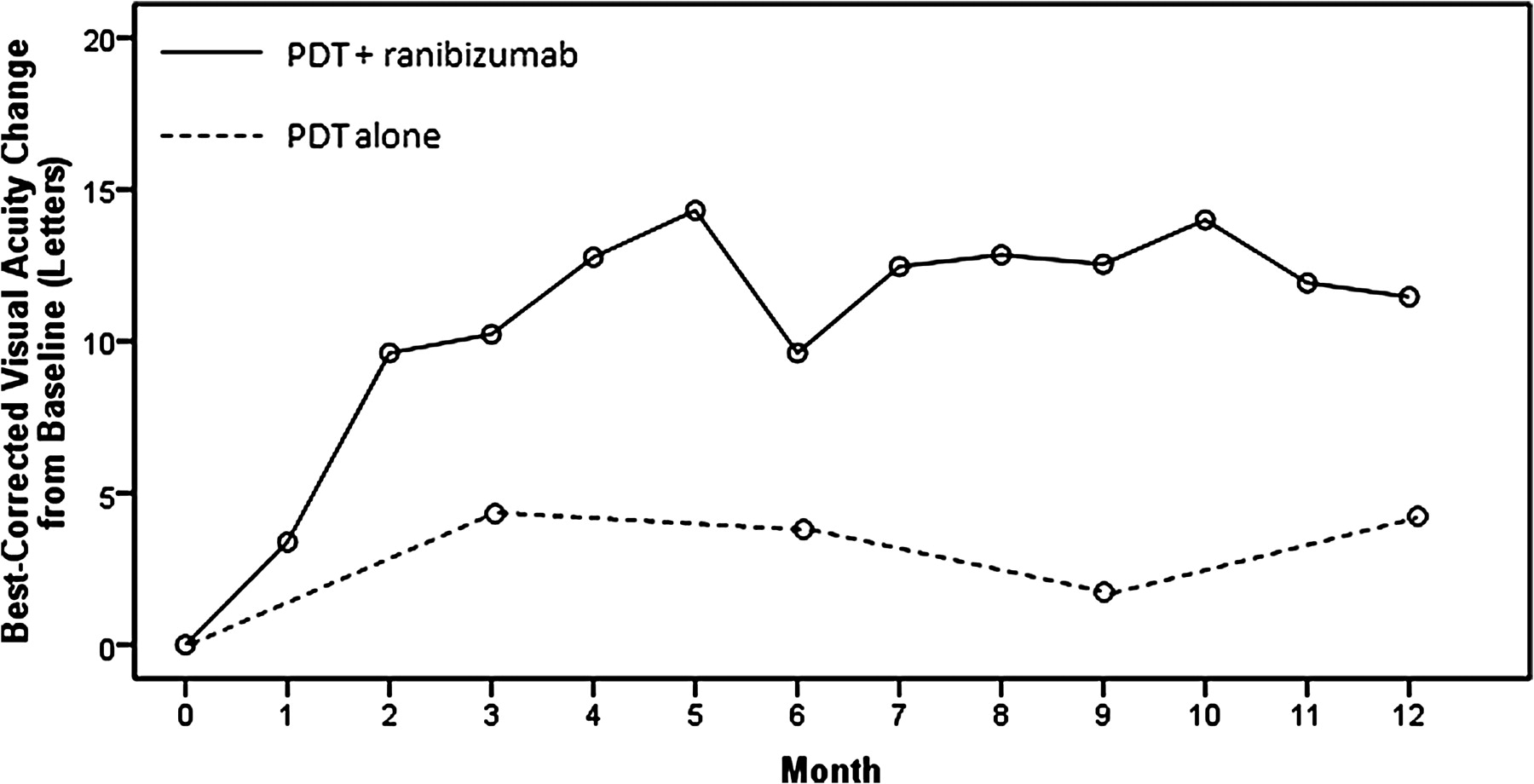
The results suggest that combining ranibizumab with PDT might increase the degree of visual improvement obtained from PDT alone for the treatment of PCV. Table 4 summarises the 1-year results of the previously published studies of PDT monotherapy for PCV. The combination therapy used in this study resulted in a significantly higher gain in BCVA than that reported in those studies. This gain was approximately three times the average value of the mean BCVA gain at each interval of 3 months that was reported in those studies (figure 2 and table 4). Moreover, the proportion of patients with moderate gain in vision (58.3%) and moderate loss of vision (8.3%) at 1 year in this study was comparable with the highest proportion of patients with moderate gain in vision (50%) and the lowest proportion of patients with moderate loss of vision (5%) at 1 year, as reported by Eandi et al and Chan et al, respectively.5 9
One-year results of verteporfin PDT alone for the treatment of polypoidal choroidal vasculopathy in published studies compared with the combination therapy in this study
{kind=link}
{kind=link}
The mean best-corrected visual acuity change over time after combination therapy (top line) and of photodynamic therapy (PDT) alone in previously published studies (bottom line).
We hypothesise that the larger improvement in vision after the use of combination therapy results from the synergistic effect of PDT and ranibizumab. After PDT, a balance in angiogenesis, which is regulated in part by VEGF, is crucial for the beneficial effect to occur. Physiological regenerative angiogenesis is required for the recanalisation of the choriocapillaris, which is temporarily occluded by PDT. However, pathological angiogenesis may account for adverse events, such as subretinal haemorrhage and the recurrence of polyps. A study by Kim et al demonstrated that combined intravitreal ranibizumab injections with PDT in an animal model did not adversely affect the recanalisation of the choriocapillaris compared to PDT alone.25 We also found no evidence of permanent non-perfusion affecting the choriocapillaris in any of the eyes reported herein. Moreover, we did not find any recurrent polyps and only one patient developed a subretinal haemorrhage after treatment, which was insignificant clinically. This suggested that the combination therapy might have balanced the angiogenesis after PDT and minimised VEGF-related adverse events and recurrence of disease.
Combination therapy, however, did not lessen the number of patients who required re-treatment or reduce the total number of re-treatments over 1 year when compared to data in the studies of PDT alone (table 4). This indicated that there were patients, such as patient 7, whose polyps were recalcitrant to the combination therapy. Other patients, such as patients 9, 10 and 11, had polyps that responded well to combination therapy, as indicated by regression on ICGA; however, the activity of the lesions as detected by leakage identified by fluorescein angiography recurred by month 6 when the effect of the initial treatment faded. Moreover, the re-treatment regimen in this study had limited efficacy in treating this fluorescein angiography leakage. More importantly, we found that this area of leakage seen with fluorescein angiography without polyps may translate into the clinical symptom of loss of vision.
It is therefore important to make an emphasis here that, after treatments or during natural courses, the disappearance of polyps on ICGA does not guarantee quiescence of activity of PCV lesions. This activity can be identified as leakage on fluorescein angiography better than as leakage on ICGA. Surprisingly, OCT, as demonstrated in this study, may not identify subretinal or intraretinal fluid although the leakage is found on fluorescein angiography.
The finding of fluorescein angiography leakage without polyps after treatment with combination therapy in this study was consistent with that reported in other studies of PDT monotherapy for PCV, in which the proportion of patients with polyp regression on ICGA outnumbered the proportion of patients without leakage on fluorescein angiography after treatment.5 8 This leakage may reflect the activity of the vascular network component of PCV, which continues despite the obliteration of the polypoidal component of PCV by PDT.26 The clinical course of this network tends to behave like typical CNV rather than PCV. Thus, anti-VEGF alone may be more effective than either combining PDT with an anti-VEGF agent or PDT alone for the treatment of the vascular network.
While the prospective, monthly follow-up of the study patients for the duration of a year is a strength of this study, there are inherent weaknesses due to the small sample size and the lack of a control group. The comparison of treatment results among the published case series of PDT monotherapy for PCV also demonstrated limitations. The designs of these series were different: four were retrospective and three were prospective; moreover, the methods of measuring outcomes (such as BCVA determination) and the criteria for defining outcomes (such as subretinal haemorrhage after treatment) were not uniform. However, the mean BCVA at baseline in this study (50.7 letters) was comparable with the average value of the mean BCVA at baseline reported among those series (50.4 letters). The criteria for re-treatment, which were based on angiographic outcomes, were uniform between those series and our study.
In summary, the treatment of PCV using PDT combined with ranibizumab showed encouraging results with respect to the improvement of vision when compared to data from the published studies of PDT monotherapy. At present, there is no randomised controlled trial that compares PDT monotherapy and PDT combined with ranibizumab for the treatment of PCV. Other important issues concerning combination therapy for the treatment of PCV, such as the use of different anti-VEGF agents, the number of the initial anti-VEGF injections and the re-treatment regimen, should also be investigated.
Acknowledgments
This study was supported by research funds from Rajavithi Hospital, Bangkok, Thailand. The use of ranibizumab in this study was supported by Novartis (Thailand). The authors acknowledge Drs Chairat Saovaprut, Atchara Ampornprut, Jiravut Limwattanayingyong and Atchareeya Sanmee at the Center of Excellence in Retina Diseases, Department of Medical Services, Ministry of Public Health, Thailand, for their support. The authors also acknowledge Dr Sid Borirak from the University of California, San Francisco, for his kind assistance in the review of this paper.
References
Supplementary materials
Web Only Data bjo.2009.173120
Files in this Data Supplement:
Web Only Data bjo.2009.173120
Files in this Data Supplement:
Footnotes
Funding Research funds of Rajavithi Hospital.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Ethical Committee on Research Involving Human Subjects of Rajavithi Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.