Article Text

Abstract
Purpose To report the clinical and microbiological profile of keratitis caused by Corynebacterium spp.
Methods The medical and microbiology records of 22 patients, who had presented at the L V Prasad Eye Institute, Bhubaneswar, between June 2009 and December 2012, and whose corneal scrapings had yielded significant growth of Corynebacterium spp, were retrospectively reviewed. A detailed ocular examination was performed before the respective corneal scraping was sent for a microbiological work-up. The data collected from each record included age, gender, predisposing factors (ocular and systemic), clinical presentation, management and outcome of treatment.
Results The mean age of the patients was 43.8±24.4 years. Ocular predisposing factor was present in 14 (63.6%) eyes. Surgical intervention was required in 12 (54.5%) patients. In vitro susceptibility (Kirby–Bauer disc diffusion method) results of Corynebacterium spp to vancomycin (17/19, 89.5%), cefazolin (16/20, 80%), chloramphenicol (11/20, 55%), ofloxacin (13/19, 68.4%), ciprofloxacin (10/20, 50%) and gatifloxacin (10/19, 52.6%) were variable. Drug resistance (more than one drug) was seen in nine (40.9%) Corynebacterium isolates, of which, two (22.2%) showed multidrug resistance to three or more classes of antibiotics.
Conclusions Corynebacteria can cause severe corneal infection requiring surgical intervention.
- Cornea
Statistics from Altmetric.com
Introduction
Bacterial keratitis can lead to significant loss of vision.1 The severity of corneal infection is dependent on the virulence of the organism and the underlying condition of the cornea.2 ,3 It occurs when microorganisms overcome host defences. Under conditions, such as trauma or systemic infection, the normal flora too can contribute to ocular infection.
The predominant resident normal commensals of the external ocular surface are Staphylococcus epidermidis and Corynebacterium xerosis. Although Corynebacterium spp, which are also referred to as diphtheroids, are regarded as non-pathogenic organisms, they have been recognised as the cause of serious systemic and ocular infection.4–6 Corynebacterium spp are associated with conjunctivitis,7 keratitis8 ,9 and endophthalmitis.10 ,11
Corynebacterium spp occur commonly in nature in the soil, water, plants and food products.12 Some species are known for their pathogenic effects in human beings and other animals. The most notable infection is diphtheria that is caused by C. diphtheriae. Other pathogenic species in human beings include C. amycolatum, C. striatum, C. jeikeium, C. urealyticum and C. xerosis.13
During the past few years, there have been an increased number of ocular infections due to coryneform bacteria.8 ,10 ,14 At L V Prasad Eye Institute, Bhubaneswar, a large number of patients are seen with microbial keratitis. In this report, we share the clinical and microbiological profile of keratitis caused by Corynebacterium spp.
Materials and Methods
The medical and microbiology records of all patients, who had presented at the LV Prasad Eye Institute, Bhubaneswar, between June 2009 and December 2012, and whose corneal scrapings had yielded significant growth of Corynebacterium spp, were retrospectively reviewed. The following data were collected from each record: age, gender, predisposing factors (ocular and systemic), clinical presentation, management and outcome of treatment.
A detailed ocular examination was performed before collecting the sample for microbiological investigation (figure 1). As per our institutional protocol, all cases of clinically non-viral microbial keratitis require microbiological investigation, which consists of smear examination and culture of the corneal scrapings. Corneal scraping was done using #15 surgical blades on a Bard-Parker handle under topical anaesthesia (0.5% proparacaine hydrochloride). Microbiological processing included Gram stain, potassium hydroxide/calcofluor white (KOH+CFW) mount and inoculation on appropriate media (5% sheep blood agar, 5% sheep blood chocolate agar, Sabouraud dextrose agar (SDA), non-nutrient agar with Escherichia coli, thioglycollate broth and brain heart infusion broth). All media were incubated aerobically at 37°C except chocolate agar (incubated in 5% CO2 at 37°C) and SDA (incubated at 27°C). The media were observed for 14 days for any growth. Colonies growing on the site of inoculum were considered for further processing and identification. Characteristic colonies on solid media and turbidity in liquid media were subjected to Gram stain and standard biochemical tests for the confirmation of Corynebacterium spp. A culture was considered significant when there was growth of the same organism on two or more media and/or confluent growth at the site of inoculation on one solid medium and/or growth in one medium with consistent (matches with) direct microscopy findings of the corneal scraping. In few cases, analytical profile index (bioMerieux, USA) was done to identify Corynebacterium species. Antibiotic sensitivity of Corynebacterium spp was done by disc diffusion Kirby–Bauer method on blood agar as per Clinical and Laboratory Standards Institute guidelines.

Slit lamp photograph showing full-thickness corneal infiltrate and hypopyon.
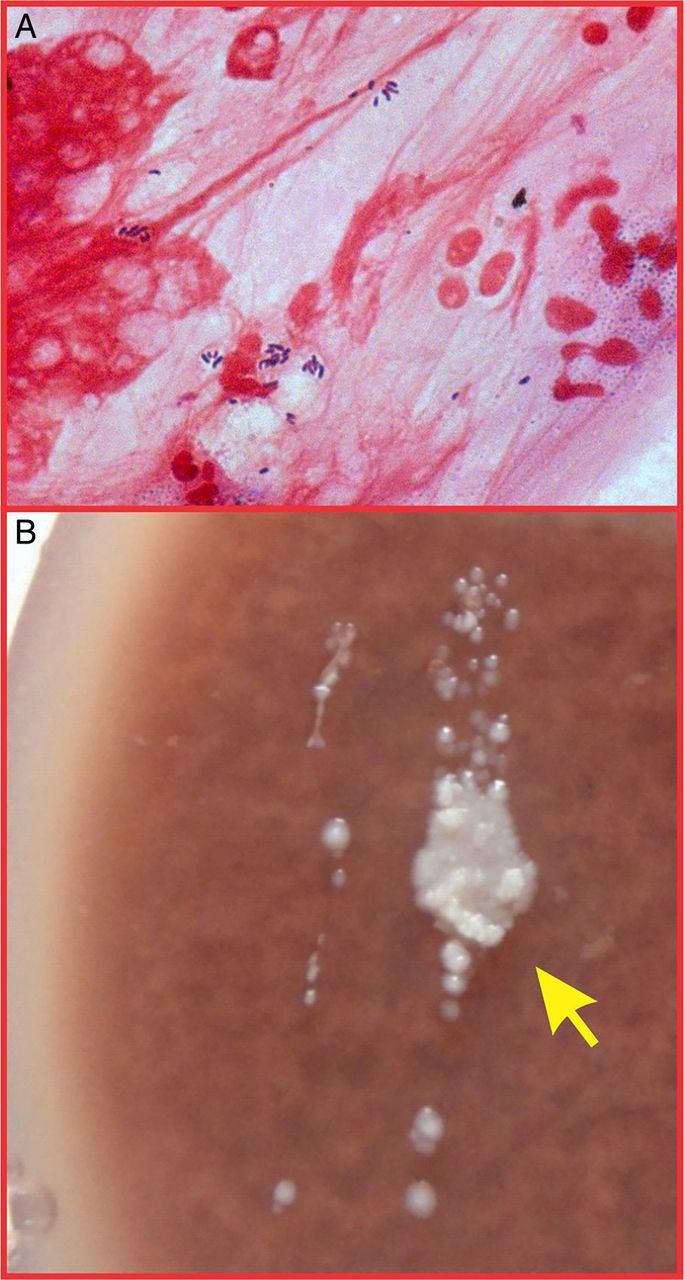
The initial treatment was based on the microscopy results of the corneal scraping (figure 2A). This was continued or modified depending on antibiotic sensitivity report after growth in culture (figure 2B) and/or clinical response. Surgical intervention was planned in cases of non-response to medical management, large infiltrate, thinning and perforation.
{kind=link}
{kind=link}
(A)Corneal scraping showing gram-positive bacilli arranged in Chinese letter pattern suggestive of Corynebacterium spp (Gram stain, ×1000). (B) Tiny, confluent, white, opaque colonies on chocolate agar.
Results
During the study period, of the 1074 clinical samples that were culture positive, Corynebacterium spp was isolated from 101 patients. The majority of the isolates (n=77; 76.2%) were from corneal scrapings of patients with keratitis. Twenty-two cases (M:F :: 15:7) showing significant growth of Corynebacterium spp as sole organism were included in this analysis. Majority of the samples yielded mixed growth. In 15/55 cases, growth of corynebacteria as single organism was not significant. In 37/55 cases, there was mixed growth with corynebacteria that was either significant or not significant. In 3/55 cases, both corynebacteria and other organism were not significant. Analytical Profile Index was done for 6/22 samples. The species identified were C. propinquum (n=3), C. bovis (n=1), C. striatum (n=1) and C. pseudodiphtheriticum (n=1). The mean age of the patients was 43.8±24.4 years (range: 2 months to 82 years). The mean duration of symptoms before presentation was 15.9±12.2 days (range, 1–30 days).
An ocular predisposing factor was present in 14 (63.6%) eyes (table 1). Two patients had diabetes mellitus. Hypopyon was present in six (27.3%) eyes at the initial presentation. One patient had associated endophthalmitis. Case #6 had undergone therapeutic penetrating keratoplasty (TPK) for Pseudomonas keratitis 9 months before presentation that had failed subsequently. Case #7 had presented as graft infiltrate after 16 days of TPK due to fungal aetiology. Case #8 had clear graft during infection. All patients were started with intensive topical fluoroquinolone. Surgical intervention was required in 12 (54.5%) patients. There was no recurrence during follow-up visits. The mean visual acuity (LogMAR) was 2.46 and 2.24 at presentation and at the last follow-up, respectively. Five patients had visual acuity >20/200 at the last follow-up visit.
Epidemiology, risk factor and clinical profile of patients with keratitis caused by Corynebacterium spp
In vitro susceptibility results (table 2) of Corynebacterium spp to vancomycin (17/19, 89.5%), cefazolin (16/20, 80%), chloramphenicol (11/20, 55%), ofloxacin (13/19, 68.4%), ciprofloxacin (10/20, 50%) and gatifloxacin (10/19, 52.6%) were variable. Out of four patients who were found to have drug resistance to fluoroquinolones, two (case #8 and #9) underwent therapeutic keratoplasty after few days of presentation as they worsened. The other two patients were continued with gatifloxacin as they were responding to treatment clinically. While one (case #9) had resistance to chloramphenicol, cefazolin and fluoroquinolone (ciprofloxacin and gatifloxacin), the other (case #20) had resistance to chloramphenicol, cefazolin and vancomycin.
Antibiotics sensitivity profile of Corynebacterium spp
Discussion
The genus Corynebacterium was created by Lehmann and Neumann in 1896 as a taxonomic group to contain the bacterial rods responsible for causing diphtheria. The principal features of the Corynebacterium genus were described by Collins and Cummins in 1986.15 They are gram-positive, catalase-positive, non-spore-forming, non-motile, rod-shaped bacteria that are straight or slightly curved.3 Their size ranges between 2 and 6 µm in length and 0.5 µm in diameter. The bacteria group together in a characteristic way, which has been described as the form of a ‘V’, ‘palisades’ or ‘Chinese letters’. They may also appear elliptical. They are aerobic or facultatively anaerobic, chemoorganotrophs. They are pleomorphic through their life cycles; they occur in various lengths and frequently have thickenings at either end, depending on the surrounding conditions.
The fact that corynebacteria are normal commensal bacteria in conjunctival sac often makes it difficult to assign a pathogenic role to the organisms in causation of ocular infections. However, it is well known that most commensals have the capacity to switch into a pathogenic role given appropriate environment. Fourteen patients had predisposing factors that could account for lowered immunity in the eye. Many of the predisposing factors were related to either ocular surface or eye lid diseases. This is due to the organisms adhering more easily to the abnormal epithelium.
Of all ocular infections, keratitis is the most common ocular infection caused by Corynebacterium spp as seen in our institute. Other ocular manifestations in our experience were conjunctivitis, endophthalmitis, lacrimal abscess, canaliculitis and scleral buckle infection. The most common predisposing factor for keratitis was trauma (27.3%). This was comparable with a study by Schaefer et al, where trauma was a risk factor in 20% cases.9 Bourcier et al have identified trauma as a risk factor in 15% of 300 cases.16
Though Streptococcus pneumoniae infection is known to be commonly associated with nasolacrimal duct obstruction,17 we had two patients in this series with nasolacrimal duct obstruction. C. macginleyi has been earlier reported to be associated with suture related keratitis.8 In our study, one case occurred after therapeutic corneal transplant, where it is contiguous with suture, and another case after corneal tear repair. In both cases (case# 7 and 18), although corneal scraping did not grow fungus in culture, the corneal tissue sent after therapeutic keratoplasty grew fungus. Both patients had deep infiltrate. This indicates that Corynebacterium spp may be present as concomitant infection with other organisms. Similarly, in one case of microsporidial keratoconjunctivitis, the corneal scraping grew Corynebacterium spp.
In our series, 12 patients required adjunctive surgical intervention. Four patients required major surgical intervention, such as therapeutic keratoplasty, of which, two had grown fungus from the corneal tissue. The reason for the severity of these cases might be due to the coexisting fungal infection. However, the other two cases did not grow any organism from the corneal tissue. Postoperatively, there was no recurrence of infection in any of the cases.
Corynebacteria are susceptible to a wide array of antibiotics, such as penicillins, macrolides, rifampicin, gentamicin and fluoroquinolones; however, resistance to antibiotics is also known, which may be species specific. One report from Japan showed that 11 out of 16 C. macginleyi ophthalmic isolates were resistant to fluoroquinolones.18 In this study, drug resistance (more than one drug) was seen in 9 (40.9%) Corynebacterium isolates, of which 2 (22.2%) showed multidrug resistance to 3 or more classes of antibiotics (one resistant to chloramphenicol, cefazolin and vancomycin, while the other resistant to chloramphenicol, cefazolin and fluoroquinolones). Among fluoroquinolones, the least resistance was for ofloxacin (15.8%) and highest for moxifloxacin (36.4%) for Corynebacterium spp in our study.
Our experience suggests that ocular predisposing factors play an important role in the causation of keratitis due to Corynebacterium spp, which can lead to serious corneal infection and may need surgical intervention.
Conclusion
Corynebacteria can cause severe corneal infection requiring surgical intervention.
References
Footnotes
Contributors All the authors included in this paper fulfil the criteria of authorship. Concept and design; analysis and interpretation; writing the article; critical revision of the article; final approval of the article; provision of materials, patients or resources; literature search: SD. Final approval of the article; data collection; provision of materials, patients or resources; literature search: AVSR. Final approval of the article; provision of materials, patients or resources; literature search; administrative, technical or logistic support: SKS. Concept and design; analysis and interpretation; critical revision of the article; final approval of the article; provision of materials, patients or resources; administrative, technical or logistic support: SS.
Funding Hyderabad Eye Research Foundation, Hyderabad.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance