Article Text

Abstract
Aim To assess the early clinical outcomes of an ICL with a central hole (Hole ICL) implantation for the correction of moderate to high myopia.
Methods This study evaluated 20 eyes of 20 patients with spherical equivalents of −7.36±2.13 D (mean±SD) who underwent Hole ICL implantation. Before surgery and at 1 week and 1, 3 and 6 months after surgery, we assessed the safety, efficacy, predictability, stability and adverse events of the surgery.
Results Logarithm of the minimum angle of resolution (logMAR) uncorrected visual acuity and logMAR best spectacle-corrected visual acuity were −0.20±0.12 and −0.25±0.06, respectively, 6 months after surgery. The safety and efficacy indices were 1.13±0.24 and 1.03±0.30, respectively. At 6 months, 95%, and 100% eyes were within ±0.5 and ±1.0 D of the targeted correction, respectively. Change in manifest refraction from week 1 to month 6 was 0.06±0.28 D. No significant rise in intraocular pressure (including pupillary block) or a secondary cataract occurred in any case during the period of observation.
Conclusions Implantation of a newly developed Hole ICL offered good results for all measures of safety, efficacy, predictability and stability for the correction of moderate to high myopic errors, even without peripheral iridectomy, suggesting its viability as a surgical option for the treatment of such eyes.
- Hole ICL
- phakic IOL
- myopia
- posterior chamber
Statistics from Altmetric.com
Introduction
Laser in situ keratomileusis has gained widespread popularity as a safe and effective surgical method for the correction of myopia, but patients with high myopia or thin corneas face some restrictions to avoid the possible risk of developing keratectasia. Moreover, a large amount of laser ablation may lead to the deterioration of superior intrinsic corneal optical performance. The Visian Implantable Collamer Lens (ICL; STAAR Surgical, Nidau, Switzerland), a posterior chamber phakic intraocular lens (IOL) that was developed to overcome these disadvantages has been reported to be effective for the correction of moderate to high ametropia.1–10 In addition, this surgical procedure is largely reversible, and unlike laser in situ keratomileusis, allows exchange of the lens, even when unexpected refractive changes occur after surgery. Recently, toric ICL has also been demonstrated to be effective for the correction of high myopic astigmatism.11–14 However, in order to prevent pupillary block, this surgical technique unavoidably requires two preoperative laser iridectomies, which are frequently accompanied by some pain, especially in younger subjects; or intraoperative peripheral iridectomy, which is sometimes complicated by iris haemorrhage, causing surgical difficulties. Moreover, there are still ongoing concerns, not only for the patient but also for the surgeon, about the risk of cataract formation, presumably resulting from direct physical contact between the ICL and the crystalline lens or from localised malnutrition causing poor circulation of the aqueous humour. We recently developed a new ICL with an artificial central hole (Hole ICL) in order to overcome these disadvantages.15–17 Fujisawa et al15 demonstrated in a porcine model that an ICL with a 3.0-mm central hole was highly effective for reducing the incidence of cataract formation, possibly by improving the circulation of the aqueous humour to the anterior surface of the crystalline lens. Shiratani et al16 reported that the modulation transfer function (MTF) of an ICL with a 1.0-mm central hole was similar to that of an ICL without a hole. Uozato et al17 showed that the in vitro optical performance of an ICL with a 0.36-mm central hole at various IOL powers fulfils the International Organisation for Standardization (ISO) criterion for MTF, which requires a contrast above 28% with a 3.0-mm effective aperture diameter. However, no clinical studies on implantation of a newly developed ICL have yet been conducted. The purpose of the current study was to assess prospectively the first clinical outcomes of Hole ICL implantation in the correction of moderate to high myopia.
Methods
Twenty eyes of 20 patients (eight men and 12 women), who underwent implantation of the posterior chamber phakic ICL having a 0.36-mm artificial central hole (Hole ICL; STAAR Surgical) for the correction of moderate to high myopia, were included in this observational study. The mean patient age at the time of surgery was 31.7±8.0 (range 23 to 49) years. The preoperative manifest spherical equivalent was −7.36±2.13 (range −3.50 to −11.75) D. The preoperative manifest refractive cylinder was 0.73±0.51 (range 0.00 to 1.50) D. Eyes with keratoconus were excluded from the study by using the keratoconus screening test of Placido disk videokeratography (TMS-2; Tomey, Nagoya, Japan). Before surgery and at 1 week, and at 1, 3, and 6 months after surgery, we determined the following in addition to the usual slit-lamp biomicroscopic and funduscopic examinations: the logarithm of the minimal angle of resolution (logMAR) of uncorrected visual acuity (UCVA), logMAR of best spectacle-corrected visual acuity (BSCVA), manifest refraction (spherical equivalent), intraocular pressure (IOP) (including 1 day postoperatively) and endothelial cell density (except for 1 week, and 1 and 3 months postoperatively). Before surgery, the horizontal white-to-white distance and anterior chamber depth were measured using a scanning-slit topograph (Orbscan IIz; Bausch & Lomb, Rochester, New York, USA), and the mean keratometric readings and the central corneal thickness were obtained using an autorefractometer (ARK-700A; Nidek, Gamagori, Japan) and an ultrasound pachymeter (DGH-500; DGH Technologies, Exton, Pennsylvania, USA), respectively. The IOP was assessed with a non-contact tonometer (KT-500; Kowa, Tokyo, Japan). The endothelial cell density was determined with a non-contact specular microscope (SP-8800; Konan, Nishinomiya, Japan).
ICL power calculation
ICL power calculation was performed by the manufacturer (STAAR Surgical) using a modified vertex formula. In all eyes, emmetropia was selected as the target refraction to reduce the preoperative refractive errors as much as possible. The size of the ICL was also chosen by the manufacturer on the basis of the horizontal corneal diameter and the anterior chamber depth measured with scanning-slit topography (Orbscan IIz).
ICL surgical procedure
On the day of surgery, the patients were administered dilating and cycloplegic agents. After topical anaesthesia, a model V4 ICL was inserted through a 3-mm temporal clear corneal incision with the use of an injector cartridge (STAAR Surgical) after placement of a viscosurgical device (Opegan; Santen, Osaka, Japan) into the anterior chamber. The ICL was placed in the posterior chamber, the viscosurgical device was completely washed out of the anterior chamber with balanced salt solution, and a miotic agent was instilled. The patients did not undergo preoperative or intraoperative peripheral iridectomies. All surgeries were uneventful and no intraoperative complication was observed. After surgery, steroidal (0.1% betamethasone; Rinderon; Shionogi, Osaka, Japan) and antibiotic (levofloxacin; Cravit; Santen, Osaka, Japan) medications were administered topically four times daily for 2 weeks, the dose being reduced gradually thereafter.
Statistical analysis
All statistical analyses were performed using StatView version 5.0 (SAS). The Wilcoxon signed-rank test was used for statistical analysis to compare the pre- and post-surgical data. Unless otherwise indicated, the results are expressed as mean±SD, and a value of p<0.05 was considered statistically significant.
Results
Patient population
The preoperative demographics of the study population are summarised in table 1. LogMAR UCVA and BSCVA were 1.35±0.22 (range 1.00 to 2.00) and −0.21±0.09 (range −0.30 to −0.08), respectively. The horizontal white-to-white distance was 11.5±0.4 (range 10.7 to 12.1) mm and the anterior chamber depth was 3.13±0.22 (range 2.80 to 3.59) mm. The mean keratometric reading was 43.8±1.8 (range 40.9 to 47.4) D, the central corneal thickness was 533.1±34.7 (range 468 to 600) μm, the IOP was 13.1±1.7 (range 10.0 to 15.7) mm Hg and the endothelial cell density was 2798±225 (range 2328 to 3221) cells/mm2.
Preoperative patient demographics
Safety outcomes
LogMAR BSCVA was −0.22±0.06, −0.24±0.08, −0.25±0.06 and −0.25±0.06, 1 week, and 1, 3 and 6 months after surgery, respectively. We found a significant difference between preoperative BSCVA and 6-month postoperative BSCVA (p=0.05, Wilcoxon signed-rank test). The safety index (mean postoperative BSCVA/mean preoperative BSCVA) was 1.05±0.22, 1.11±0.23, 1.13±0.26 and 1.13±0.24 at 1 week, and 1, 3 and 6 months after surgery, respectively. Twelve eyes (60%) showed no change in BSCVA, five eyes (25%) gained 1 line and two eyes (10%) gained 2 lines, while one eye (5%) lost 1 line, but no eyes had lost more than one line 6 months after Hole ICL implantation (figure 1).

Changes in best spectacle-corrected visual acuity (BSCVA) after implantation of an implantable collamer lens with a central hole (Hole ICL).
Effectiveness outcomes
LogMAR UCVA was −0.16±0.09, −0.17±0.11, −0.21±0.11 and −0.20±0.12, 1 week and 1, 3 and 6 months after surgery, respectively. We found a significant difference between preoperative UCVA and 6-month postoperative UCVA (p<0.001, Wilcoxon signed-rank test). The efficacy index (mean postoperative UCVA/mean preoperative BSCVA) was 0.91±0.21, 0.96±0.28, 1.04±0.31,and 1.03±0.30, 1 week and 1, 3 and 6 months after surgery, respectively. One week and 1, 3 and 6 months after surgery, 100%, 100%, 100%, and 100% of eyes, and 95%, 95%, 100%, and 100% of eyes, respectively, had a UCVA of 20/40, and of 20/20 or better.
Predictability
A scatter plot of the attempted versus the archived manifest spherical equivalent correction is shown in figure 2. One week, and 1, 3, and 6 months after surgery, 95%, 100%, 100% and 95% of eyes, and 100%, 100%, 100% and 100% of eyes were within ±0.5 and ±1.0 D, respectively, of the attempted spherical equivalent correction.

Scatter plot of attempted versus achieved correction (spherical equivalent) after implantation of an implantable collamer lens with a central hole (Hole ICL).
Stability
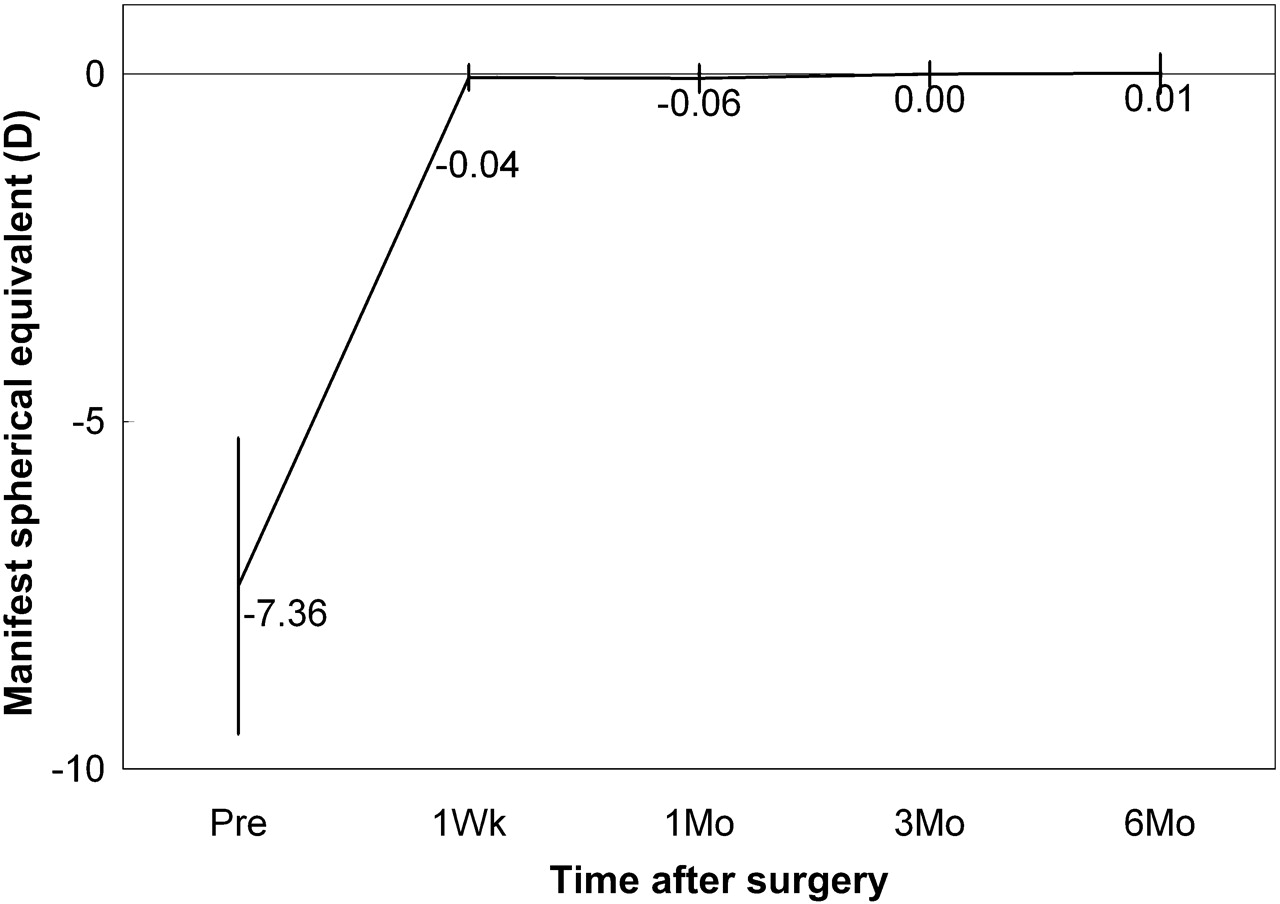
The change in the manifest spherical equivalent is shown in figure 3. One week and 1, 3 and 6 months after surgery the mean manifest spherical equivalent was −0.04±0.19, −0.06±0.20, 0.00±0.19 and 0.01±0.29 D, respectively. Manifest spherical equivalent was significantly decreased, from −7.36±2.13 D preoperatively to 0.01±0.29 D 6 months postoperatively (p<0.001, Wilcoxon signed-rank test). The change in manifest refraction from 1 week to 6 months was 0.06±0.28 D.

Time course of manifest spherical equivalent after implantation of an implantable collamer lens with a central hole (Hole ICL).
IOP
The IOP was 11.3±2.6, 13.2±3.2, 12.9±3.3, 12.8±2.5 and 13.0±3.0 mm Hg at 1 day, 1 week and 1, 3 and 6 months after surgery, respectively. No significant increase in IOP (>21 mm Hg) occurred in any case during the observation period.
Endothelial cell density
The endothelial cell density changed, but not significantly, from 2798±224 cells/mm2 preoperatively to 2720±268 cells/mm2 6 months postoperatively (p=0.16, Wilcoxon signed-rank test). The mean percentage of endothelial cell loss was 2.8% at 6 months after implantation.
Secondary surgeries/adverse events
There were no intraoperative complications and all implantations were uneventful. None of the following was seen at any time during the observation period: cataract formation, pigment dispersion glaucoma, pupillary block or any other vision-threatening complication (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Slit-lamp photograph of the eye after implantation of an implantable collamer lens with a central hole (Hole ICL).
Discussion
In the present study, our results with Hole ICL implantation were favourable in all measures of safety, efficacy, predictability and stability when used for the correction of high myopic astigmatism throughout the 6-month follow-up period, suggesting its viability as a surgical option for the treatment of such eyes. With regard to the safety and efficacy of the procedures, ICL implantation was safe and effective for the correction of moderate to high myopia, a finding that was in line with previous studies.1–10 With regard to predictability and stability, ICL implantation is also excellent for the treatment of moderate to high myopia. It may be that ICL implantation through a 3-mm corneal incision, regardless of the amount of myopic correction, has a negligible effect on refractive outcome, and that this surgical technique is less subject to the wound healing responses of the cornea.10
With regard to the complications of this surgical technique, we found no significant rise in IOP (including pupillary block) throughout the 6-month observation period, even without preoperative or intraoperative peripheral iridectomy. This finding may also support the view that postoperative pupillary block can be prevented by the presence of the central hole in the ICL. Conventional ICL implantation inevitably requires preoperative laser iridectomies or intraoperative peripheral iridectomy in order to prevent the occurrence of the pupillary block. The former is frequently accompanied by some pain, especially in younger subjects, resulting in patient dissatisfaction; and the latter is sometimes accompanied with iris haemorrhage, adding to the difficulty of the surgical procedure. Hence, we believe that Hole ICL implantation has many advantages over conventional ICL implantation in the management of preoperative pain, intraoperative iris haemorrhage and IOP, because it does not require these additional procedures. Moreover, we found no cataract formation throughout the study period. Although we accept that a relatively short follow-up in a small number of the patients is insufficient for the detection of rare complications, this finding may support the view that the presence of the central hole may contribute to the improvement of the circulation of the aqueous humour to the anterior surface of the crystalline lens, resulting in less cataract formation. The US Food and Drug Administration (FDA) Trial demonstrated that the incidence of anterior subcapsular cataract with ICL V4 was 2.7%.8 Sanders et al reported that 31 (5.9%) of 526 eyes developed symptomatic and asymptomatic anterior subcapsular cataracts.18 Kamiya et al previously demonstrated that the incidence of cataract formation with ICL V4 was 10.7% 4 years after ICL implantation if traumatic cataract formation was excluded,10 and 5.4% 1 year after toric ICL implantation.14 Fujisawa et al15 reported that the insertion of an ICL causes a change in the dynamics of the intraocular aqueous humour. Although we speculate that the new design may influence the rate of cataract formation, presumably because of the improvement of the circulation of the aqueous humour to the anterior surface of the crystalline lens, further investigations are required to clarify this point. Otherwise, there were no significant complications in Hole ICL-implanted eyes during the 6-month observation period, partly because of the small sample size of the patients and the relatively short follow-up time. However, from a statistical standpoint, the sample size is insufficient for the detection of rare complications. More prolonged and careful observation is still required to assess the long-term safety of this surgical procedure.
There are concerns about the optical performance of the new ICL with a central artificial hole because the presence of the central hole may deteriorate the optical quality of the IOL by, for example, introducing glare or halo. We previously reported that the MTF, obtained using the Zemax optical simulation software, of an ICL with a central hole (diameter 1.0 mm) in the optic region was similar to that of an unperforated ICL.16 We also showed, using an in vitro optical simulation model, that the differences in MTF between a Hole ICL and a conventional ICL were small and clinically negligible, and that the in vitro optical performance of ICL with a 0.36-mm central hole at various IOL powers fulfils the ISO criterion for MTF.17 We are currently conducting a new study to make a detailed comparison of the optical performance of Hole ICLs and conventional ICLs.
In summary, our results indicate that Hole ICL implantation is safe and effective, and provides predictable and stable refractive results in the correction of moderate to high myopia throughout a 6-month observation period. Moreover, no vision-threatening complications occurred throughout the follow-up period. These findings suggest that this new surgical approach, which does not require additional iridectomies, may be a good alternative to current corneal refractive procedures for the treatment of such eyes.
References
Footnotes
Funding KS is a consultant to STAAR Surgical. No other financial interest exists.
Competing interests None.
Patient consent Obtained.
Ethics approval The study was approved by the Institutional Review Board at Kitasato University School of Medicine, and followed the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance