Article Text

Abstract
Background/aims To evaluate the cost-effectiveness of ranibizumab as either monotherapy or combined with laser therapy, compared with laser monotherapy, in the treatment of diabetic macular oedema (DME) causing visual impairment from a UK healthcare payer perspective.
Methods A Markov model simulated long-term outcomes and costs of treating DME in one eye (BCVA ≤75 letters) based on data from the RESTORE Phase III trial. Outcomes measured in quality-adjusted life-years (QALYs) were simulated for a 15-year time horizon based on 12-month follow-up from RESTORE and published long-term data. Costs included treatment, disease monitoring, visual impairment and blindness (at 2010 price levels).
Results Ranibizumab monotherapy resulted in a 0.17 QALY gain at an incremental cost of £4191 relative to laser monotherapy, yielding an incremental cost-effectiveness ratio (ICER) of £24 028. Probabilistic sensitivity analysis showed a 64% probability of being cost-effective at a threshold of £30 000 per QALY. Combined ranibizumab and laser therapy resulted in a 0.13 QALY gain at an incremental cost of £4695 relative to laser monotherapy (ICER £36 106; 42% probability of ICER <£30 000).
Conclusions Based on RESTORE 1-year follow-up data, ranibizumab monotherapy appears to be cost-effective relative to laser monotherapy, the current standard of care. Cost-effectiveness of combination therapy is less certain. Ongoing studies will further inform on disease progression and the need for additional ranibizumab treatment.
- Ranibizumab
- diabetic macular oedema
- visual impairment
- cost-effectiveness
- macula
- treatment medical
- clinical trial
- epidemiology
- public health
- vision
- retina
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Ranibizumab
- diabetic macular oedema
- visual impairment
- cost-effectiveness
- macula
- treatment medical
- clinical trial
- epidemiology
- public health
- vision
- retina
Introduction
Diabetic macular oedema (DME) is the most frequent cause of vision impairment in people with diabetes and can lead to blindness if left untreated. Even when patients receive optimal treatment with the current standard of care for DME, laser photocoagulation, improvements in vision are relatively uncommon and many patients lose vision despite laser therapy.1 2 This continued vision loss is the result of structural and physiological damage to the retinal capillary bed, and from progressive and permanent damage to the macular pigment epithelium, associated with poor control of blood glucose, blood pressure and lipid levels (the three main systemic risk factors for diabetic retinopathy and DME).3
The UK prevalence of visual impairment due to DME is estimated at approximately 3% of the adult (aged 18+ years) diabetic population.4 Visual impairment places a substantial socio-economic burden on patients, their caregivers and healthcare systems at large.5 There is, therefore, a strong public health incentive to choose safe therapies that provide increased health gains through improved vision and patient functioning, while offering an acceptable balance between benefits and costs.
Ranibizumab (Lucentis®, Novartis Pharma AG, Switzerland) is a novel agent that is currently licensed for the treatment of visual impairment due to DME.6 Ranibizumab selectively inhibits active isoforms of human vascular endothelial growth factor A (VEGF-A) from binding to its receptors. VEGF-A stimulates growth of new blood vessels and is a major mediator of increased vascular leakage,7–10 mechanisms thought to be associated with retinal damage and progression of DME and the resulting visual impairment.
The Phase III RESTORE trial enrolled 345 patients with visual impairment due to DME and assessed ranibizumab given either as monotherapy or in combination with laser photocoagulation, compared with laser photocoagulation alone. The results showed that ranibizumab alone or in combination with laser provided significantly greater improvements in best corrected visual acuity (BCVA) at 1 year compared with laser therapy alone, with mean average BCVA changes of +6.1 and +5.9 versus +0.8 letters, respectively.11 In addition, health-related quality of life, as assessed using the National Eye Institute Visual Function Questionnaire (NEI VFQ-25), was improved significantly from baseline for both ranibizumab treatment groups compared with laser therapy alone (p<0.05 for composite score and vision-related subscales). RESTORE is ongoing in a 2-year open-label extension phase.
This report summarises the results of a health economic model that was developed based on RESTORE trial data to evaluate the cost-effectiveness of ranibizumab from a UK payer perspective when used as monotherapy or in combination with laser therapy compared with laser therapy alone. The model was developed separately from current assessments of ranibizumab by the UK Health Technology Assessment bodies, such as the National Institute for Health and Clinical Excellence.
Methods
A Markov model was constructed to simulate costs and changes in BCVA over a 15-year period in a hypothetical cohort of patients with DME (figure 1), based on data from the RESTORE trial (in which 87.5% of patients had type 2 diabetes and average baseline glycated haemoglobin was 7.3%). The average age at entry to the model was 63 years, consistent with patient characteristics in RESTORE. The model also assumed the same baseline BCVA distribution, but excluded patients with BCVA >75 letters, consistent with guidance from the ranibizumab summary of product characteristics that such patients may benefit less from treatment than those with baseline BCVA ≤75 letters.6
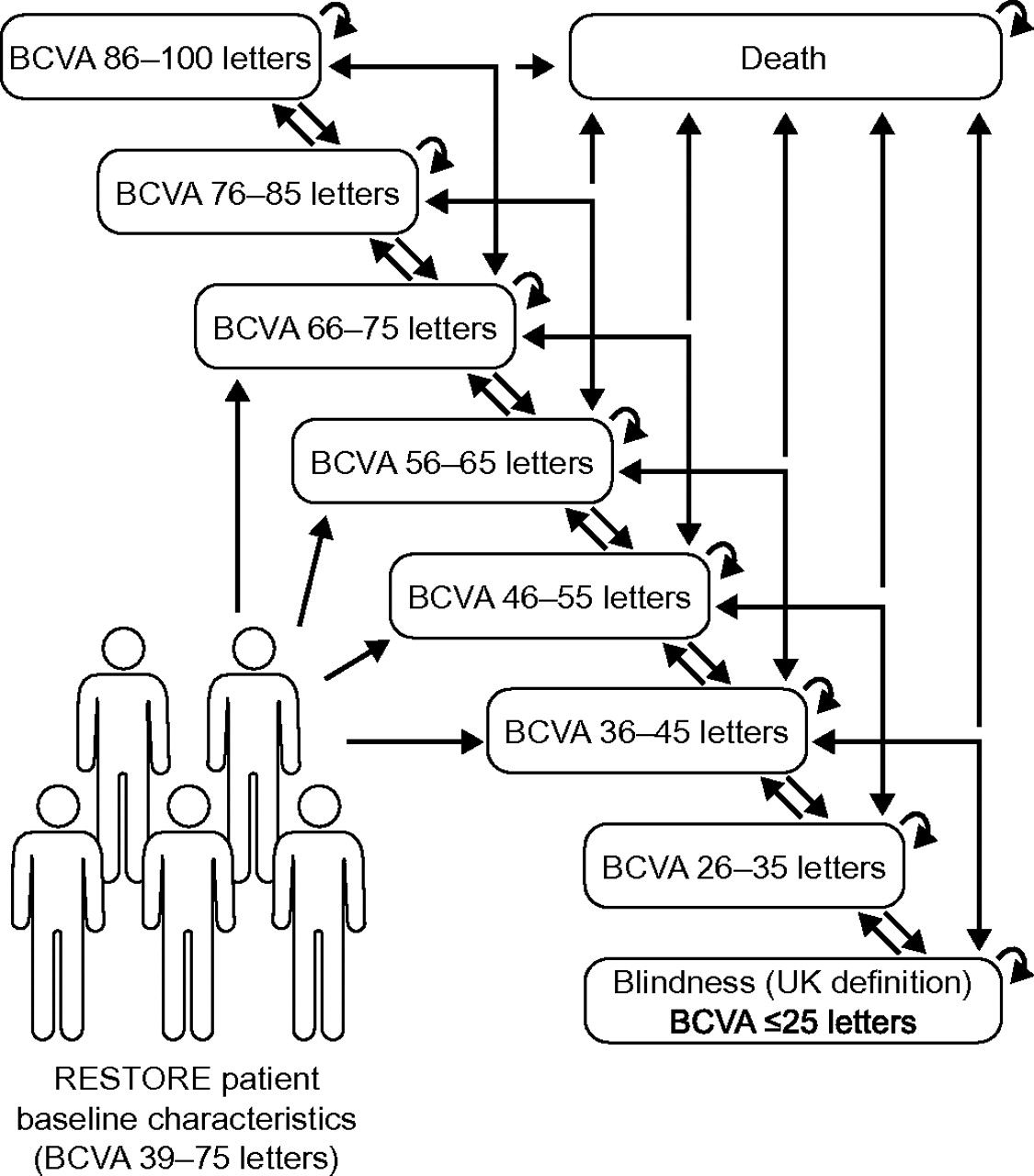
Markov model structure. Health states are defined by best corrected visual acuity (BCVA) in the treated eye. Patients enter the model at treatment start where they are assumed to have BCVA as in RESTORE (>39 letters and ≤75 letters). BCVA is evaluated at 3-monthly intervals. After each cycle, patients may transition to any other health state including death; the probability of moving from health state A to health state B is based on RESTORE data (baseline to month 12) and literature.
The model framework allocated eight linear health states defined by BCVA in the treated eye using a set of 10-letter (two-line) categories (table 1). Movement of patients from one health state to another was determined by transition probabilities that depended on the effectiveness of treatment and natural BCVA changes over time. A 10-letter range was used to categorise health states based on evidence that a 10-letter BCVA score loss is associated with a substantial decline in health-related quality of life (eg, loss of functional ability, increasing dependency, role limitations and impaired mental health).15 Each health state was assigned a quality-of-life index and cost. Costs and outcomes were accrued over 3-month cycles, applying half-cycle corrections. The time horizon in the base case was 15 years; although a lifetime horizon could be justified given the chronic nature of the condition, we selected a more conservative approach for the base case because of the lack of evidence on long-term prognosis.
Utility by BCVA in treated eye
The key inputs and assumptions are summarised in table 2. Patients were assumed to receive ranibizumab treatment in year 1 at the frequency observed in RESTORE. In year 2, patients were assumed to need fewer injections, as observed in the Diabetic Retinopathy Clinical Research Network (DRCR.net) protocol I study (which included patients with comparable baseline demographics to RESTORE).1 A proportionately smaller number of monitoring visits was therefore assumed in year 2. After year 2, laser therapy was assumed to be administered as required in all arms, with no further need for ranibizumab; the assumed number of monitoring visits was further reduced accordingly.
Key model inputs and assumptions
The average BCVA achieved in year 1 was assumed to be maintained during year 2, as was observed in the DRCR.net protocol I study.1 After year 2, all arms of the model followed natural disease history based on 4-year health state transition outcomes modelled from the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) reports.17–19 Transition probabilities were calibrated to adjust for the improvement in diabetes management since the WESDR reports (see Supplementary Methods), and predicted that around 30% of patients would be expected to exhibit a worsening in BCVA of at least 10 letters and 20% of patients would show an improvement of at least 10 letters over a 4-year time horizon (Supplementary table 1).
Treatment discontinuation rates observed in RESTORE were applied to the model in year 1; it was assumed there would be no additional withdrawals from treatment in year 2. Adverse events were assumed to have a negligible impact on the cost-effectiveness of ranibizumab therapy based on the established safety profile of ranibizumab in clinical trials in DME and in wet age-related macular degeneration, an indication for which ranibizumab is also licensed.1 20–22
Mortality was estimated by adjusting general UK population death rates according to the increased RR of death in patients with DME. Mulnier et al estimated an increased mortality (HR 1.93) in a UK type 2 diabetes population relative to patients without diabetes,23 while Hirai et al estimated an HR of 1.27 for death in patients with clinically significant macular oedema (CSME) and diabetes relative to diabetic patients without CSME.24 We calculated a 2.45 RR of death in a DME population by multiplying these two ratios.
Utility scores were calculated based on patient-reported outcomes data from RESTORE (table 2), in which patients completed the EuroQoL (EQ-5D) questionnaire at baseline and months 3, 6 and 12. Individual EQ-5D health scores were converted into utility scores using preferences from a UK population survey;14 mean utility scores were calculated for each health state (table 1). As these states were defined by BCVA in the treated eye, of which 67.2% were the worse-seeing eye at baseline, this method established an association between utility and BCVA changes in the treated eye.
Health state costs included the costs of treatment and monitoring (Supplementary tables 3–6), and the costs associated with blindness (Supplementary table 2). Treatment costs included the costs of ranibizumab (Novartis UK, personal communication) and its administration, laser therapy and investigative procedures. Monitoring costs, including consultation and procedure costs, were estimated from the UK National Health Service Reference Costs.25 Costs of blindness included those incurred by the UK National Health Service for items such as low-vision aids, low-vision rehabilitation, residential or home care, depression and hip fracture/replacement as listed in the costing study by Meads and Hyde.16 Where older cost estimates were used, these were inflated to 2010 prices using the Hospital and Community Health Services index.26 The cost of blindness would be incurred only in patients reaching health states with BCVA ≤35 letters (Snellen ≤6/60) in the better-seeing eye. However, as the study assesses treatment response according to the enrolled eye, the proportion of patients reaching this level within the time horizon of the model is therefore uncertain. As such, the base case model adjusts for the cost of blindness on the basis of treated eyes reaching the BCVA ≤35-letter threshold. As with other model parameters subject to uncertainty, deviations from this assumption were explored in sensitivity analyses (Supplementary table 7).
The main outcome measure was the incremental cost-effectiveness ratio (ICER), expressed as the additional cost per quality-adjusted life-year (QALY) gained by one treatment over another. An annual 3.5% discount rate was applied for future costs and utilities, consistent with the standard UK approach.
Univariate sensitivity analyses assessed the uncertainty around specific data sources by exploring the effects on the ICER of inputs, as shown in table 3. Probabilistic sensitivity analysis assessed the overall uncertainty about the ICER based on variations in individual input parameters; details of the applied distributions and results are provided in Supplementary table 7.
Cost-effectiveness: base case and sensitivity analyses*
Results
The model predicted that after 1 year, a greater proportion of patients treated with ranibizumab monotherapy or combination therapy would have BCVA >65 letters (Snellen score >6/18) compared with patients treated with laser monotherapy (48% and 47%, respectively, versus 38% in the laser arm) (figure 2). After 15 years, the proportion with severe visual impairment in the treated eye (BCVA <35 letters, Snellen <6/60) was predicted to be 12% and 13% in the ranibizumab monotherapy and combination therapy groups, respectively, versus 19% in the laser group.

{kind=link}
{kind=link}
Modelled distribution by health states after (A) 1 and (B) 15 years. BCVA, best corrected visual acuity.
Ranibizumab monotherapy was associated with an incremental gain of 0.17 QALY and cost of £4 191, corresponding to an ICER of £24 028 per QALY gained relative to laser monotherapy (table 3). Combination therapy provided an incremental gain of 0.13 QALY over laser monotherapy for an incremental cost of £4 695, leading to an ICER of £36 106 per QALY gained.
Univariate sensitivity analyses showed that the model was stable and that ICERs were most sensitive to changes in the number of injections and time horizon (table 3). Using utilities elicited by Lloyd et al12 and Brown et al13 in patients with diabetic retinopathy led to greater QALY gains and lower ICERs for ranibizumab monotherapy or combination therapy relative to laser monotherapy. Probabilistic sensitivity analysis confirmed the model's robustness (Supplementary figure 1). Assuming a willingness-to-pay threshold of £30 000 per QALY gained, the probability that ranibizumab monotherapy would be cost-effective relative to laser monotherapy was estimated to be 64% (Supplementary figure 2); the corresponding probability for combination therapy relative to laser monotherapy was 42%.
Discussion
This is the first study to evaluate the cost-effectiveness of an anti-VEGF agent for the treatment of patients with DME causing visual impairment. Our economic model, which was based on data from the RESTORE clinical trial, shows that ranibizumab monotherapy provides superior improvements in visual acuity and is cost-effective relative to the current standard of care, laser photocoagulation. Ranibizumab monotherapy was associated with an ICER of £24 028 per QALY gained relative to laser therapy alone, a value within the willingness-to-pay threshold of £30 000 per QALY gained that has generally been considered cost-effective in the UK. The results of our model may be applicable to a broad spectrum of patients with visual impairment due to DME, as the RESTORE trial showed consistent efficacy of ranibizumab therapy across patient subgroups based on a range of demographic and disease characteristics.
The cost-effectiveness of combined ranibizumab and laser therapy was less favourable than that of ranibizumab monotherapy (ICER £36 106 per QALY gained relative to laser therapy alone). While this in part reflects higher treatment costs, combination therapy also provided a lower predicted QALY gain than ranibizumab monotherapy (0.13 vs 0.17 QALY over the 15-year time horizon in the base case). A possible explanation for these results is the observation in RESTORE that combination therapy provided smaller improvements in BCVA in patients who had received prior laser therapy than those who had not (4.7 vs 6.9 letters gained, respectively).11 In RESTORE, the proportions of patients who received prior laser therapy were 52% (ranibizumab monotherapy), 47% (combination therapy) and 43% (laser therapy).
Sensitivity analyses showed that the model results were robust to reasonable alterations in inputs and assumptions; ICERs were particularly sensitive to changes in the number of ranibizumab injections and the time horizon of the model. The base case assumed an average of 10 ranibizumab injections over 2 years, based on data from the DRCR.net protocol I study.1 Ranibizumab monotherapy remained cost-effective (ICER below £30 000 per QALY gained) up to a total of 13 injections. Increasing the number of injections beyond 13 resulted in an ICER outside the generally accepted threshold, emphasising that additional injections beyond 2 years of treatment will be an important cost driver. However, the current model is conservative in that it includes incremental costs for additional injections beyond year 2, but assumes no incremental benefit. The possible need for re-treatment beyond 2 years remains speculative; forthcoming data from the 2- and 3-year RESTORE follow-up and the DRCR.net 5-year data will improve our understanding of the likely duration of treatment. Longer time horizons would be expected to lead to improved cost-effectiveness of ranibizumab, because the benefits of improved vision accrue over time whereas treatment costs are incurred immediately once treatment is initiated.
We have identified only one previously reported cost-effectiveness study of interventions for DME. Sharma et al modelled the cost-effectiveness of laser therapy alone for DME,27 comparing early and deferred laser treatment with no treatment based on 3-year outcomes from the Early Treatment Diabetic Retinopathy Study.28 The model included health states defined by BCVA and applied a 40-year time horizon based on a population with a mean age of 47 years. Over this time horizon, laser treatment was predicted to provide a gain of 0.236 QALY and was considered highly cost-effective for DME relative to no treatment. Our results cannot be compared directly with the Sharma et al27 study because RESTORE did not include a ‘no treatment’ arm; moreover, our model applied a 15-year time horizon from a baseline age of 63 years, consistent with RESTORE. However, if a baseline age of 47 years and time horizon of 40 years were applied to our model, as in the Sharma et al27 model, the RESTORE model would predict a 0.26 QALY gain and an ICER of £10 412 for ranibizumab monotherapy relative to laser therapy alone. This suggests that the cost-effectiveness of ranibizumab would be higher in patients with DME who were younger than the average in RESTORE (63 years) because of their longer life expectancy.
Several methodological considerations should be noted. While treatment effectiveness was based on 1-year data from RESTORE, we projected long-term changes in BCVA using the best available clinical evidence. For year 2, the DRCR.net protocol I study supported the assumption that BCVA at 1 year was maintained on average to 2 years.1 BCVA changes in years 3–15 were based on reported progression in the WESDR study, which demonstrated a gradual decline in vision over time in DME. The rate of decline in BCVA was reduced by adjustment using data from both the Diabetes Control and Complications Trial and UK Prospective Diabetes Study to account for a less intensive systemic diabetes management regimen in the past relative to current practice.29–32 Sensitivity analysis showed that these assumptions had only a minor impact on the model results.
Utilities were estimated from the BCVA of treated eyes in RESTORE, irrespective of whether this was the better-seeing or worse-seeing eye. This approach links utility values directly to the eye receiving the intervention. The RESTORE study protocol required the worse-seeing eye to undergo intervention unless there was a medical contraindication; 32.8% of treated eyes were the better-seeing eye at baseline, and 37.3% were the better-seeing eye at 12 months. Using the better eye as reference is supported by quality of life studies in vision-related conditions, which have shown that the better eye is the major driver of overall quality of life and patient functioning.33 Indeed, patient-preference studies have shown that the utility gains associated with treating the worse-seeing eye are uncertain, even though good vision in two eyes confers better quality of life than good vision in only one eye.34 As expected, subdividing the elicited utilities in RESTORE by better-seeing or worse-seeing eye showed that patients being treated in the better-seeing eye reported lower utility at a given level of BCVA than those treated in the worse-seeing eye. Nevertheless, utility measured in patients treated in the worse-seeing eye demonstrated significant sensitivity to variation in the BCVA in the treated eye, comparable with that of patients treated in the better-seeing eye. Unfortunately, the small sample of RESTORE patients in each BCVA health state meant that the resulting utility functions were not sufficiently robust to allow separate cost-effectiveness analysis by better-seeing or worse-seeing eye. It should also be stated that the option of not treating visual impairment in a better-seeing eye is not an ethical stance.
We could not find published utility estimates from specific populations with DME. We performed sensitivity analysis using utilities reported in two studies based on populations with diabetic retinopathy (which includes a wider population than DME).12 13 Lloyd et al reported utilities elicited by the general population, while Brown et al reported utilities elicited by patients. This showed that applying the Lloyd et al12 utilities to the model greatly improved the cost-effectiveness of ranibizumab monotherapy, leading to a larger incremental gain of 0.22 QALY and a lower ICER of £19 238 per QALY gained relative to laser therapy alone. Applying the Brown et al13 utilities also increased the QALY gain with ranibizumab and led to an ICER of £21 953 per QALY gained for ranibizumab monotherapy versus laser therapy alone. The fact that the RESTORE utilities are less sensitive to BCVA decline may simply reflect the fact that a majority of the reference eyes in RESTORE were worse-seeing, while all reference eyes in the Lloyd et al12 and Brown et al13 studies were better-seeing.
Limitations of this analysis should be considered. First, we modelled treatment of unilateral DME based on RESTORE data, but did not estimate the cost-effectiveness of treating bilateral DME. While 82.8% of patients in RESTORE had signs of bilateral DME at baseline, the proportion of patients who would have become eligible for treatment because of vision impairment in their fellow eye was not known. Treatment of both eyes may be relevant in many patients with bilateral DME, but there is a lack of evidence for the additional utility benefit of treating the fellow eye. Uncertainty also exists regarding the cost consequences of treating both eyes, where total cost is not likely to double given the possibility of achieving economies of scale from shared categorical spending, such as administrative and monitoring costs. An additional limitation was that the model assumed the cost of blindness would be incurred in patients reaching health states with BCVA ≤35 letters (Snellen ≤6/60) in the treated eye.
There is also uncertainty inherent in working with published results of studies, as was necessary for incorporating the DRCR Network Protocol I results, as opposed to using patient-level data. While analysis using patient level data is clearly preferable, incorporation of findings from studies in addition to RESTORE, such as the highly comparable DRCR study, provide very useful data for answering critical questions relating to clinical practice in a broad spectrum of patients with DME. It should be noted, however, that some subgroups, such as patients with the poorest glycaemic control (high glycated haemoglobin), were excluded from these trials.
In conclusion, the results of our economic model show that ranibizumab monotherapy is cost-effective relative to laser therapy alone in the treatment of DME causing visual impairment, while combined ranibizumab and laser therapy may be cost-effective depending on patient characteristics. The cost-effectiveness of ranibizumab monotherapy or combination treatment is expected to be higher in younger patients who have a longer life expectancy. These findings have important practical implications, given the high socio-economic burden of DME and the need for new, cost-effective treatments that reduce long-term progression to blindness. Ongoing studies, such as the RESTORE extension, will provide additional clarification of current uncertainties such as the need for ranibizumab injections after 2 years and the likelihood of recurrent DME.
Acknowledgments
The authors acknowledge the editorial support of Dr Richard White (Oxford PharmaGenesis Ltd) in collating the comments of the authors and finalising the manuscript for submission.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study was supported by Novartis Pharma AG, Basel, Switzerland.
Competing interests PM has received a consultancy fee from Novartis Pharma AG, Pfizer, Solvay and Allergan. He has also been paid lecture fees/honoraria by Novartis Pharma AG, Pfizer, Solvay and Allergan. LA has received unrestricted grants from Novartis Pharma AG. SKT is an employee of Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. KG is an employee of Novartis Pharmaceuticals, Frimley, UK. RH is an employee of Novartis Pharma AG, Basel, Switzerland and a Novartis shareholder. MK and HO were employed as consultants by Novartis Pharma AG for this study. MG was formerly employed by Novartis Pharma AG, Basel, Switzerland; current affiliation Amgen Inc., Thousand Oaks, CA, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance