Article Text

Abstract
Purpose To determine the relationship between retinal ischaemia and the presence of macular oedema (DMO) in patients with diabetic retinopathy (DR) using ultra-widefield fluorescein angiography (UWFA) imaging.
Methods A retrospective review of 122 eyes of 70 treatment-naïve diabetic patients who underwent diagnostic UWFA using the Optos 200Tx imaging system. Two independent, masked graders quantified the area of retinal ischaemia. Based on clinical examination and optical coherence tomography (OCT), each patient was given a binary classification as either having DMO or no DMO. McNemar's test (with Yates' correction as indicated) and a two-sample test of proportions were used to determine the relationship between DMO and ischaemia for binary and proportional data, respectively. Linear and logistic models were constructed using generalised estimating equations to test relationships between independent variables, covariates and outcomes while controlling for inter-eye correlation, age, gender, haemoglobin A1c, mean arterial pressure and dependence on insulin.
Results Seventy-six eyes (62%) exhibited areas of retinal ischaemia. There was a significant direct correlation between DMO and peripheral retinal ischaemia as seen on UWFA (p<0.001). In addition, patients with retinal ischaemia had 3.75 times increased odds of having DMO compared with those without retinal ischaemia (CI 1.26 to 11.13, p<0.02).
Conclusion Retinal ischaemia is significantly correlated with DMO in treatment-naïve patients with DR. UWFA is a useful tool for detecting peripheral retinal ischaemia, which may have direct implications in the diagnosis, follow-up and treatment such as targeted peripheral photocoagulation.
- Ultra-wide field imaging
- fluorescein angiography
- diabetes
- diabetic retinopathy
- diabetic macular oedema
- retina
- epidemiology
- retina
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Ultra-wide field imaging
- fluorescein angiography
- diabetes
- diabetic retinopathy
- diabetic macular oedema
- retina
- epidemiology
- retina
Introduction
Diabetic retinopathy (DR) is one of the leading causes of blindness among adults, accounting for approximately 5% of global blindness. In parts of the Americas, Europe and the Western Pacific, DR is responsible for as much as 17% of the total blindness caused by eye disease.1 The risk of developing significant visual loss due to DR can be significantly diminished with proper control of systemic disease and prompt treatment of eye pathology.1
Diabetic macular oedema (DMO), in particular, is a major contributor to vision loss among patients with DR.2 More than 25 years ago, the Early Treatment of Diabetic Retinopathy Study (ETDRS) established guidelines for identifying clinically significant macular oedema (DMO) and proved that treatment with focal laser photocoagulation decreased risk of moderate visual loss, increased the chance of moderate visual gain and reduced retinal thickening.3 While ETDRS remains the seminal study on DMO, additional awareness of diabetic pathology, the advent of new pharmacology and improvements in retinal imaging technology have allowed us to expand upon our understanding and treatment of DMO.
Ischaemic changes and microvascular pathologies have long been hypothesised to play a role in the development of DMO. In DR, ischaemia stimulates the production of vascular endothelial growth factor (VEGF),4 which can lead to the breakdown of blood-retinal barriers, and may cause DMO through an increase in retinal vessel permeability.5 Anti-VEGF drugs have proven efficacious in the treatment of DMO, even in cases not responding to laser photocoagulation.6 The success of anti-VEGF therapy lends support to the thinking that retinal ischaemia and DMO are associated, but traditional retinal imaging of ischaemia makes it difficult to study this association.
Retinal ischaemia is best characterised with fluorescein angiography (FA). Traditional FA employs retinal photography that is able to view approximately 30° of the retina at one time. The ETDRS developed the seven-standard fields (7SF) protocol in which seven photographed areas of the retina were combined to give nearly 75° of visualisation. With the advent of ultra-widefield fluorescein angiography (UWFA), as with the Optos 200Tx imaging system (Optos PLC, Dunfermline, Scotland), it is now possible to view up to 200° of retina in a single photograph. Initial small-scale studies have shown that UWFA is more useful in detecting capillary non-perfusion in patients with DMO than other methods with a more limited degree of retinal imaging.7
The principle aim of this study was to better characterise the relationship between the area of retinal ischaemia as measured with UWFA and the presence of DMO in patients with DR. We hypothesise that peripheral vascular changes can influence the posterior retina and that patients with retinal ischaemia are at an increased odds of having DMO. Given the extent of retinal thickening in patients with DMO can be determined with cross-sectional retinal visualisation in optical coherence tomography (OCT),8 this study also evaluated whether the area of retinal ischaemia was correlated with the severity of DMO as evaluated by OCT.
Methods
We present a retrospective review of all patients with DR over a two-and-a-half-year time period (October 2007 to January 2010) at a single institution who underwent UWFA using the Optos 200Tx imaging system (Optos PLC, Dunfermine, Scotland). The Weill Cornell Medical College–New York Presbyterian Hospital Institutional Review Board (IRB) approved this study according to local and national IRB guidelines. Health Insurance Portability and Accountability Act compliance was maintained. Care of the patients in this study was in accordance with the Declaration of Helsinki and all federal and state laws.
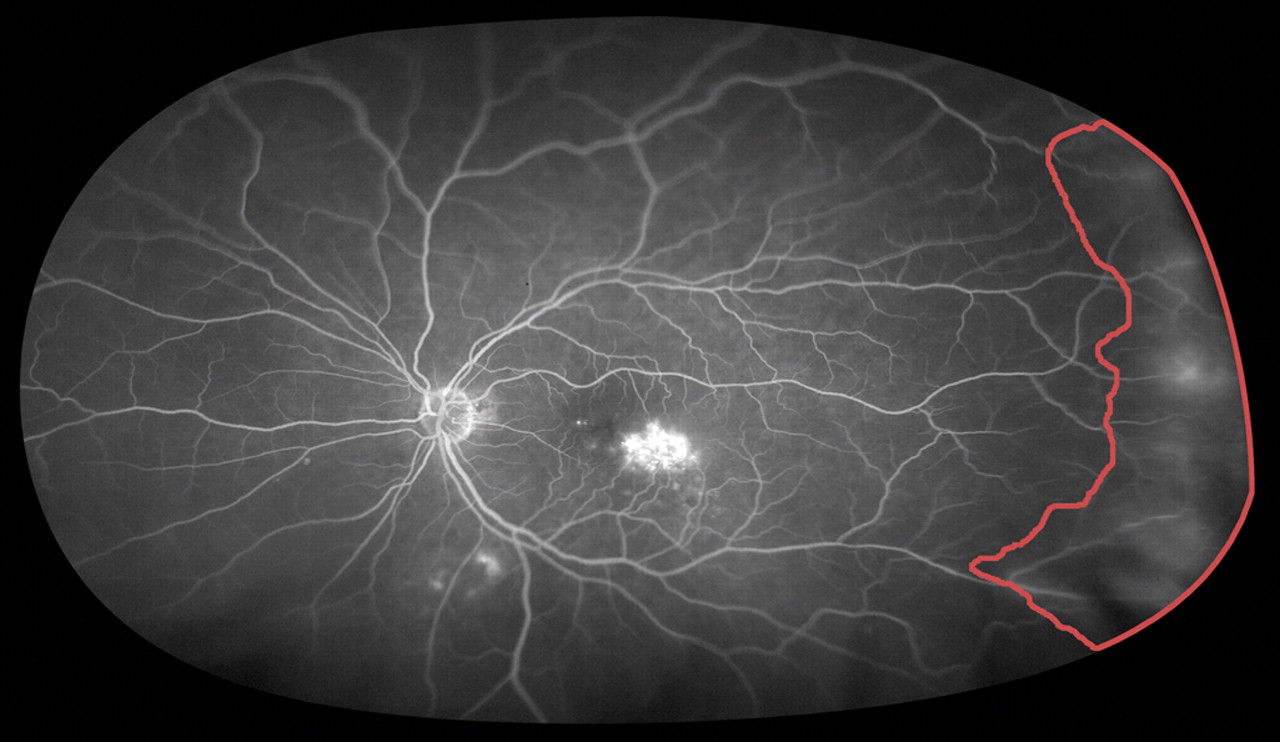
All UWFA images were collected according to standard clinic protocol. Patients received an intravenous injection of 5 cc of sodium fluorescein 10%. A representative image of each eye was captured after complete arteriovenous filling, using the Optos V2 Vantage Review Software. Images were compressed into high quality jpeg files, transferred to Adobe software and evaluated by two independent trained masked graders for the presence of retinal ischaemia. For the purpose of this study, retinal ischaemia was defined as angiographically visually significant hypofluorescence of an area of at least one disc diameter (representing retinal non-perfusion or capillary dropout) or areas of microvascular pathology (multiple microaneurysms, intraretinal microvascular anomalies and significant perivascular leakage) with associated capillary pruning of at least one disc diameter. Given that delineation of ischaemic retina on FA can be challenging, graders were thoroughly trained prior to analysing images for the study in using various controls in Adobe software (ie, brightness, contrast, level, zoom) and how to ignore eyelashes and peripheral blurring that be mistaken for non-perfusion. Preliminary sample images were reviewed together and remaining areas of disagreement were reviewed with the senior author. Once good correlation was documented with sample images, the graders independently analysed the 236 UWFA images included in the study. A total retinal surface area, as well as the area of retinal ischaemia was measured in pixels (figure 1A,B). The data was then averaged between the two graders to obtain final values. Lin correlation coefficients were calculated and >0.80 was considered sufficient to prove a strong inter-grader correlation. Had any data fallen below this value, a third grader would have been used to resolve discrepancies; however, this step was unnecessary. The proportion of ischaemic to total visible retinal area was calculated for each image.

(A): A sample ultra-widefield fluorescein angiogram. Retinal ischaemia is outlined in red. To obtain the proportion of ischaemic to total retina, the pixels enclosed by the outlined area were divided into the total pixels of the image. (B): A close-up view of the superonasal quadrant of (A) showing the difference between ischaemic (I) and non-ischaemic (N) retina. Retinal ischaemia is defined as angiographically visually significant hypofluorescence (capillary dropout) or areas of significant capillary pruning associated with microvascular pathology (microaneurysms, intraretinal microvascular anomalies, perivascular leakage). Note that the ground glass appearance and normal capillary architecture of the non-ischaemic retina differs from the hypofluorescent areas of non-perfusion and ischaemic vasculature highlighted in red. This figure is produced in colour in the online journal—please visit the website to view the colour figure.
For each diabetic patient who received UWFA during the period of interest, it was noted whether a clinical diagnosis of DMO was made in the chart during dilated fundoscopy. The following information was also obtained from the electronic medical record: age, gender, haemoglobin A1c, mean arterial pressure (MAP) and dependence on insulin. MAP and haemoglobin A1c values were used only if they were within 3 months of the UWFA image collection. If a patient presented for UWFA on multiple occasions, the earliest clinical visit was evaluated. Exclusion criteria consisted of the following: eyes that had undergone retinal surgery or laser treatment, eyes that had received intravitreal injections, eyes with concomitant non-diabetic pathology (including artery and vein occlusions, uveitis, sickle cell retinopathy) as identified by either angiography or clinical history, eyes with >5 disc diameters of chorioretinal scarring, eyes with tumours, eyes that were poorly photographed due to significant media opacities (vitreous haemorrhage, cataract) or poor patient cooperation (eyelids covering at least one quarter of retinal image).
Additionally, where available, OCT (Heidelberg Spectralis HRA+OCT, Heidelberg Engineering, Germany) images were analysed to detect the presence and extent of DMO. OCT images were only considered relevant if they were collected on the same day as the UWFA images. Values for central macular thickness (1 mm diameter, centred on the fovea), and the central macular volume (both 1 mm and 3 mm diameters, centred on the fovea) were obtained using Heidelberg Eye Explorer software in accordance with ETDRS protocol.
All analyses were conducted using Stata 11/IC software (StataCorp LP, College Station, Texas, USA). McNemar's test and a two-sample test of proportions were used to determine the relationship between DMO and ischaemia for binary and proportional data, respectively. Associations of binary, continuous and proportional dependent variables with covariates and predictors of interest were modelled using generalised estimating equations to control for inter-eye correlation among patients. All statistical tests were two-sided with a 0.05 level of significance.
Results
A total of 236 UWFAs from 118 diabetic patients were reviewed. One hundred and fourteen eyes were excluded from the study (table 1) leaving a total of 122 treatment-naïve eyes of 70 diabetic patients. Patients ranged in age from 18 to 87 years (median 60 years). Eyes being evaluated were initially separated into two categories based on electronic medical record chart diagnoses: DMO (24 eyes) or no DMO (98 eyes). The median age of patients with at least one eye with DMO was 58 years, and 50% of these patients were male. The median age of patients with no DMO in either eye was 60 years, and 41% were male.
Exclusion criteria and number of excluded eyes
Each eye was also evaluated for presence or absence of retinal ischaemia using UWFA images. Out of 122 eyes, 76 demonstrated some degree of ischaemia. The binary classification of DMO was compared with the binary classification of ischaemia (table 2) and the two were found to be significantly related (p<0.001). Furthermore, the odds of having DMO in patients with retinal ischaemia were calculated (table 3). This analysis adjusted for several covariates, including MAP and haemoglobin A1c (if available within 3 months of UWFA) as well as age. Eyes with retinal ischaemia had significantly higher odds of having DMO (OR=3.75, 95% CI 1.26 to 11.13, p=0.02). There was no significant association between odds of DMO and haemoglobin A1c (OR=1.34, 95% CI 0.61 to 2.93, p=0.47), MAP (OR=1.00, 95% CI 0.94 to 1.06, p=0.99), or age (OR=1.01, 95% CI 0.96 to 1.07, p=0.68) on univariable analysis. However, among patients with demonstrable ischaemia on UWFA, haemoglobin A1c level was significantly associated with the proportion of retina found to be ischaemic (ß=0.34, 95% CI 0.07 to 0.61, p=0.01) (figure 2).
Diabetic macular oedema and retinal ischaemia are significantly related
There are significantly increased odds of macular oedema in patients with evidence of retinal ischaemia

An analysis of patients with demonstrable ischaemia on ultra-widefield fluorescein angiogram. Note the strong correlation between the value of haemoglobin A1c and the proportion of retinal ischaemia to total retina (‘ischaemic index’) in this group of patients.
Although binary classification of ischaemia was significantly associated with presence or absence of DMO, we did not find a significant relationship between DMO and the proportion of ischaemic retina (p=0.88). Furthermore, among the 18 eyes for which there were both UWFA and OCT images, there was no significant relationship between proportion of ischaemic retina and extent of DMO based on OCT image analysis (r=0.05, p=0.86).
Discussion
Since first described by Friberg and Forrester in 2004,9 UWFA has proven to be a reliable method of retinal evaluation, having favourable sensitivity and specificity compared with other traditional methods.10–12 In some applications, including identification of diabetic pathology, it has proven to be superior to traditional methods, including 7SF. A recent comprehensive study of efficacy in detection of diabetic pathology found that UWFA was able to demonstrate retinal non-perfusion and neovascularisation in 10% of eyes that would have been missed by 7SF.13
To our knowledge, this study is one of the first and largest to use UWFA to evaluate retinal ischaemia and identify its relationship with DMO. This study also examined whether UWFA can be used as a complement to OCT to determine whether the degree of macular thickening correlates with the proportion of retinal ischaemia.
We demonstrate that patients with retinal ischaemia have a 3.75 times greater chance of having DMO. This observation has several important implications. First, it lends support to the growing data suggesting that retinal ischaemia and release of vasoproliferative growth factors play a role in the pathogenesis of DMO. Several recent studies, including the BOLT and PACORES study groups, have shown that anti-VEGF therapy is effective in treating DMO, even in cases where macular laser therapy has failed.14–16 In that retinal ischaemia is most likely driving the release of VEGF, and that patients with retinal ischaemia have a 3.75 times greater chance of developing DMO, detection and monitoring of peripheral retinal ischaemia could play an important role in the management of patients with diabetic retinopathy. For example, patients with retinal ischaemia on UWFA may necessitate closer monitoring and earlier follow-up than patients with no evidence of retinal ischaemia.
A second implication of our study is that new treatment modalities, such as targeted retinal photocoagulation (TRP) may prove efficacious in treating DMO. In early studies evaluating patients with proliferative diabetic retinopathy, it has been suggested that TRP may replace pan-retinal photocoagulation by directing therapy specifically at ischaemic parts of the retina to precisely eliminate the source of VEGF, thus minimising the sequelae of pan-retinal photocoagulation.17 In many of the eyes that we analysed, DMO was present despite minimal posterior diabetic pathology. In some of these eyes, UWFA was able to demonstrate anterior areas of retinal ischaemia (figure 3). In that the pathogenesis behind the formation of DMO is most likely related to peripheral retinal ischaemia in these cases, it would be reasonable to consider treating DMO by using UWFA and TRP. In combination with macular laser and anti-VEGF therapy, TRP could prove to be important in the growing arsenal of treatment modalities for DMO.

{kind=link}
{kind=link}
{kind=link}
An ultra-widefield fluorescein angiogram with diabetic macular oedema and a peripheral area of ischaemia. Targeted photocoagulation treatment of this area could possibly prove to be another treatment choice if traditional methods were not efficacious.
Interestingly, our study failed to detect an association between the amount of retinal ischaemia and the degree of macular thickening. While this might in part be attributable to the small number of patients who had both OCT and UWFA images performed at the time of their initial visit, it might also suggest that the degree of retinal ischaemia is not related to the extent of macular thickening. It is possible that only a small amount of retinal ischaemia is necessary for the causal factors of DMO to develop, and the macular thickness may be more attributable to local, structural and micro-anatomical factors than to the extent of released VEGF. Additional studies would be needed to explore this relationship further. Also, it was also noted that the proportion of retinal ischaemia was significantly related to the value of haemoglobin A1c (figure 2), but not with the presence of DMO. This could suggest that both DMO and ischaemia are related to the pathophysiology of diabetes, but by different mechanisms. Along with evaluating whether there is a direct association between ischaemia and DMO, it would be valuable to examine whether there is a threshold level of ischaemia at which DMO is induced.
We recognise there are limitations to the conclusions that can be drawn from our study. Although we attempted to use all UWFAs in the two-and-a-half-year time period, there was likely a significant selection bias given that physicians had multiple options of obtaining fluorescein angiograms in our clinic, only one of which was the Optos system. Given the retrospective nature of our study and the limited time span in which the study was conducted, we realise that not all results are generalisable. However, the large number of patients included in the study helps to mitigate this issue. While this is, to our knowledge, the largest study examining the correlation between retinal ischaemia and DMO, further studies with an increased number of patients would enhance our findings, and prospective trials could help validate these potential applications of UWFA in clinical practice. Additionally, we realise that measurements of a three-dimensional eye using a two-dimensional system are imprecise, and it is likely that peripheral pathology is over-represented. While not trivial, this discrepancy would not significantly alter the conclusions that can be drawn from our data. Finally, while identifying the presence of retinal ischaemia on UWFA imaging is fairly straightforward, variations in image quality could lead to some variability in quantifying the area of ischaemic retina in each image. These limitations were minimised by our large sample size and the use of two independent reviewers to evaluate each image.
Overall, the findings of this study suggest that there may be a role for UWFA in assessing retinal changes associated with DMO. UWFA may serve as a valuable tool for identifying diabetic patients at risk of developing DMO, for guiding management and follow-up protocols, and for potential new treatment options. As DMO contributes significantly to vision loss in patients with diabetes, the possibility of using UWFA to develop earlier and more precise detection and treatment strategies for DMO is encouraging.
References
Footnotes
Funding The study was made possible in part by the generous support of a departmental Research to Prevent Blindness grant. The ophthalmology department at Weill Cornell has received research funding from the manufacturer of the ultra-widefield imaging device (Optos, PLC). However, the data and analysis presented in this study has no relationship to that research funding.
Competing interests SK serves as a consultation to Optos, PLC. No additional competing interests declared.
Ethics approval This study was approved by the Weill Cornell Medical College–New York Presbyterian Hospital institutional review board (IRB) according to local IRB guidelines. Health Insurance Portability and Accountability Act (HIPPA) compliance was maintained. Care of the patients in this study was in accordance with the Declaration of Helsinki and all federal and state laws. Because the study is a retrospective analysis with no personal medical information or personal identifiers, no individual consent was sought.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data available on request from SK; szk7001{at}med.cornell.edu