Article Text

Abstract
Background: To compare the efficacy of intravitreal pegaptanib (IVP) with panretinal laser photocoagulation (PRP) in the treatment of active proliferative diabetic retinopathy (PDR).
Methods: A prospective, randomised, controlled, open-label, exploratory study. Twenty subjects with active PDR were randomly assigned at a 1:1 ratio to receive treatment in one eye either with IVP (0.3 mg) every 6 weeks for 30 weeks or with PRP laser. Efficacy endpoints included regression of retinal neovascularisation (NV), changes from baseline in best-corrected visual acuity (BCVA) and foveal thickness. Safety outcomes included observed and reported adverse events.
Results: In 90% of randomised eyes to IVP, retinal NV showed regression by week 3. By week 12, all IVP eyes were completely regressed and maintained through week 36. In the PRP-treated group, at week 36, two eyes demonstrated complete regression, two showed partial regression, and four showed persistent active PDR. The mean change in BCVA at 36 weeks was +5.8 letters in pegaptanib-treated eyes and −6.0 letters in PRP-treated eyes. Only mild to moderate transient ocular adverse events were reported with pegaptanib.
Conclusions: IVP produces short-term marked and rapid regression of diabetic retinal NV. Regression of NV was maintained throughout the study and at the final visit.
Statistics from Altmetric.com
Diabetic retinopathy (DR) is a major cause of blindness in the Western world.12 Research into the aetiology of ocular neovascular diseases such as DR has identified a pivotal role for vascular endothelial growth factor (VEGF) in promoting both angiogenesis and increased vascular permeability.34
Intravitreal injection of VEGF induces many of the pathological changes characteristic of DR, including intraretinal and preretinal neovascularisation, microaneurysm formation, intraretinal haemorrhage, macular oedema and areas of capillary non-perfusion with endothelial cell hyperplasia.5 Elevated intraocular levels of VEGF have been reported in patients with DR. Moreover, this elevation is more pronounced in PDR than in non-proliferative diabetic retinopathy (NPDR).67
The Isoform165 of VEGF-A (VEGF165) is particularly potent in promoting ocular neovascularisation and breakdown of the blood–retinal barrier (BRB) through a leucocyte-dependent mechanism.89 Pegaptanib sodium is a selective anti-VEGF aptamer that binds to VEGF165.10 Preclinical studies demonstrated that intravitreal injections of pegaptanib (IVP) can inhibit pathological ocular neovascularisation while leaving physiological vascularisation unimpaired.8 In a recent Phase II study of pegaptanib for the treatment of diabetic macular oedema (DME), findings suggested that IVP may be capable of halting and even reversing pathological retinal neovascularisation (NV).1112
We hypothesised that in patients with active PDR, IVP would cause marked reduction in vitreous levels of VEGF165 with regression of pathological NV, thereby hindering the progression of PDR. In this report we present the final results from our pilot study to test this hypothesis.
Methods
Study design
This study was a randomised, prospective, open-label direct comparison of pegaptanib alone to PRP alone in patients with PDR. It was approved by the Sterling Institutional Review Board, and conducted in conformity to the principles of the Declaration of Helsinki.
Subject selection
Eligible subjects had active PDR, in one or both eyes, with at least one of the following high-risk characteristics as defined by the Diabetic Retinopathy Study (DRS): (1) new vessels within one disc diameter of the optic nerve head that are larger than a third of the disc area and/or (2) vitreous or preretinal haemorrhage associated with either less extensive new vessels at the optic disc, or with new vessels elsewhere half the disc area or larger.13 In addition, at the screening visit, the best-corrected visual acuity (BCVA; measured by the Early Treatment Diabetic Retinopathy Study (ETDRS) chart) was ⩾24 letters (approximately 20/320) and ⩽85 letters (approximately 20/20). Eyes with mild preretinal haemorrhage or vitreous haemorrhage (VH) that did not interfere with visualisation of the macula and optic disc were eligible for inclusion. Subjects could participate in the study only if, in the opinion of the evaluating physician, PRP could be safely withheld for 4 weeks. Exclusion criteria included the following: haemorrhage or media opacity obscuring visualisation of the macula and optic nerve; significant epiretinal membranes (ERM) involving the macula; proliferative diabetic membranes along the major retinal arcades sufficiently extensive to cause either significant vitreomacular traction or significant impairment in BCVA; any tractional retinal detachment; severe ischaemia involving the foveal avascular zone; neovascular glaucoma; study eye treated with intravitreal steroid injections within 6 months prior to baseline and/or PRP treatment within 90 days of baseline.
Randomisation and treatment
After baseline measurements were obtained, eligible eyes were randomly assigned (1:1) to either pegaptanib alone or PRP alone based on a sequence generated by the random number function in Microsoft Excel (Microsoft Corporation, Seattle, Washington). Each patient received treatment with either pegaptanib or PRP at day 0.
Pegaptanib-treated eyes were scheduled to receive a total of six intravitreal injections at 6-week intervals beginning on day 0 and ending at week 30. Commercially available pegaptanib sodium is formulated for intravitreal injection at 0.3 mg/90 μl in preservative-free phosphate-buffered saline (pH 5–7), and packaged in sterile, single-use United States Pharmacopoeia type 1 graduated glass 1 ml syringes with preattached 27-gauge needles.
Injections were administered according to the product recommendations under controlled aseptic conditions using sterile gloves, a sterile drape and a sterile eyelid speculum. Adequate anaesthesia and a broad spectrum microbicide were administered prior to injection.
PRP was administered using a modified ETDRS protocol in one or two sessions, depending on the subject’s tolerance of the procedure. Eyes assigned to PRP could receive an additional treatment at the discretion of the evaluating physician.
For subjects in whom both eyes were eligible, one eye was selected randomly as the study eye. Fellow eyes of these subjects were treated according to standard clinical guidelines established in the DRS. Vitrectomy surgery of fellow eyes was performed if indicated, but treatment of fellow eyes with another anti-VEGF drug and/or intravitreal steroid was not permitted.
Study assessments
Ocular health assessments included an ophthalmic history, protocol refraction and BCVA, tonometry, ophthalmological exam, colour fundus photography, fluorescein angiography (FA) and optical coherence tomography (OCT). Other assessments included medical history, physical exam and vital signs, electrocardiogram (ECG), urine pregnancy check, cholesterol and glycosylated haemoglobin (HbA1c) measurement, telephone safety checks and adverse event recording. All baseline assessments and examinations were performed within 2 weeks prior to the first injection; follow-up visit assessments were completed within 2 weeks of the prescheduled dates.
Efficacy endpoints
The primary endpoint was the regression of PDR from baseline to week 36, defined as regression of NVD and/or NVE. Using clinical findings, FA and fundus photography, the level of neovascularisation was classified as (1) active, (2) partially regressed, which was defined as a reduction equal or greater than 50% compared with baseline, or (3) regressed. Additional efficacy endpoints were changes from baseline to week 36 in BCVA assessed by ETDRS letter-score, as well as changes in OCT assessments of central macular thickness (CMT) and macular volume (MV).
Safety endpoints
Safety outcomes included all observed and reported adverse events and serious adverse events, whether attributable to treatment or not. Data from ECG, vital signs and laboratory tests were also monitored. Safety outcomes and injection-related events of particular concern included elevated intraocular pressure, lens damage, retinal detachment, and infectious and non-infectious endophthalmitis.
Criteria for treatment failure in eyes that received either IVP or PRP were defined as any one of the following: (1) development or increased NVD and/or NVE; (2) NVD and/or NVE that was not regressed by at least 50% within 3 weeks in comparison with the baseline amount; (3) development of significant VH that was sufficient in quantity to obscure visualisation of the entire macula, optic disc and the major temporal arcade vessels. Any study eye meeting one or more of the above criteria was treated with the standard of care, including PRP and focal/grid laser.
Data analysis
Baseline demographic information and safety endpoints are summarised descriptively. No estimates were made to determine the patient population size required to detect prespecified differences between treatment groups. The efficacy endpoints between the two groups at 36 weeks were assessed using a χ2 exact and unpaired t test. All data analysis was done using STATA 8 (Station Corp LP, College Station, Texas).
Results
Study eyes
Ten study eyes were each initially enrolled in both the pegaptanib and PRP-treatment arms; however, two subjects from each arm were discontinued due to patient non-compliance prior to study conclusion. In the pegaptanib-treated arm, the two patients exited the study at weeks 18 and 30. In the PRP-treated arm, one subject exited the study after the baseline visit and the other at week 30. Data analysis was carried through until the last follow-up visit. The mean age of the remaining subjects was 56.2 years and 59 years, respectively. Baseline characteristics for both groups are summarised in table 1.
Patient demographics
All 10 pegaptanib-treated eyes showed at least partial NV regression defined as a reduction of more than 50% of the NV size at week 3. Ninety per cent of these eyes presented complete regression of the NV. By week 12, all of the eyes were completely regressed, and this was maintained until the final visit at week 36. In contrast, among the nine PRP-treated control eyes, neovascularisation was completely regressed in two eyes at week 3. At week 6, these two eyes remained stable, and two additional eyes improved from active to partial regression of NV. At week 36, two eyes showed complete regression, two demonstrated partial regression, and four remained active (table 2).
Neovascularisation status in the intravitreal pegaptanib (IVP) and panretinal laser photocoagulation (PRP)-treated eyes
At baseline, mean BCVA scores were similar between treatment groups (76 letters in each arm). At week 3, mean scores had improved by 5.8 letters in the pegaptanib-treated eyes and declined by 3.0 letters in the PRP-treated eyes. In the pegaptanib-treated arm, the change in mean BCVA from baseline was +5.1 at week 6 and +5.8 at week 36. In the PRP-treated group, the change in mean BCVA was +3.0 and −6.0 at weeks 6 and 36, respectively (table 3). The differences between both groups were not statistically significant (p = 0.22).
Early Treatment Diabetic Retinopathy Study visual acuity (VA) scores
All study eyes had OCT assessments performed at the initial baseline visit and at the week 36 visit according to the study protocol. Note that one subject in the pegaptanib-treated group did not receive OCT assessment at baseline; this subject will not be included in the analysis. In addition, OCT assessments were also performed on a subset of eyes at week 3 and week 6. These consisted of six pegaptanib-treated eyes and six PRP-treated eyes.
In the subset of pegaptanib-treated eyes mean CMT was 201 μm at baseline (range 138–310 μm), 178 μm at week 3 (range 132–243 μm), 175 μm at week 6 (range 138–228 μm) and 191 at week 36 (range 144–360 μm). In the subset of PRP-treated eyes, the mean CMT was 232 μm (range 144–420 μm) at baseline, 229 μm (range 136–312 μm) at week 3, 226 μm (range 147–297 μm) at week 6, and 303 μm at week 36 (range 161–604 μm) (fig 1).

Comparison of central macular thickness between IVP and PRP-treated eyes. IVP, intravitreal pegaptanib; OCT, optical coherence tomography; PRP, panretinal photocoagulation. The comparison between the two groups for macular thickness at 36 weeks was statistically significant, that is, p = 0.025 (t test).
The comparison between the two groups for NV and macular thickness at 36 weeks was statistically significant, with p = 0.021 (χ2 exact) and p = 0.025 (t test) respectively. However, differences in visual outcome was not statistically significant, with p = 0.22 (t test).
Fellow eyes of the pegaptanib-treated subjects
Of the 10 fellow eyes of the pegaptanib-treated group, five met the study entry criteria and received PRP treatment. This group responded to treatment in the same fashion as the PRP-treated group. The mean BCVA at baseline was 82.0 letters. There was a decrease in mean BCVA from baseline of 1.4 letters at week 3, an increase of 0.2 letters at week 6, and a final decrease of 7.4 letters at week 36. Four of these eyes underwent OCT assessment at baseline and weeks 3, 6 and 36. The mean CMT was 201.5 μm at baseline (range 158–285 μm), 224.8 μm at week 3 (range 163–295 μm), 214.3 μm at week 6 (range 166–314 μm) and 271.5 μm at week 36 (range 216–334 μm).
Safety outcomes
The pegaptanib study eyes experienced mild to moderate transient ocular adverse events including most commonly subconjunctival haemorrhage following study injections. One eye presented with ERM; no other ocular adverse events were noted. Fellow eyes of this group presented with ERM (one eye), VH (two eyes), cataract formation (one eye) and DME (one eye).
Study eyes of the PRP-treated group presented with ERM (four eyes), VH (two eyes), iritis (one eye) and macular hole (one eye). The fellow eyes of this group presented with ERM (one eye), VH (two eyes) and DME (one eye).
Discussion
Over the past 25 years, large-scale clinical trials such as the DRS and ETDRS have contributed immensely to our understanding of DR. These landmark studies clearly established a role for the use of PRP as an effective treatment modality for PDR.14151617 While PRP can reduce the risk of severe vision loss in diabetic retinopathy, it is an anatomically destructive treatment unavoidably associated with an increased risk of moderate adverse effects that negatively impact visual function and patient quality of life.181920
Since its identification, the VEGF molecule has been shown to play a pivotal role in the angiogenic process.21222324 Blockage of the VEGF165 isomer may inhibit pathological neovascularisation with little or no effect on physiological neovascularisation.202225
In this study, after a single pegaptanib treatment, significant NV regression occurred in all eyes by week 3. No eyes met the treatment failure criteria. More importantly, this regression was maintained throughout the study (fig 2). These results support our hypothesis and the fundamental assertion that VEGF165 plays an important role in the development and maintenance of pathological neovascularisation secondary to PDR.1224

{kind=link}
{kind=link}
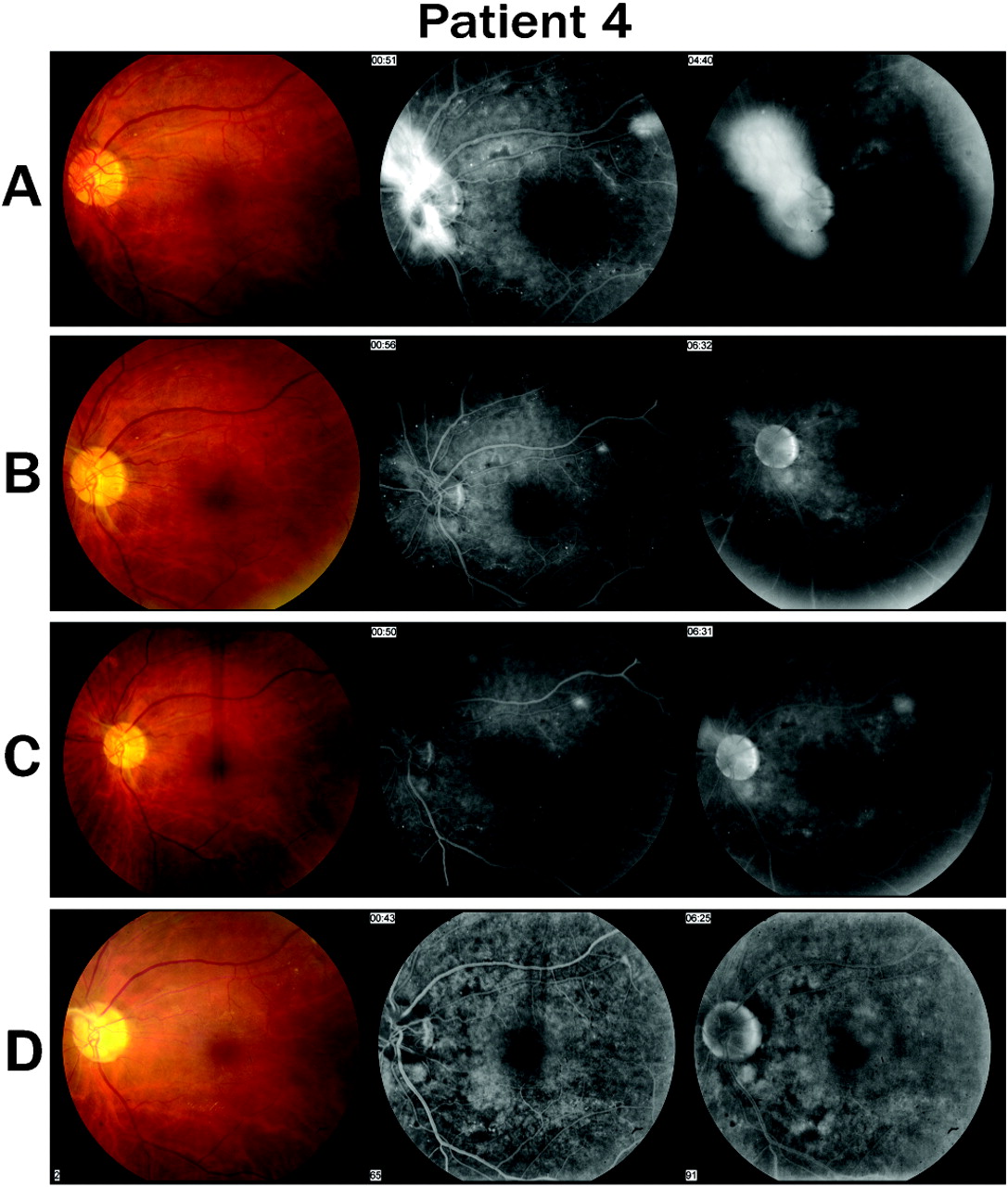
Colour fundus photos and mid- and late-phase fluorescein angiograms in a pegaptanib-treated eye showing (A) active neovascularisation of the disc (NVD) with high-risk characteristics at baseline; (B) regression of NVD 3 weeks after pegaptanib treatment; and (C) complete regression of NVD 6 weeks after treatment. (D) Maintained regression of NVD at week 36.
The majority of PRP-treated eyes failed to regress completely at 36 weeks. At the end of the study, half of the eyes showed persistent active PDR. Seven eyes in the PRP-treated group met one or more of the criteria for treatment failure at week 3. All of these eyes received additional treatment with PRP and/or focal laser. Despite treatment, only one eye subsequently developed a dense VH at week 36, necessitating vitrectomy. In sharp contrast, none of the pegaptanib-treated eyes in this study required retinal laser or surgery at any point during the study.
The PRP-treated eyes exhibited a fluctuation in mean BCVA, with an eventual decrease below baseline at week 36. However, as mentioned, one subject in this group presented with a dense VH at week 36. If the BCVA data for this subject are removed from the analysis, the mean BCVA for this group is slightly greater than baseline at week 36.
These data suggest that VEGF blockade may be a safe and efficacious adjuvant treatment to PRP in PDR. It may also have the potential to reduce the overall amount of PRP treatment needed to treat PDR, thereby reducing the adverse effects associated with it. Furthermore, this treatment should help to prevent severe vision loss due to progression of NV and other complications associated with the more advanced stages of PDR. A study currently enrolling in our clinic is designed to help answer this question.
Our findings also suggest that IVP is effective in reducing concomitant DME. A statistically significant difference was noted in the CMT between both groups at 36 weeks (p = 0.025)
With the results obtained in the current study, one could raise the possibility that greater benefit could be achieved with the combination of PRP and IVP rather than PRP or IVP alone. Currently an outgoing study by our group is evaluating the combination of PRP and IVP in the treatment for PDR. The interim results were presented at the Association for Research in Vision and Ophthalmology (ARVO) at Fort Lauderdale, Florida in 2008 (ARVO 2008 Session 331, poster A542).
Ultimately, we suggest that IVP produces marked and rapid short-term regression of diabetic NV. In some eyes, pegaptanib treatment may also reduce the severity of coexisting DME. Whether or not anti-VEGF therapy must be continued indefinitely is still a question that remains to be answered, and will require further study.
After concluding our study, we stopped recording data after the subjects exited the study, as the IRB would have required a new consent from the subjects to gather such data. On average, however, in most of the IVP-treated eyes, NV began to crop up at about 10–12 weeks in the clinic, requiring PRP.
REFERENCES
Footnotes
Funding This study was supported by a grant from Pfizer, New York and (OSI) Eyetech, New York.
Competing interests VHG is a paid consultant and speaker for (OSI) Eyetech Pharmaceuticals.
Provenance and Peer review Not commissioned; externally peer reviewed.
Ethics approval Ethics approval was provided by Sterling Institutional Review Board.
Patient consent Obtained.
Linked Articles
- At a glance