Article Text

Background/aims To determine to what extent subjects implanted with the Argus II retinal prosthesis can improve performance compared with residual native vision in a spatial-motor task.
Methods High-contrast square stimuli (5.85 cm sides) were displayed in random locations on a 19″ (48.3 cm) touch screen monitor located 12″ (30.5 cm) in front of the subject. Subjects were instructed to locate and touch the square centre with the system on and then off (40 trials each). The coordinates of the square centre and location touched were recorded.
Results Ninety-six percent (26/27) of subjects showed a significant improvement in accuracy and 93% (25/27) show a significant improvement in repeatability with the system on compared with off (p<0.05, Student t test). A group of five subjects that had both accuracy and repeatability values <250 pixels (7.4 cm) with the system off (ie, using only their residual vision) was significantly more accurate and repeatable than the remainder of the cohort (p<0.01). Of this group, four subjects showed a significant improvement in both accuracy and repeatability with the system on.
Conclusion In a study on the largest cohort of visual prosthesis recipients to date, we found that artificial vision augments information from existing vision in a spatial-motor task.
Clinical trials registry no NCT00407602.
- Retinal prosthesis
- retinitis pigmentosa
- low vision
- retinal degeneration
- retina
- degeneration
- clinical trial
- low vision aid
- prosthesis
Statistics from Altmetric.com
- Retinal prosthesis
- retinitis pigmentosa
- low vision
- retinal degeneration
- retina
- degeneration
- clinical trial
- low vision aid
- prosthesis
Introduction
Second Sight Medical Products (Sylmar, California, USA) has developed an epiretinal prosthesis aimed at partially restoring vision to people blinded by outer retinal degenerative diseases such as retinitis pigmentosa (RP). In these diseases, while the photoreceptors are compromised and there is anatomical remodelling of the remnant retina,1 2 post mortem anatomical studies have found that some bipolar and ganglion cells survive.3 4 Multiple acute and chronic studies in normal5–9 and degenerate10 animal models, and in human subjects, have shown that electrical stimulation of the retina can elicit percepts (phosphenes).11–13 More recently it has been demonstrated that stimulation with multiple electrodes can yield some level of spatial vision as measured by high-contrast square-wave grating tests.14
The Argus II retinal prosthesis system (Second Sight Medical Products) consists of a surgically implanted 60-electrode stimulating microelectrode array consisting of 200 μm diameter disc electrodes, an inductive coil link used to transmit power and data to the internal portion of the implant, an external belt-worn video processing unit (VPU) and a miniature camera mounted on a pair of glasses (figure 1). The video camera captures a portion of the visual field and relays the information to the VPU. The VPU digitises the signal in real-time, applies a series of image processing filters, down-samples the image to a 6×10 pixelised grid, and creates a series of stimulus pulses based on pixel brightness values and look-up tables customised for each subject. The stimulus pulses are delivered to the microelectrode array via application-specific circuitry and a superior-temporally placed inductive radio frequency coil link allowing for wireless forward and reverse telemetry between intra and extra-ocular portions of the system.

A schematic illustration showing the surgically implanted stimulating microelectrode array, and inductive coil telemetry link of the Argus II system (left). The external portions of the system consist of a video processing unit (VPU) (middle) and a miniature camera mounted on a pair of glasses (right).
Here we present results of a task requiring the integration of visual information afforded by the Argus II retinal prosthesis with motor movement—the localisation of a high contrast square target on a computer monitor.
Methods
Blind subjects with severe to profound RP were implanted with the Argus II prosthesis as part of a clinical study at multiple clinical sites worldwide. Those centres were: Doheny Eye Institute at the University of Southern California (Los Angeles, California, USA); Retina Foundation of the Southwest (Dallas, Texas, USA); Moorfields Eye Hospital (London, UK); University of California at San Francisco (San Francisco, California, USA); Wilmer Eye Institute at the Johns Hopkins School of Medicine (Baltimore, Maryland, USA); Wills Eye Institute at the University of Pennsylvania (Philadelphia, Pennsylvania, USA), the Edward S. Harkness Eye Institute at Columbia University (New York, USA); Puerta de Hierro Centro Medico (Guadalajara, Mexico); Centre Hospitalier National d'Ophtalmologie des Quinze-Vingts (Paris, France); Hôpitaux Universitaires de Genève (Geneva, Switzerland). All data presented here were collected at these clinical sites, with the exception of sites in Philadelphia and New York, where psychophysical testing and data collection were done at the Scheie Eye Institute at the University of Pennsylvania and Lighthouse International, respectively.
All implanted subjects had some level of bare light perception (BLP) prior to surgery, and at the time of the latest clinical follow-up. No subjects had a recordable visual acuity prior to surgery (worse than 2.9 logarithm of the minimum angle of resolution (logMAR)) (ie, worse than 20/15887) as determined by an adaptive four alternative force choice (4-AFC) square wave grating test.
The experiments described in here were run on all Argus II subjects who were currently available for regular testing and who had been implanted before 1 July 2009 (27 subjects). Nineteen of the 27 subjects (70%) included in this study were male. At the time of publication the mean subject age was 58±10 (range 27–77) years; the mean duration of implantation was 430±314 (range 60–857) days.
In the experiment, white square stimuli (5.85 cm2, 200 pixels2, 221 cd/m2) were displayed in random locations on a 19″ (48.3 cm) LCD touch screen monitor (ELO Accutouch or IntelliTouch Surface Wave LCD Touch Screen Flat Monitor 1915L; Menlo Park, California, USA) located 12″ (30.5 cm) in front of the subject (subtending a visual angle of 10.9°). After the onset of the square and an auditory prompt, the subjects were instructed to locate and touch the square centre. The program provided verbal feedback after subject's responses indicating ‘correct’ for a touch anywhere on the square and ‘close’ for a touch within 100 pixels (2.9 cm) of the edge of the square. Corrective feedback was given after ‘close’ and incorrect responses. For example, a response 6 cm to the left of and 4 cm below the stimulus square prompted the response ‘It was higher and right.’
Before the test was administered, 10 trials were presented in ‘training mode’ to familiarise the subject with the position and vertical and horizontal extent of the monitor. In this mode subjects defined the location of the square centre by pressing the blank touch screen monitor; a 5.85 cm square appeared at that location until subjects touched another part of the monitor. The subjects' cameras were aligned with respect to the monitor centre. Experiments consisting of 40 trials were run with both the system on and off (80 trials total per subject). The subjects' eyes were not patched in either condition; in system off testing the subjects did not wear the Argus II system glasses.
Subjects were instructed to move their head while keeping their eyes centred relative to their head position. (Since the stimulating array is fixed on retina, the perceived phosphene location depends on eye and head position.) The x–y pixel coordinates of the square centre and of the location touched were recorded for off-line analysis and plotting using Matlab 7.1, Microsoft Excel 2007 and Igor Pro 6.1.
Results
The accuracy of subject responses in an experiment was determined by calculating the mean distance between individual responses and target square centre. For display purposes, subjects were ordered from smallest improvement in accuracy with the system on compared with off, to largest improvement system on compared with off. The ordered list of 27 subjects was divided into nine sections, and system on and system off results for the median performer from each sub-section are shown in figure 2. In these plots the responses are plotted relative to a fixed target square location centred at (0, 0). These nine subjects are representative of the range of results.

Results from square localisation experiments of nine representative subjects with the system off and on. Plots are normalised to square centre; responses (white circles) are plotted relative to target square location (axes units are in pixels). Standard deviations of the mean of all responses in an experiment are indicated (dotted line). The subjects are plotted from smallest (top left) to largest (bottom right) factor of improvement in accuracy (system on vs off).
Each subject's mean accuracy for system on and off is presented in figure 3. (Subjects showing the greatest improvement with the system on are presented on the right.) Ninety-six percent (26/27) of subjects showed statistically significant improvement in accuracy with the system on compared with off (p<0.05, two-tailed unpaired Student t test). Subject JHU-003 was slightly more accurate with the system on compared with off; however, the improvement was not statistically significant. The mean distance from the target for all subjects for all tests was 149±50 pixels with the system on, and 323±94 pixels with the system off.

Mean distance from target square centre (pixels) for each subject with system on (black square) and off (white circles). Range of standard error of mean is shown by vertical bars. Subjects are plotted in order of increasing factor of improvement in accuracy (system on vs off).
The repeatability (or clustering) of subject's responses was determined by calculating the mean difference between individual responses and the mean of all responses. Ninety-three percent (25/27) of subjects have significantly better repeatability with the system on compared with off. (JHU-003 and JHU-005 are more repeatable with the system off compared with on.) There is a high correlation between subjects' repeatability and their accuracy with both the system on (R2=0.88, slope=0.82) and off (R2=0.90, slope=1.00) (figure 4).

Repeatability (pixels) versus accuracy (pixels) for all subjects with system on (top) and system off (bottom). Linear regression (dashed line) for system off (y=1.00x–22.9; R2=0.90) and system on (y=0.82x+7.9; R2=0.88) shows a good correlation between subject's ability mean response distance from target and the clustering of their responses. The five subjects (JHU-003, LON-001, JHU-005, MAN-001 and PENN-001) that had success with the task with their native vision are clearly separated from the rest of the cohort in the system off plot.
Discussion
The square localisation task described here assessed the ability of blind subjects implanted with the Argus II retinal prosthesis system to localise and touch a high contrast square target on a touch screen monitor. Successful performance of the task required subjects to develop adequate head-scanning technique and good ‘camera-hand’ coordination. Ninety-six percent of implanted subjects studied had responses that were significantly more accurate, and 93% had responses that were more repeatable with the system on compared with the system off. There was a high correlation between accuracy and repeatability with both the system on (R2=0.88) and off (R2=0.90). This is intuitive since a subject that can more often correctly determine the target centre also gets more visual feedback with which to refine motor movement.
For the subjects who showed significant improvement in accuracy with the system on compared with the system off, the factor of improvement ranged from 1.25 (LON-001) to 4.63 (JHU-002). This range was largely due to the variability in performance with the system off. (The standard deviation of the mean accuracy across all subjects was 86.3 pixels with the system off compared with 51.4 with the system on.) In other words, the rare cases of only marginal improvement in accuracy with the system on were due to the fact that a few subjects had enough light perception and eye-hand coordination to perform the task with their native vision. This limited the possible range of improvement with the system on. Possible secondary explanations for the wide range of factor of improvement include differences in array–retina apposition and array–macula distance, and in subject-specific variability in performing psychophysical tasks.
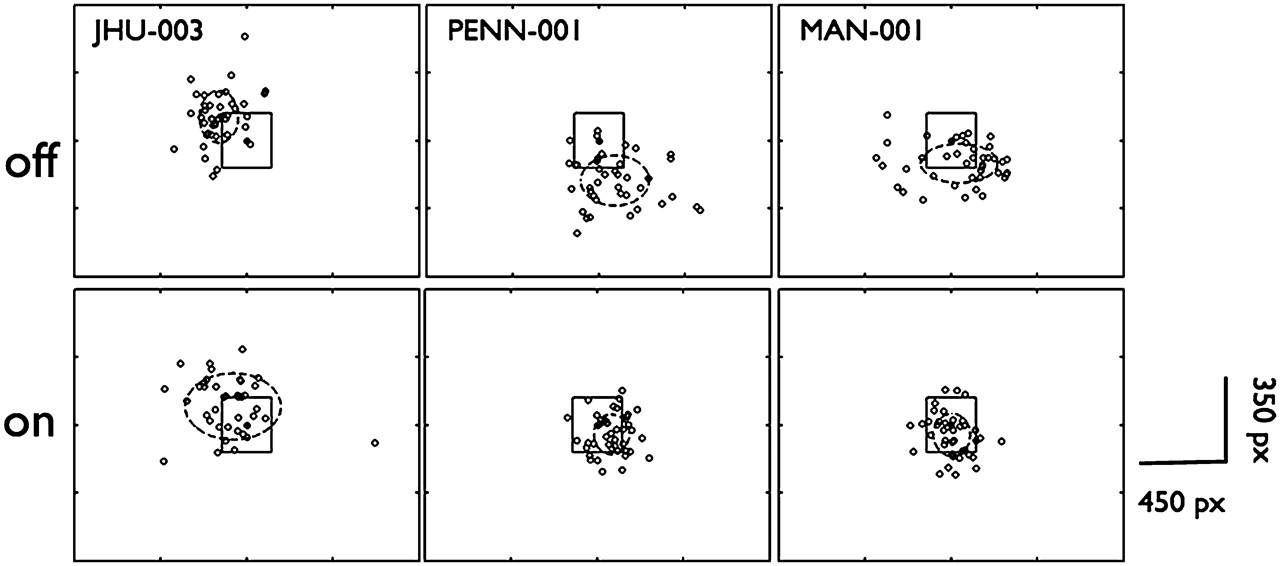
Case reports of those whose sight is partially restored after years of blindness indicate that motor tasks requiring hand-eye coordination (eg, maze tracing, picking up small pellets) are adversely affected after prolonged binocular visual deprivation.15 16 Similarly, subjects in this study who had the most success on this task with their native vision were still consistently off the square centre with system off due to years of lack of visual feedback (JHU-003, MAN-001, PENN-001; figure 5). Therefore, in determining subjects who could perform the task with their native vision, both accuracy and repeatability were considered. The bottom of figure 4 shows a plot of repeatability versus accuracy with system off. There is a clear clustering of five subjects who were significantly better at performing the task with their native vision compared with all other subjects. These subjects (JHU-003, LON-001, JHU-005, MAN-001 and PENN-001) had both repeatability and accuracy values <250 pixels. Even though these subjects had enough residual native vision and visual-motor feedback to perform well, remarkably four of five of these subjects still showed a significant improvement in accuracy with system on compared with off and had a mean distance from the square centre of less than 150 pixels (4.4 cm) with the system on (all except JHU-003). This suggests that these subjects were able to synergise visual input from the prosthesis system with their residual native vision, which would be a prerequisite for implanting individuals with better sight with the Argus II system. This perhaps surprising result that artificial vision augmented performance rather than interfered with it lends support to the idea that, like with other sensory prostheses such as cochlear implants, individuals with better vision than those studied here may also benefit from prosthesis use. We believe this is the first report of a visual prosthesis improving the performance of blind subjects, even those with a measureable amount of native vision, in a spatial-motor task over such a large cohort.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results from square localisation experiments with the system off (top) and on (bottom) for JHU-001, MAN-001 and PENN-001. Plots are normalised to square centre; responses (empty circles) are plotted relative to target square location (axes units are in pixels). Standard deviations of the mean of all responses in an experiment are indicated (dotted line). Although all subjects could perform the task with their native vision, years of visual deprivation effect of spatial-motor feedback. Two of three (MAN-001 and PENN-001) of these subjects' accuracy and repeatability improved with the system on.
References
Footnotes
Funding National Institutes of Health (Bethesda, MD, USA) grant no. 5R01EY12893.
Competing interests AKA, JDD, AC, MJMcM and RJG are employees of and have a financial interest in Second Sight Medical Products. GD, LdaC and PS belong to institutions that receive funding from Second Sight Medical Products to support the study. The individuals themselves have no financial interest in Second Sight Medical Products.
Patient consent Obtained.
Ethics approval This study was conducted with ethics approval from all participating clinical sites: Doheny Eye Institute at the University of Southern California (Los Angeles, California, USA); Retina Foundation of the Southwest (Dallas, Texas, USA); Moorfields Eye Hospital (London, UK); the University of California at San Francisco (San Francisco, California, USA); Wilmer Eye Institute at the Johns Hopkins School of Medicine (Baltimore, Maryland, USA); Wills Eye Institute at the University of Pennsylvania and the Scheie Eye Institute (Philadelphia, Pennsylvania, USA), The Edward S. Harkness Eye Institute at Columbia University and Lighthouse International (New York, USA); Puerta de Hierro Centro Medico (Guadalajara, Mexico); Centre Hospitalier National de Ophtalmologie des Quinze-Vingts (Paris, France); Hôpitaux Universitaires de Genève (Geneva, Switzerland).
Provenance and peer review Not commissioned; externally peer reviewed.