Article Text

Abstract
Aims To determine the diurnal variations of the luminal and stromal areas of the choroid in normal eyes.
Methods This was a prospective observational study of 38 eyes of 38 normal subjects. The blood pressure, heart rate, intraocular pressure and enhanced depth imaging optical coherence tomographic (EDI-OCT) images were recorded every 3 hours between 6:00 and 21:00 hours. The horizontal EDI-OCT images of the subfoveal choroid were converted to binary images. The central choroidal thickness (CCT), total cross-sectional choroidal area, the luminal areas, stromal areas and the ratio of luminal area to total choroidal area (L/C ratio) were determined.
Results There were significant diurnal variations in the CCT, total choroidal area, luminal area and L/C ratio with the maximum values at 6:00 hours and the minimum values at 15:00 hours (p<0.001 for the CCT, p=0.011 for the total choroidal area, p<0.001 for the luminal area and p=0.014 for the L/C ratio). There was no significant variation in the stromal area (p=0.216). The range of fluctuation in the CCT was significantly correlated with that in the luminal area and the total choroidal area (p<0.001). However, there was no significant correlation between the fluctuation range in the CCT and that in the stromal area (p=0.095). There was no statistical relationship between the systemic parameters and the choroidal parameters.
Conclusions The changes in the luminal area are most likely responsible for the diurnal change in the CCT and subfoveal choroidal area.
Trial registration number UMIN000019060, Pre-results.
- Choroid
- Imaging
- Macula
- Physiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Recent studies have shown that the choroid is closely associated with the physiology of the eye and the pathogenesis of various retinal diseases.1–10
Enhanced depth imaging optical coherence tomography (EDI-OCT) and swept-source OCT have enabled clinicians to evaluate the choroidal structure in different kinds of retinal diseases. However, because a layer-by-layer architecture is not distinct, the main structures measured in the OCT images have been the overall choroidal thickness, choroidal area and the shape of the chorioscleral border. Only a limited number of studies have assessed the vascular structure of the choroid which unfortunately used custom-made software not in general use.11 ,12
A new method, called the binarisation method, that can differentiate and quantify the choroidal luminal area from the stromal area was recently published.13 This method uses an open access software named ImageJ with a detailed protocol.13 This method can be used by any researcher with easy accessibility. We used the binarisation technique to differentiate the choroidal luminal area from the stromal area, and we reported that the choroidal thickness and the ratio of luminal area to total choroidal area (L/C ratio) decreased significantly with ageing and longer axial length in normal eyes.14
Recent studies have shown that there is a significant diurnal variation in the choroidal thickness.15–17 To the best of our knowledge, however, there has not been a study to determine whether changes of the luminal or stromal area of the choroid were mainly responsible for the circadian changes in the choroidal thickness. This information should be useful in understanding the physiology in normal eyes and pathogenesis of chorioretinal diseases.
Thus, the purpose of this study was to determine whether there are diurnal variations in the luminal and stromal areas of the choroid using the binarisation technique.
Materials and methods
The procedures used conformed to the tenets of the Declaration of Helsinki, and an informed consent was obtained from all of the subjects. This study was approved by the Institutional Review Board of Tokushima University Hospital and registered with the University Hospital Medical Network (UMIN)-clinical trials registry. The registration title is ‘UMIN000019060, Choroidal structure on EDI-OCT images’ (17 September 2015).
Inclusion and exclusion criteria
This was a prospective, cross-sectional, observational study of 50 right eyes of 50 normal, non-smoking subjects with no ophthalmic or systemic symptoms. The exclusion criteria included the age of <20 and >60 years, high myopia defined as a refractive error (spherical equivalent) of <−6.0 dioptres or an axial length of >26.5 mm, low EDI-OCT image quality defined as an image quality index of <30, abnormal EDI-OCT findings and previous ocular surgeries. Slit-lamp biomicroscopy and indirect ophthalmoscopy were performed to determine whether ocular abnormalities such as corneal diseases, cataracts, vitreoretinal diseases and glaucoma were present. Subjects with any systemic diseases such as hypertension and diabetes mellitus based on the results of their most recent physical examination were also excluded.
Systemic and ophthalmic examinations
The systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate, intraocular pressure (IOP) and EDI-OCT were measured every 3 hours between 6:00 and 21:00 hours. The central corneal thickness, the refractive error and the axial length were measured at 15:00 hours. The SBP, DBP and heart rate were measured on the right arm with a commercial sphygmomanometer (BP-203 RVII, OMRON COLIN, Japan). The mean arterial pressure (MAP) and the mean ocular perfusion pressure (MOPP) were calculated according to the following formulas and used for the analyses: MAP=DBP+1/3 (SBP−DBP) and MOPP=2/3 MAP−IOP. All examinations were performed in the sitting position within 10 min for each subject at each time point.
Spectral-domain optical coherence tomography
Spectral-domain OCT was performed at six-time points with 3-hour intervals; 6:00, 9:00, 12:00, 15:00, 18:00 and 21:00 hours with Spectralis OCT instrument (Heidelberg Engineering, Heidelberg, Germany). Cross-sectional horizontal images of 30° through the fovea were obtained by EDI-OCT for each eye. Each image was recorded with the eye tracking system without pupil dilation, and 100 scans were averaged to improve the signal-to-noise ratio. The Follow-up mode was used to obtain images of the same position of the fundus for each subject. The first scan which was performed at 6:00 hours was set as the reference for each subject. All subsequent scans were aligned to this. All OCT scans were performed by an experienced orthoptist under standardised mesopic lighting conditions to minimise the possible light-evoked vasodilations and constrictions. On the day of the examination, participants were instructed not to take food, drink and vigorous exercise before the initial examination at 6:00 hours, and then to eat according to their usual daily routine thereafter.
The examined area of the retina and choroid was 1500 μm wide and was centred on the fovea. The parameters measured were the central choroidal thickness (CCT), luminal, stromal and total choroidal areas, the central foveal thickness (CFT) and retinal area. The L/C ratio was calculated. The CFT was defined as the distance between internal limiting membrane and the outer surface of the retinal pigment epithelium (RPE), and the CCT as the distance between the outer border of the RPE and the chorioscleral interface. These distances were measured by two independent investigators (KSh and ME) using the calliper function of the measuring software embedded in the Heidelberg Spectralis OCT. The averages of two measurements were used for statistical analyses.
Evaluation of luminal, stromal and total choroidal areas by binarisation technique
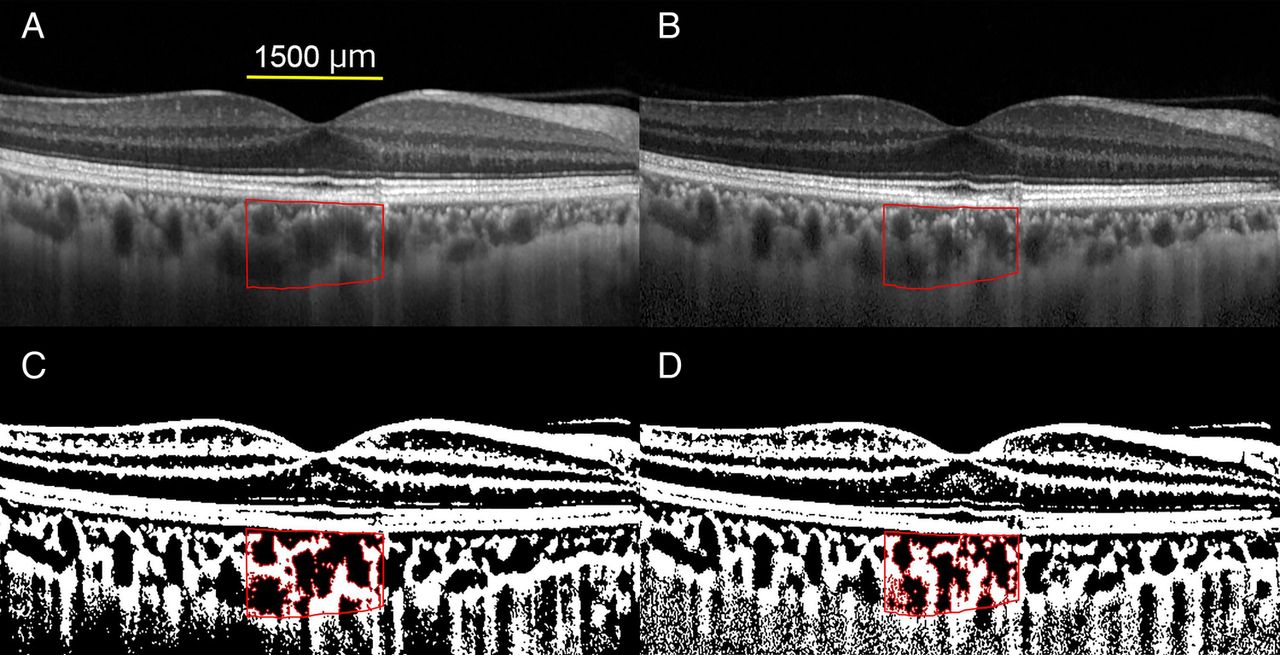
The EDI-OCT images were evaluated by one of the authors (KSh) who was masked to the clinical findings. The binarisation of the choroidal area in the EDI-OCT images was done by a modified Niblack method using the ImageJ software (ImageJ V.1.47, NIH, Bethesda, Maryland, USA) as described in detail (figure 1).13 The examined area was 1500 μm wide and located in the subfoveal choroid, and it extended vertically from the RPE to the chorioscleral border. In the binarised images, the light pixels were defined as the stromal areas and the dark pixels were defined as the luminal areas. After including the distance between each pixel, the luminal and stromal areas were automatically calculated. Similarly, the retinal area of 1500 μm wide centred on the fovea was determined by measuring the area between internal limiting membrane and the outer border of the RPE.

Representative enhanced depth imaging optical coherence tomographic (EDI-OCT) images and converted binary images of a healthy subject. (A and B) Horizontal EDI-OCT images recorded at 6:00 hours (A) and at 15:00 hours (B). The luminal area (dark area) and the stromal area (light area) can be seen. The rectangle surrounded by a red line was excised, and the dark areas were traced by the Niblack method. (C and D) Converted binary images of the EDI-OCT images shown in A (C) and B (D). In the merged binarised images and the margins of traced areas, the light pixels were defined as the stromal area and the dark pixels as the luminal area. The central choroidal thickness (CCT, 325.9 μm), luminal area (330 146.7 μm2) and the ratio of luminal to total choroidal area (L/C ratio, 67.8%) at 6:00 hours were larger than those at 15:00 hours (CCT, 300.7 μm; luminal area, 261 594.3 μm2; L/C ratio, 59.4%).
All parameters were measured three times and the averages were used for the statistical analyses. Although the method for the analysis of the choroid was demonstrated to have a high repeatability and reproducibility in normal eyes,13 intra-rater correlation coefficients were calculated for the data obtained from the images recorded at 6:00 hours. The correlations of the OCT parameters with the systemic parameters and IOP were also determined.
Statistical analyses
Statistical analyses were performed with the SPSS V.22 software (IBM, Armonk, New York, USA). The significances of the diurnal variations in the retinal and choroidal parameters were determined using the repeated-measures analysis of variance with Greenhouse-Geisser corrections. The Bonferroni test was used for post hoc analysis. The correlations in the diurnal variation between choroidal OCT parameters and other parameters including the systemic parameters and IOP were determined by calculating the within-subject correlation coefficients using a general linear model.18 The intra-rater correlation coefficients were calculated using one-way random effects model for measurements of agreement. The inter-rater correlation coefficients were calculated using two-way mixed effects model for measurements of absolute agreement. A two-sided p value of <0.05 was considered statistically significant.
Results
Baseline demographic data
Fifty subjects consisting of 28 men and 22 women were studied. Eleven eyes of 11 subjects were excluded because of high myopia and one eye because of prior laser in situ keratomileusis. No eye was excluded because of low image quality. Thus, the data from 38 eyes of 38 subjects (20 men and 18 women) were used for the statistical analyses. The age of the subjects ranged from 21 to 52 years (mean±SD, 30.5±9.11 years). The axial length, the refractive errors and the central corneal thickness (mean±SD) were 24.5±1.07 mm, −2.8±2.07 dioptres and 537.3±31.18 μm, respectively.
Repeatability of measurement of OCT parameters
The intra-rater agreement was high, with an intraclass correlation coefficient of 0.997(CI 0.994 to 0.998) for the total choroidal area, 0.996 (CI 0.993 to 0.998) for the luminal area, 0.964 (CI 0.939 to 0.980) for the stromal area and 0.974 (CI 0.956 to 0.986) for the L/C ratio. The inter-rater agreement for the CCT and CFT were 0.997 (CI 0.994 to 0.998) and 0.994 (CI 0.989 to 0.997), respectively.
Diurnal variations in optical coherence tomographic parameters
Significant diurnal variations were observed in the mean CCT, the mean total choroidal area, the mean luminal area and the mean L/C ratio with the maximum values at 6:00 hours; 359.0±76.2 μm for the mean CCT, 535 243.1±113 295.7 μm2 for the mean total choroidal area, 352 586.1±113 295.7 μm2 for the mean luminal area and 65.2±4.13% of the mean L/C ratio (figure 2). The minimum values were found at 15:00 hours; 341.2±70.1 μm for the mean CCT (p<0.001), 508 696.8±104 240.4 μm2 for the mean total choroidal area (p=0.011), 330 806.8±85 029.5 μm2 for the mean luminal area (p<0.001) and 64.2±3.91% for the mean L/C ratio (p=0.014).

Diurnal variations in the choroidal structural parameters. There were significant diurnal variations in the central choroidal thickness, total choroidal area, luminal area and the ratio of luminal area to total choroidal area. There was no significant diurnal variation in the stromal area and the retinal area.
The mean stromal area was largest at 6:00 hours with a value of 182 657.0±25 959.9 μm2 and smallest at 21:00 hours with a value of 179 053.2±25 255.9 μm2. However, the difference was not statistically significant (p=0.216). There was no significant variation in the CFT and the retinal area (p=0.497 and p=0.441, respectively).
The difference in the CCT between 6:00 and 15:00 hours was significantly correlated with the differences in the total choroidal area (r=0.972, p<0.001) and luminal area (r=0.767, p<0.001) in the partial regression coefficient in which the refractive error and age were set as the control variables (figure 3). However, there was no correlation between the fluctuation range in the CCT and that in the stromal area (r=0.287, p=0.095).
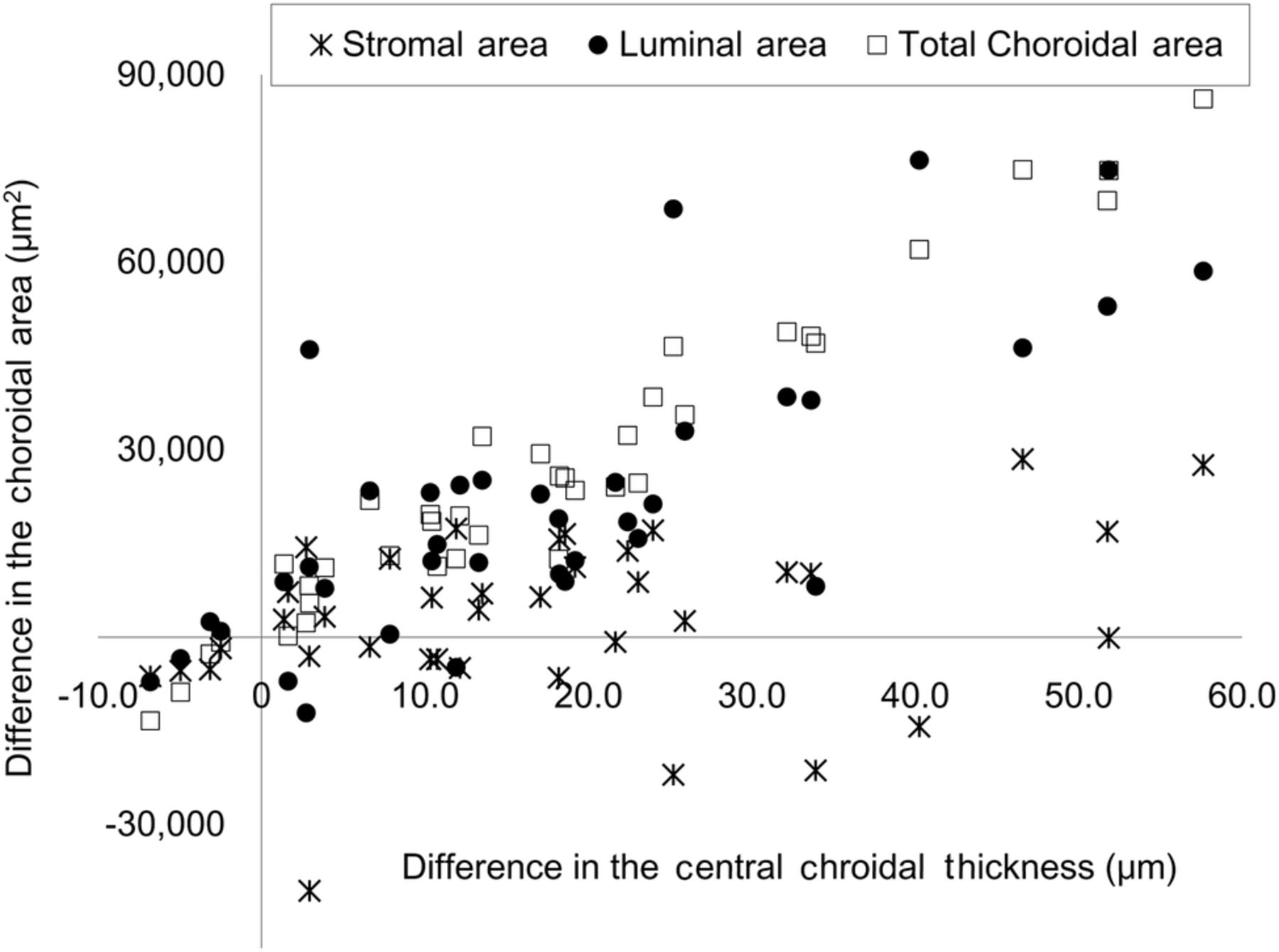
Scatter plots showing the associations between the fluctuation range in the central choroidal thickness and those in the choroidal areas. The difference in the central choroidal thickness between 6:00 and 15:00 hours was correlated with the difference in the total choroidal area and that in the luminal area, but not with that in the stromal area.
Diurnal variations in the systemic parameters and intraocular pressure
None of the subjects had an IOP >20 mm Hg at any time.
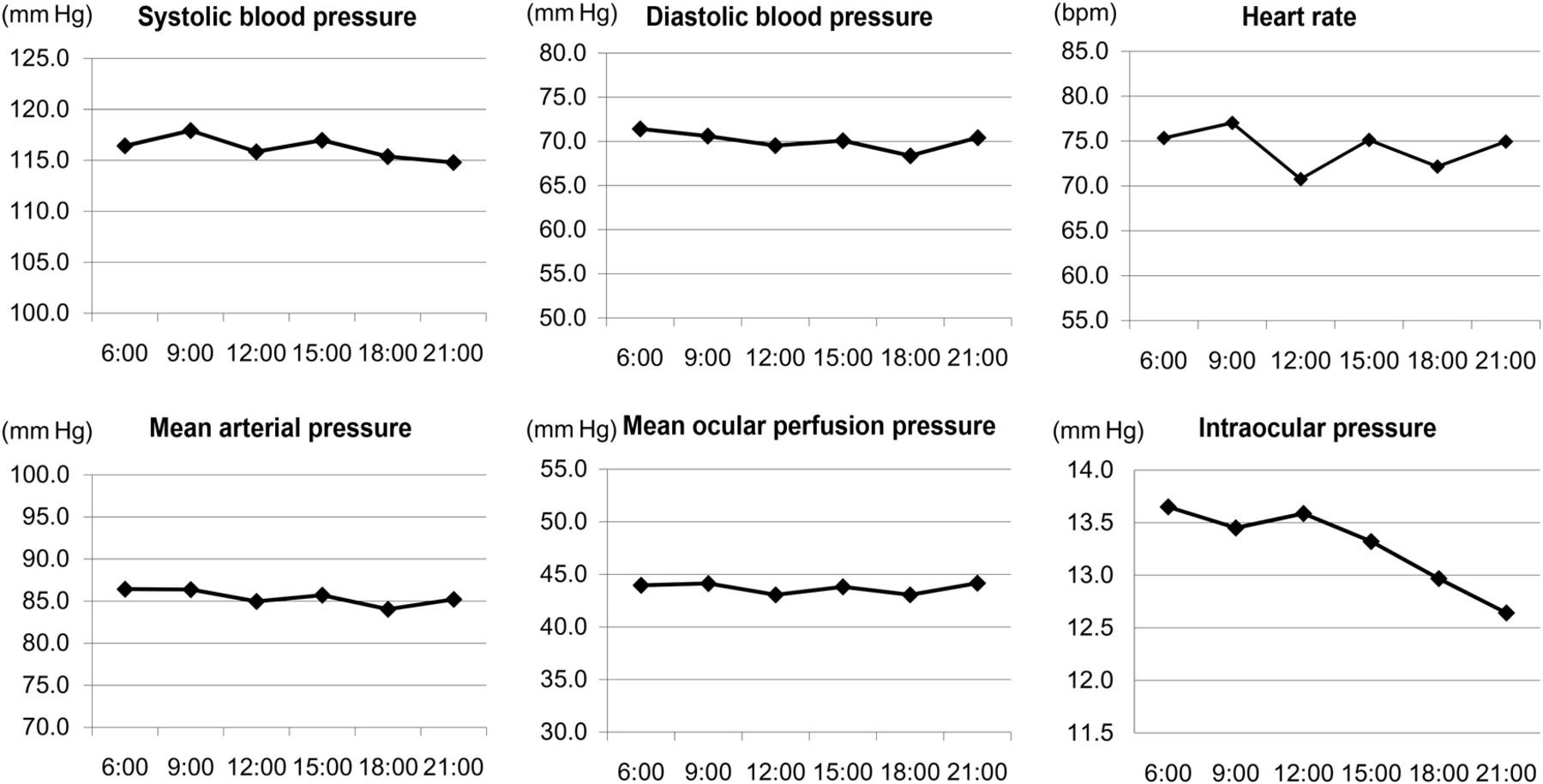
There were no significant diurnal variations in the mean SBP, DBP, MAP and MOPP (p=0.434, p=0.088, p=0.268 and p=0.501, respectively; figure 4). There were significant diurnal variations in the mean heart rate (p=0.002) and IOP (p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diurnal variations in the systemic parameters and intraocular pressure. There was no significant diurnal variations in the mean systolic blood pressure, diastolic blood pressure, mean arterial pressure and mean ocular perfusion pressure. There were significant diurnal variations in the mean heart rate and intraocular pressure.
Correlations of OCT parameters with systemic parameters and intraocular pressure
There were several significant correlations in the diurnal variations between the OCT parameters and the DBP, MAP and IOP but they were not relevant (all |r|<0.2, table 1).
Correlations of OCT parameters with systemic parameters and IOP
Discussion
Our results showed that there were significant diurnal variations in the CCT, total choroidal area and the luminal area. These parameters were maximal at 6:00 hours, decreased during the day to the minimum values at 15:00 hours and then increased in the evening. These variations are similar to the diurnal variations in the CCT reported in other studies.16 ,17 Our results demonstrated that the choroidal thickness at the fovea and the macular choroidal area had significant diurnal variations.
Importantly, the fluctuations in the stromal area were not significant as well as CFT and retinal area which were used as negative controls. On the other hand, the L/C ratio had significant diurnal variations. The change in the CCT was significantly correlated with the change in the luminal area and the total choroidal area. However, there was no correlation between the change in the CCT and that in the stromal area. These results suggest that such fluctuations are mainly due to the diurnal variations in the luminal area. At present, there are reports on the diurnal variations in the choroidal thickness and choroidal circulatory parameters,15 ,16 ,19 ,20 which make clinicians speculate that the diurnal variation in the choroidal thickness should be related to the diurnal circulatory fluctuations. To the best of our knowledge; however, this is the first report which determined that the diurnal variations in the choroidal thickness and choroidal area should not be attributed to the variation in the stromal area but to the luminal area.
The vascular tone and diameters can be altered by various factors including the blood pressure and myogenic responses, metabolic influences, for example blood gases and pH, visual stimulation and vasoactive agents including angiotensin II and nitric oxide.21 Usui et al16 reported a significant negative correlation between the choroidal thickness and SBP during the diurnal variations in these two parameters. Tan et al15 reported a significant correlation between the change in the choroidal thickness and the change in the SBP. On the other hand, Li et al22 reported that they found no significant correlation between the SBP or DBP and the choroidal thickness. Our results also showed no statistical relationship between the blood pressure and the choroidal parameters. Although the reason for this discrepancy was not determined, the choroidal vessels are under neurogenic control, and the autoregulation of choroidal blood flow is restricted compared with that of the retina.21 The degree of fluctuations in the systemic parameters including SBP, DBP, MAP and MOPP were small with no statistical significance. This may explain the discrepancy between the earlier studies and ours. Another possible explanation could be that diurnal variations in the choroid may be influenced by other factors than that examined in this study. Further studies are needed to determine the relationship between choroidal circulatory and structural parameters.
Changes in the IOP could also influence the choroidal parameters. A recent report showed that the diurnal fluctuation of the IOP and choroidal thickness were out of phase,17 but no correlation was detected in another report.16 In this study, no statistical correlation was found between the choroidal parameters and the IOP. The amplitude of the diurnal fluctuations in the mean IOP was approximately 1.0 mm Hg. A significant correlation may not have been detected because of the small range of IOP fluctuations.
Evaluating the choroidal structure including the L/C ratio should be useful for understanding the pathogenesis of chorioretinal diseases as we reported recently.13 ,23 ,24 However, careful attention should be paid to the diurnal variations in the choroidal structure when evaluating the choroidal structure in various chorioretinal diseases.
There are some limitations in this study. First, we did not examine the 24-hour diurnal variations. The L/C ratio during midnight might provide some new information in the future. Second, the scanned area of 1500 μm was not enough to assume the diurnal variation of the whole choroid. A wider range of the examination area may be more conclusive.
In conclusion, there are significant diurnal variations in the total choroidal area, luminal area and the L/C ratio but not in the stromal area. These findings indicate that the diurnal variations in the choroidal area are mainly due to the fluctuations in the luminal area.
Acknowledgments
The authors thank Professor Emeritus Duco Hamasaki of the Bascom Palmer Eye Institute of the University of Miami for providing critical discussions and suggestions for our study and revision of the manuscript.
References
Footnotes
Contributors All authors have given final approval of this version to be published. Design of the study: TK, YM, ME, SS and TS. Conduct of the study: TK, YM, KSh and ME. Management of the data: YM, KSh, AI, AF, YO, KSe and KA. Analysis of the data: TK, YM, KSh, ME, KSe, EU and SS. Interpretation of the data: TK, YM, KSh, ME, AI, AF, YO, KSe, KA, SS and TS. Preparation of the manuscript: TK, YM, EU, SS and TS. Overall coordination: TS.
Funding This work was supported in part by grant-in-aid 16K11288 (to YM) from the Ministry of Education, Science, Sports and Culture, Japan.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Institutional Review Board of Tokushima University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available from the corresponding author upon request.
Linked Articles
- At a glance