Article Text

Abstract
Aim To characterise the presence of a hyperautofluorescent (HAF) ring associated with choroidal neovascularisation (CNV) complex in patients with wet age-related macular degeneration (AMD).
Methods Fundus autofluorescence images and spectral-domain optical coherence tomography (OCT) scans from 362 eyes with wet AMD were reviewed. The presence and size of an HAF ring associated with the CNV complex was evaluated. A subgroup of 64 treatment-naive eyes with new-onset CNV was studied to analyse the relationship between pretreatment OCT characteristics and the presence of the HAF ring.
Results An HAF ring was present in 38% of the entire cohort of eyes and in 39% of treatment-naive eyes. The presence of the HAF ring was significantly correlated with the extent of baseline subretinal fluid (SRF) on OCT (p=0.0113), the number of antivascular endothelial growth factor (VEGF) injections (p=0.0439) and the number of treatment cycles (p=0.0154). Eyes with an HAF ring were more likely to have disruption of the ellipsoid zone line once the SRF was resolved compared with eyes without an HAF ring (p=0.0002). In multivariate analysis, the best predictors for HAF ring were the baseline area of SRF (p=0.0449) and the number of anti-VEGF treatments received (p=0.0568).
Conclusions Nearly 40% of wet AMD eyes had an HAF ring. In treatment-naive eyes, the HAF ring had a significant association with SRF and was found as early as the baseline measurement and as long as 18 months after beginning treatment, persisting for up to 6 years after the initial diagnosis. Its association with baseline SRF and disruption of the ellipsoid zone line of the photoreceptors on OCT could indicate continuous stress on the outer retinal structures after exposure to prolonged SRF and/or transmitted autofluorescence from loss of the photoreceptors overlying the retinal pigment epithelium.
- Imaging
- Macula
Statistics from Altmetric.com
Introduction
Age-related macular degeneration (AMD) is a multifactorial, chronic disease that causes progressive impairment of central vision. According to the WHO, AMD ranks third as a cause of blindness worldwide after cataract and glaucoma, and is the leading source of irreversible vision loss in industrialised countries.1 Choroidal neovascularisation (CNV) characterises the exudative (neovascular or ‘wet’) form of AMD, in which abnormal new blood vessels proliferate beneath the retinal pigment epithelium (RPE) and invade the subretinal space. This gives rise to intraretinal and subretinal fluid (SRF), haemorrhages, RPE detachments, lipid deposition and ultimately fibrotic scarring with disruption of the RPE and consequent loss of the overlying photoreceptors.2 ,3
The introduction of confocal scanning laser ophthalmoscopy (cSLO) has made possible the visualisation of fundus autofluorescence (FAF) as a non-invasive imaging technique that assesses the health and function of the RPE.4 ,5 The cSLO has become a useful tool in AMD, allowing evaluation of lipofuscin content in RPE cells using FAF imaging modality.6 ,7 Decreased FAF is indicative of RPE atrophy and photoreceptor loss, while increased FAF suggests compromised RPE function in areas with elevated metabolic demand and hence higher concentrations of lipofuscin.8 ,9
Among some of the patients with neovascular AMD examined in our clinic, we have noticed a hyperautofluorescent (HAF) ring surrounding the CNV complex; the significance of this ring is not clearly understood. We hypothesised that the presence of SRF, which is typical of this form of AMD, stresses the RPE and therefore could give rise to this enhanced FAF. To test our hypothesis, we performed the present study investigating factors associated with this HAF ring.
Methods
Inclusion and exclusion criteria
In this retrospective study, we included 248 consecutive patients with history of wet AMD (362 eyes), of which 58 were treatment-naive patients with new-onset CNV secondary to wet AMD (64 eyes). All patients presented for imaging studies at the Jacobs Retina Center of the University of California, San Diego, between March 2008 and October 2013.
To be included in the study, all patients had a diagnosis of wet AMD and must have had performed cSLO examination using Heidelberg Spectralis (Heidelberg Engineering, Heidelberg, Germany), including spectral-domain optical coherence tomography (OCT) scans, FAF images and fluorescein angiography (FA) images. From the time of first examination at our institution, patients received antivascular endothelial growth factor (VEGF) therapy every four weeks in the case of bevacizumab or ranibizumab, and every eight weeks for aflibercept until intraretinal fluid (IRF) and SRF, as well as leakage on FA, were resolved.
Eyes with poor-quality images, namely from media opacities or posterior segment pathology preventing the evaluation of the retinal imaging (eg, subretinal haemorrhage), inflammatory choroidopathies, history of retinal detachment, hereditary retinal diseases and ocular trauma, were excluded from the study. In addition, eyes with CNV secondary to pathology different from AMD and patients with dry AMD were excluded from the study.
Imaging evaluation
Trained physicians (NC, GB and JTN) evaluated cSLO images at first examination showing wet AMD of treatment-naive eyes (referred as baseline examination). First, examiners used built-in callipers of the cSLO device to measure the largest horizontal and vertical extent of the CNV lesion on OCT scans, including the presence of IRF, SRF and RPE detachment (pigment epithelial detachment). Separate measures were obtained solely for the SRF vertical and horizontal dimensions. Second, examiners looked at the presence of an HAF ring associated with the CNV complex on FAF images. If the ring was present, they manually outlined its margins using a dedicated built-in tool of the cSLO device. Third, examiners measured the HAF ring vertical and horizontal dimensions on FAF image at the same location of the previously measured dimensions on OCT, superimposing the FAF image with the near-infrared image connected to the OCT scan using a program that allows setting transparent windows (Chaos Crystal V.2.0.001, Elgorithms, Pryor Creek, Oklahoma, USA).
If the HAF ring was not present at baseline, examiners searched for the presence of the ring at follow-up visits during the anti-VEGF therapy, as well as at the end of the first cycle of treatment. In addition, the cSLO images from the last follow-up visit of the 64 eyes with new-onset CNV were evaluated to verify the presence or absence of the HAF ring at this time point. The corresponding measurements on OCT scans and on FAF images were taken and compared with the previous ones from baseline examination. The OCT scans were also reviewed for evaluation of outer retinal structures within the area of the HAF ring.
Standardised human grading
Grading of hyperautofluorescence intensity among patients with the HAF ring was performed using human readers who used reference images to grade and qualitatively classified them as having low, moderate or high HAF (figure 1) compared with the background autofluorescence, defined as the FAF of unaffected retinal tissue outside the macular lesion in the same frame, to control for changes in brightness between different images. This was done by consensus of three graders.

Fundus autofluorescence imaging showing low (A), moderate (B) and high (C) hyperautofluorescent ring intensity.
HAF intensity electronic quantification
For an objective measurement, the examiners used Java-based image processing software, ImageJ (NIH, Bethesda, Maryland, USA) to electronically quantify the autofluorescence intensity in a 900 μm square located at the point of maximum intensity within the HAF ring and compared it with a 900 μm square of adjacent healthy retinal tissue exhibiting normal FAF. The difference between these two measurements was designated as the HAF ring objective intensity.
Statistical analysis
Statistical analysis was performed using JMP statistical software V.11 (SAS Institute, JMP Software, SAS Campus Drive, Cary, North Carolina, USA). Univariate and multivariate analyses were performed using HAF ring information as response variables and ocular as well as systemic characters as independent variables. The analysis was performed after the first treatment cycle and at the last follow-up. Both nominal logistic regression and ordinal logistic regression were performed to capture information of the autofluorescence intensity of the ring. For the agreement analysis between raters for HAF ring intensity, SAS software was used and weighted κ was tested and reported. For parametric analysis of HAF ring intensity acquired through ImageJ, the intensity was categorised according to the quartiles (1 for values <35 (25% quartile), 2 for values between 35 and 62, and 3 for values >62 (75% quartile) and 0 for the cases without an HAF ring). Since patients without HAF rings all had zero fluorescein intensity and the measured HAF ring intensity was not normally distributed, non-zero data were categorised into ordinal based on quartiles of their distribution.
The statistical significance was assumed when p value was <0.05.
Results
Tables 1 and 2 show the demographic characteristics of the study population. The mean age of the 248 patients with history of wet AMD was 79 years (range 49–97), of which 61% were women. The subgroup of 58 treatment-naive patients had a mean age of 78 years (range 65–92), of which 62% were women. At the time of baseline examination, over half of the eyes were pseudophakic (56.3%) and mean best-corrected visual acuity (VA) was 0.3 (SD 0.37) in logarithm of the minimum angle of resolution scale.
Patient characteristics (entire population)
Patient characteristics (subgroup of treatment-naive eyes)
Out of the 362 eyes included, 138 (38.1%) showed an HAF ring associated with the CNV complex during anti-VEGF treatment; all patients had persistence of the HAF ring throughout the observation period to the last follow-up visit (up to 6 years). In the treatment-naive group (table 3), an HAF ring was present in 10 eyes (15.6%) at baseline and in 23 eyes (35.9%) at the end of the first cycle of treatment. Of these 23 eyes, 21 (91.3%) had SRF on baseline OCT compared with 19 (46.3%) from the remaining 41 eyes without the HAF ring. At the time of the last visit, two more eyes had develop an HAF ring, giving a total of 25 eyes (39.1%).
Clinical characteristics of the treatment-naive eyes after the first treatment cycle and at the last follow-up visit
Comparing measurements of the baseline SRF on OCT scans with measurements of the HAF ring seen on subsequent FAF, we found a positive concordance of the measurements in 18 out of the 21 eyes (85.7%) with SRF on baseline OCT (figures 2 and 3). Patients with IRF at baseline, but absent SRF, did not display an HAF ring at baseline or subsequent examinations (figure 4). When doing a bivariate fit, we found a positive correlation between the size of the HAF ring and the size of the baseline SRF (r2=0.56); in addition, there was a strong relationship between vertical and horizontal measurements of the HAF ring and the extent of SRF on OCT (r2=0.78).

Fundus autofluorescence showing ring of hyperautofluorescence (A), baseline infrared image (B) with demarcating line for optical coherence tomography (OCT) scan (D), which shows the presence of subretinal fluid (5974 μm in length measured by built-in callipers) and overlap of figures 2A and B (C) with corresponding measurements of hyperautofluorescent (HAF) ring area (33.89 mm2), vertical length (6086 μm) at the same location as the vertical OCT scan on (D). Follow-up OCT scan (E) showing resolution of subretinal fluid and disruption of ellipsoid zone line in the location of HAF ring.

Fundus autofluorescence showing ring of hyperautofluorescence (A). Corresponding baseline infrared image (B) with demarcating line crossing through area of hyperautofluorescent ring, outlining the position of the baseline optical coherence tomography (OCT) scan (C) with the presence of subretinal fluid. Follow-up OCT scan (D) showing resolution of subretinal fluid and disruption of ellipsoid zone line in the location of the hyperautofluorescent ring.
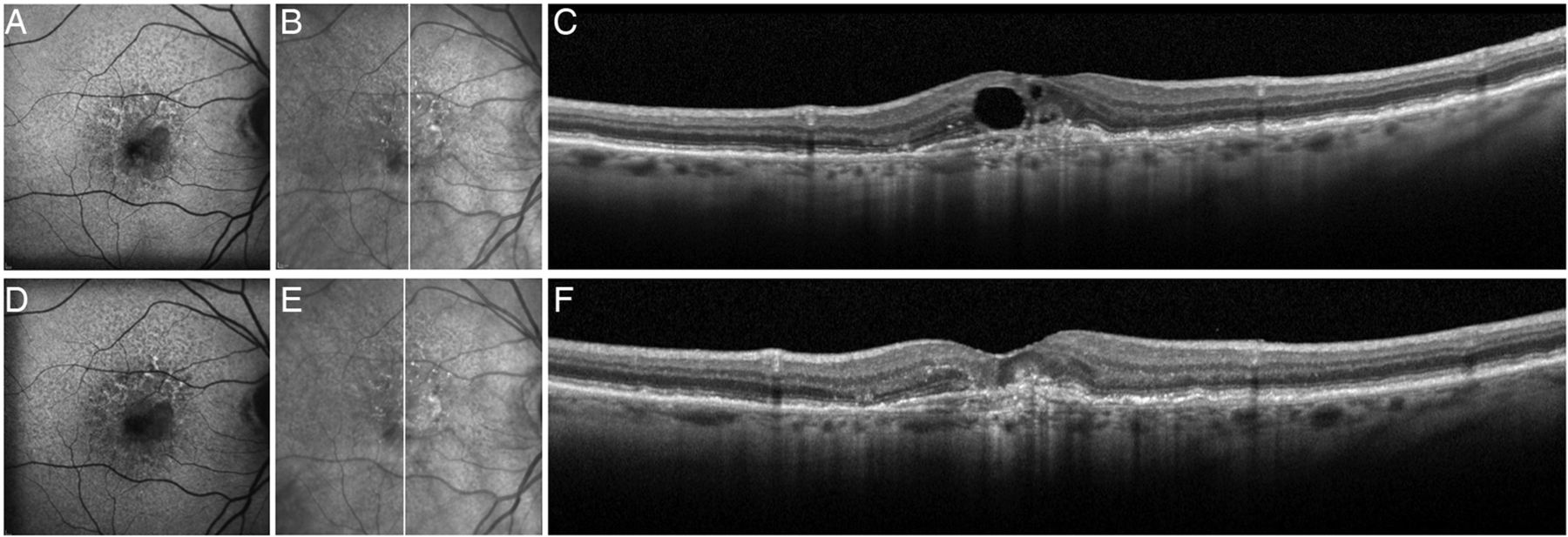
Fundus autofluorescence at baseline showing speckled hypoautofluorescence/hyperautofluorescence around the macula, but no clear hyperautofluorescent ring (A). Corresponding near-infrared image (B) with demarcating line outlining the position of the optical coherence tomography (OCT) scan (C) showing the presence of subfoveal pigment epithelial detachment, pigment migration and cystic intraretinal fluid. Follow-up retinal fundus autofluorescence (D), near-infrared image (E) and corresponding OCT scan (F) showing resolution of intraretinal fluid and subfoveal loss of retinal pigment epithelium and ellipsoid zone line, corresponding to area of increased hypoautofluorescence. Note the absence of hyperautofluorescent ring (D).
Associations between baseline predictors and HAF ring at the end of the first cycle of treatment are shown in table 4. There was a significant association of the presence of HAF ring with the baseline area of SRF (p=0.0113) and with the number of injections performed (p=0.0439). There was also a trend of association between HAF ring and length of treatment needed (p=0.1192) but no association with the estimated disease duration before treatment.
Univariate analysis of predictors for hyperautofluorescent ring presence after first treatment cycle
Associations between baseline predictors and HAF ring at the final follow-up visit are shown in table 5. We found that duration of follow-up (p=0.0053), number of injections (p=0.0154) and number of recurrences of CNV activity (p=0.0014) were associated with the presence of the HAF ring.
Univariate analysis of predictors for hyperautofluorescence ring presence at last follow-up
We also found that eyes with an HAF ring on FAF were more likely to have loss or disruption of the ellipsoid zone line on OCT once the SRF was resolved (figures 3 and 5) compared with patients without an HAF ring (p=0.0002). Among patients with an HAF ring, there was a greater disruption or loss of the ellipsoid zone line in those with a higher HAF ring intensity (p<0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fundus autofluorescence showing hyperautofluorescent ring (A). Corresponding baseline infrared image (B) with demarcating line crossing through area of hyperautofluorescent ring, outlining the position of the baseline optical coherence tomography (OCT) scan (C) with the presence of subretinal fluid. Follow-up OCT scan (D) showing resolution of subretinal fluid and disruption of ellipsoid zone line in the location of the hyperautofluorescent ring.
Due to the presence of co-linearity among some independent variables, we performed a multivariate analysis (table 6) and found that the best predictor for HAF ring presence was the baseline area of SRF (p=0.042), followed by the number of anti-VEGF injections received (p=0.095), which showed a statistical trend towards significance.
Multivariate analysis of predictors for hyperautofluorescent ring presence after first treatment cycle
Standardised human grading
Reproducibility of ring intensity (intensity of HAF) as classified by three masked examiners was high, with a weighted κ value of 0.75, p=0.002. Using an ordinal logistic regression analysis (table 7), we found that baseline SRF area (p=0.0097) and number of injections received (p=0.004) were independently predictive of HAF ring presence and intensity.
Multivariate analysis of predictors for hyperautofluorescent ring intensity after first treatment cycle
HAF intensity electronic quantification
We also used the objective grading obtained from ImageJ software for multivariate analysis of predictors of HAF ring intensity (table 8) and found similar results to those obtained with the Standardised Human Grading, showing again that the most predictive variables for HAF ring intensity were baseline SRF area (p=0.0449) and the number of injections received, which reached borderline statistical significance (p=0.0568).
Multivariate analysis of predictors for hyperautofluorescent ring intensity after first treatment cycle
Discussion
In this study, we described and analysed the presence of an HAF ring in a consecutive series of 362 eyes with history of wet AMD and found a prevalence of 38%. When analysing a subgroup of treatment-naive eyes, we found a very similar prevalence of 39%. The occurrence and size of the HAF ring were strongly correlated to the extent of SRF on OCT at baseline and with disruption of the ellipsoid zone line at the time of the last follow-up. The number of anti-VEGF treatments received, and therefore the persistence of active wet AMD, also influenced its development.
To the best of our knowledge, the characterisation of the HAF ring in AMD has not been clarified in the literature, although FAF phenomena in this disease are well documented.10–13 Most of the FAF research done has been in eyes with non-neovascular AMD and particularly on the classification and impact of specific patterns of abnormal FAF in patients with geographic atrophy (GA).4 ,14–16 It has been shown that areas with increased FAF signal precede the development or the enlargement of GA and that phenotypic features of FAF abnormalities have an impact on atrophy progression.17 We previously published on the correlation between OCT and FAF at the margins of GA and showed a statistically significant correlation between the pattern of FAF and the type of OCT margin in these patients. Areas displaying increased FAF have a corresponding irregular margin on OCT, suggesting abnormal hypertrophic and damaged RPE cells with increased lipofuscin correlating to increased autofluorescence on FAF imaging.18
A number of studies have looked at FAF findings in neovascular AMD.4 ,8 ,10 ,11 ,16 ,19 ,20 von Rückmann et al10 reported areas of increased FAF around disciform lesions that corresponded to areas of irregular pigmentation, which may have been caused by a multilayered RPE or accumulation of intracellular material from exudation of new vessels.
Vaclavik et al21 reported on the importance of preserved continuous autofluorescence as a possible marker for RPE/photoreceptor complex viability after the onset of CNV, presuming that the autofluorescence is derived from the RPE in these patients.
Schmitz-Valckenberg et al16 conducted a comprehensive review on FAF and the progression of AMD; they found that consistently areas with high FAF often extend beyond the edge of the angiographically defined CNV lesion and are usually located inferiorly as a result of gravity effects.
Studies done on other macular pathologies, such as central serous chorioretinopathy (CSC), have described a similar finding, and it has been speculated to represent areas with SRF with accumulation of outer segments of photoreceptors in the subretinal space and dispersed chromophores.22–24 Kim et al published a series of 91 eyes with history of resolved CSC and abnormal FAF imaging. Twenty per cent (20.9%) of the eyes in their series had a hyper-type or mixed-type FAF, and this finding was significantly associated with loss of the ellipsoid zone line of the photoreceptors on OCT, suggesting that a larger hyper-FAF-type or mixed-FAF-type lesion may indicate a more severely damaged ellipsoid zone line.22 On the other hand, Greenberg et al25 evaluated the autofluorescence features of achromatopsia and concluded that the area of HAF found in 71% of their patients likely reflected increased cone outer segment turnover, marked by intensified bisretinoid deposition in the RPE.
In our study, we found a ring of enhanced FAF that was significantly associated with baseline SRF extent of the CNV complex and that could represent the boundary of the maximum amount of fluid following resolution or at least regression from prior levels. All patients had persistence of the HAF ring until the present time (up to 6 years), and when evaluating the integrity of the ellipsoid zone line at the end of the observation period, we found a significant correlation between the presence of the HAF ring and disruption of this outer retinal structure, which to our knowledge has not been documented previously. Furthermore, eyes with higher-intensity HAF rings had greater disruption or complete loss of the ellipsoid zone line, suggesting a possible transmission effect from the underlying RPE. Chen et al26 reported this phenomenon in eyes with neovascular AMD using the model of macular translocation and found that many had well-delineated increased FAF lesions in the parafoveal region likely caused by the unmasking effect of visual pigment reduction resulting from permanent outer segment shortening rather than fluorophores within the neuroretina. Schmitz-Valckenberg et al16 had previously stated that the intensity of the FAF is not always related to the concentration of fluorophores within the RPE, but instead can be caused by other fluorophores located anterior or posterior to the RPE or by masking of the RPE FAF through reduced absorption of excitation light by pigments located anterior to the RPE.
The HAF ring also showed an association towards the total number of anti-VEGF injections, indicating a longer duration of SRF in contact with RPE, thereby needing a greater number of injections to control the active disease. The duration until dry through the first cycle of treatment had a trend towards significance in the right direction, indicating also a possible longer exposure to fluid, but it did not reach statistical significance as follow-up days have a large standard variation. However, because in a cohort of study eyes it was present at baseline before starting anti-VEGF treatment, we believe that the HAF ring was related to fluid or fluid duration and its deleterious effect on the photoreceptors; not treatment itself. This finding may have clinical implications by elucidating areas of stressed or vulnerable RPE and resulting damage to the outer retina or perhaps may serve as a potential prognostic factor, denoting a possible worse outcome in patients with a positive HAF ring, although in our series there was no significant difference in terms of VA among treatment-naive patients with and without this finding (p=0.65).
The lack of association between VA and the presence of the HAF ring can be explained by the fact that we measured the Early Treatment Diabetic Retinopathy Study central VA and our findings of the HAF ring were extrafoveal; therefore, we did not assess the subfoveal outer retinal integrity. We know from previous papers published by our group that microperimetry measurements do correlate with areas of absent photoreceptors,27 but given the retrospective nature of our study, we were not able to evaluate the possible association between microperimetry defects and HAF ring presence.
We did not find an association between the presence of an HAF ring and the estimated disease duration before anti-VEGF therapy until the end of first treatment cycle, but we noted that the time between CNV onset and initiation of treatment was a poorly defined parameter derived from patient interviews. Moreover, we found that the overall follow-up for the patients with the HAF ring was statistically longer than for those without it, suggesting longer disease duration.
This study has some limitations. FAF image quality is variable in quality, depending on pupillary dilation and ocular media transparency; this could affect imaging interpretation. In addition, in patients with wet AMD, other findings such as RPE detachment can produce changes in FAF and therefore serve as confounding factors at the time of measuring the HAF ring. Strengths of our study include the use of a single instrument to measure blue hyperautofluorescence, masked examiners to study images and a fairly large number of study eyes.
In summary, the presence of an HAF ring on FAF was found in nearly 40% of the patients with CNV in wet AMD. In patients with new-onset CNV and no previous treatment, the HAF ring showed a significant correlation with the presence of SRF and was found as early as baseline and as long as 18 months after beginning treatment, persisting for up to 6 years after the initial diagnosis. Its positive association with OCT finding such as the extent of baseline SRF and latter disruption of the ellipsoid zone line, as well as its correlation with disease duration, indicates continuous stress on the outer retinal structures after lasting exposure to SRF associated with CNV in AMD. These finding could reflect increased cone outer segment turnover, with intensified bisretinoid deposition in the RPE and resulting increased FAF, or an unmasking transmission effect of the normal RPE autofluorescence by the absent or disrupted ellipsoid portion of the photoreceptor inner segments.
Further research should help us understand the causative factors and prognostic significance of the HAF ring and perhaps its usefulness in the evaluation and management of wet AMD and its response to anti-VEGF therapy.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data: NC, GB, JTN, SE-E and WRF. Drafting the work or revising it critically for important intellectual content: NC, GB, LC, D-UB and WRF. Final approval of the version published: WRF.
Funding This study was supported by NIH grants R01EY007366 (WRF) and R01EY020617 (LC), and in part by an unrestricted fund from Research to Prevent Blindness to the Department of Ophthalmology, University of California San Diego. NC has funding by the Pan-American Ophthalmological Foundation (PAOF) and Retina Research Foundation.
Competing interests GB is a full-time employee at Genentech.
Ethics approval This study adhered to the tenets of the Declaration of Helsinki, complied with Health Insurance Portability and Accountability Act regulations, and was approved by the Institutional Review Board of the University of California, San Diego.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance