Article Text

Statistics from Altmetric.com
Intractable diplopia occurs in approximately 0.8% of patients following strabismus surgery, with considerable detriment to visual quality of life. Long-term therapeutic occlusion is required to permit functional vision.
Black intraocular lens (IOL) implantation is an effective therapeutic option associated with high rates of postoperative satisfaction.1 Black IOL implantation entails a cost to the public sector or patient but this may be offset by long-term clinical and social benefits and fewer hospital visits.
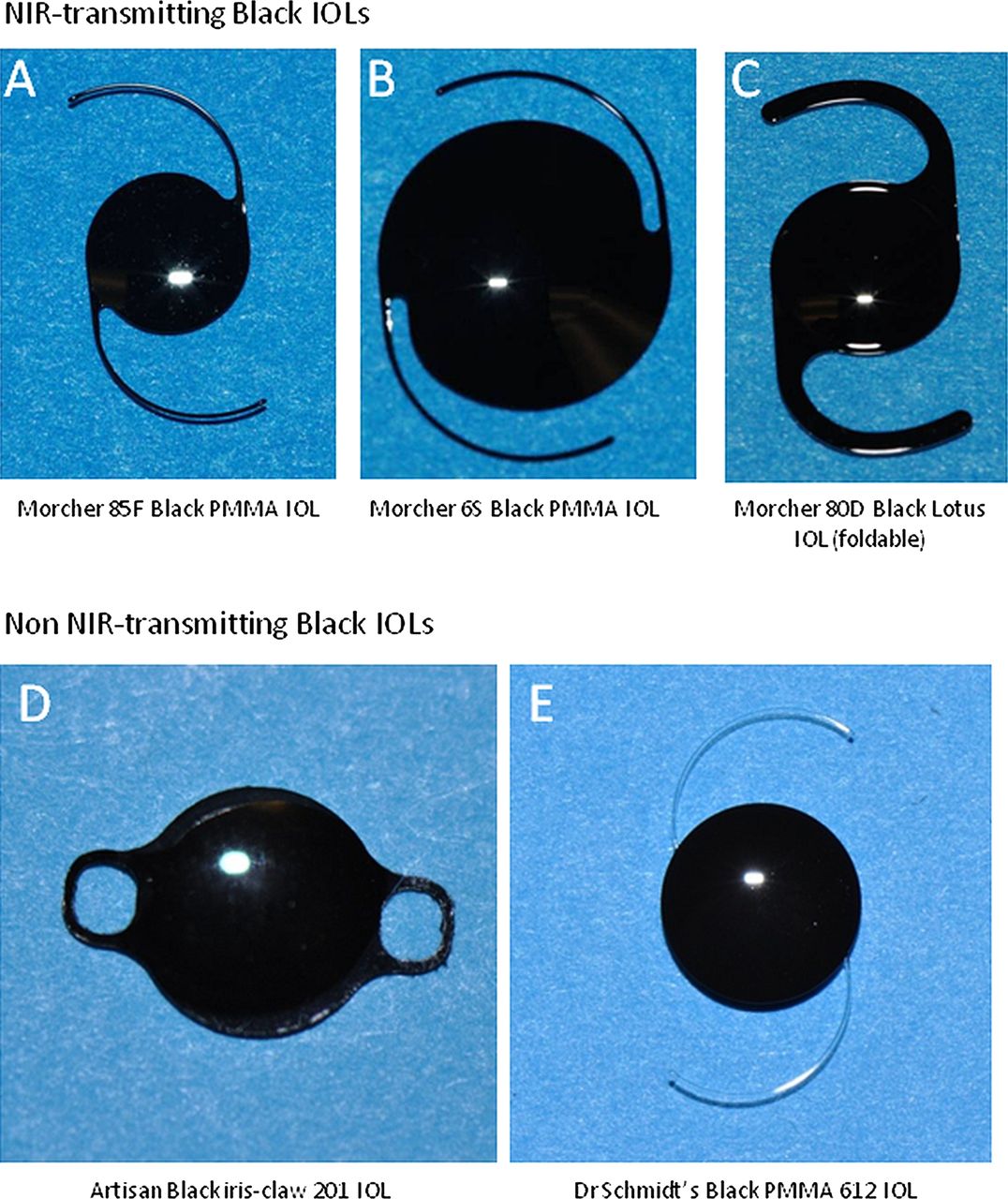
A distinction has emerged between black IOLs that transmit near-infrared (NIR) light and those producing total occlusion of all wavelengths of light (figure 1).2 Morcher black IOLs transmit NIR light exponentially from 720 nm, with 100% transmission over 820 nm, permitting posterior segment imaging with scanning laser ophthalmoscopy (SLO) and optical coherence tomography (OCT).2 This property offers a distinct clinical advantage; SLO/OCT may detect life-threatening retinal and optic nerve diseases, such as choroidal melanoma.2
{kind=link}
Black IOLs in clinical use. Near-infrared (NIR)-transmitting black IOLs: (A) 85F PMMA IOL (6 mm optic, 12 mm overall), (B) 6S PMMA IOL (10 mm optic, 12 mm overall), (C) 80D PMMA IOL (6 mm optic, 13.5 mm overall). All NIR-transmitting Black Lotus 80D PMMA IOL are manufactured by Morcher GmbH, Stuttgart, Germany. Non NIR-transmitting black IOLs: (D) Artisan Black iris-claw IOL (201, polycarbonate, 5.4 mm optic 8.5 mm overall, manufactured by Ophtec BV, Groningen, Netherlands), (E) Black PMMA IOL (612, 6 mm optic, 12 mm overall, manufactured by Dr Schmidt Intraocularlinsen, Sankt Augustin, Germany).
The intended benefit of black IOL implantation is occlusion of light. Enigmatic perception of light across NIR-transmitting black IOLs has been reported widely without any consensus on the mechanism of light perception.1 ,3–5 Four hypotheses have been suggested: (1) Perception of light by long-wavelength, L-cone photoreceptors due to NIR light transmission across Morcher black IOLs2 ,5 (2) Para-optical light leakage in patients with large scotopic pupil diameters,4 (3) Light transmission across the intact sclerochoroidal tunic,4 (4) Non-organic light perception.
Retrospective examination of all black IOL case series reported in the literature (table 1) strongly supports the hypothesis of NIR light perception across NIR-transmitting black IOLs as the primary mechanism underlying treatment failure—defined as troublesome persistence of light perception or diplopia despite black IOL implantation.
Evidence for light perception through NIR-transmitting black IOLs
Twenty-three patients have been reported across four case series, which document preoperative and postoperative visual acuities of patients implanted with NIR-transmitting black IOLs1 ,3–5 (table 1). Twenty-one patients (91%) recorded light perception vision through the black IOL postoperatively.
Two patients experienced complete occlusion of light after NIR-transmitting black IOL implantation4; both patients had optic neuropathies documented preoperatively (compressive and demyelinating, respectively). Optic neuropathies are associated with loss of red–green chromatic discrimination due to effects on parvocellular pathways representing long-wavelength cone photoreceptors6; such patients are unlikely to perceive long-wavelength NIR light.
Clinical observations further discount the alternative hypotheses of light perception following black IOL implantation. Light perception has been reported in a patient with formal scotopic pupillometry (6.5 mm pupil) despite implantation of a NIR-transmitting black IOL with a 10 mm occlusive optic (figure 1B). This observation makes para-optical light transmission highly unlikely.
We have experience of a patient with chronic, debilitating light perception despite implantation of an NIR-transmitting black IOL, who underwent secondary implantation of a NIR-blocking Artisan iris-claw IOL (figure 1D) fixed over the pupillary margin with enclavation. This patient recorded no light perception postoperatively, discounting the hypothesis of light penetrating the intact sclerochoroidal tunic (Yusuf et al, unpublished). There is no evidence for a non-organic aetiology as a basis for light perception in these case series.
The recent discovery of NIR-transmission across some black IOLs in clinical use2 may clarify the unusual observations in clinical reports that preceded it. Establishing the mechanism of light perception in such cases is critical to preventing and managing treatment failure. The mechanism of light perception in patients with NIR-transmitting black IOLs is stimulation of L-cone photoreceptors in NIR-rich light environments such as incandescent and solar light, provided the stimulus is sufficiently bright. An 850 nm light-emitting diode (LED) (Osram GmbH, Munich, Germany) used in our previous studies is visible to the unaided eye, yet falls outside the visible range (380–740 nm).2
This insight may inform the design of an optimal black IOL occlusive to all light wavelengths below 820 nm—minimising light perception—but permitting SLO/OCT imaging of the posterior pole (SLO/OCT superluminescent diodes operate at 820–870 nm).
Patients undergoing NIR-transmitting black IOL implantation must be counselled that perception of light is to be expected postoperatively during informed consent. The presented evidence suggests that light perception following NIR-transmitting black IOL implantation is the rule, not the exception.
Acknowledgments
Stuart N. Peirson's research is funded in part by the Wellcome Trust.
Footnotes
-
Contributors IHY, SNP and CKP wrote the manuscript.
-
Competing interests Stuart N. Peirson's research is funded in part by the Wellcome Trust. None of the authors have any financial interest in any product, method or material or lack thereof mentioned in this article.
-
Provenance and peer review Not commissioned; externally peer reviewed.