Article Text

Abstract
Background To determine whether the internal limiting membrane (ILM) insertion technique is as effective as the inverted ILM flap technique for the initial surgical treatment of eyes with large idiopathic macular holes (MHs).
Methods This retrospective, non-randomised, comparative clinical study included 41 eyes with large MHs (minimum diameter >500 µm) that were treated using the ILM insertion technique or the inverted ILM flap technique. The hole closure rate, postoperative best corrected visual acuity (BCVA) and swept source optical coherence tomography findings were analysed at 6 months after surgery.
Results There were 15 and 26 eyes in the insertion and inverted flap groups, respectively. Hole closure was achieved in all eyes. The mean final BCVA was better in the inverted flap group than in the insertion group (0.527 vs 0.773, p=0.006), although significant postoperative improvements were observed in both groups (p<0.001). Postoperative foveal discolouration was more common in the insertion group than in the inverted flap group (86.7% vs 7.7%, p<0.001). Complete resolution of ellipsoid zone and external limiting membrane defects was observed in 7 and 18 eyes, respectively, in the inverted flap group; in contrast, complete resolution was not observed in any of the eyes in the insertion group (p=0.035 and p<0.001, respectively).
Conclusion The ILM insertion technique may be as effective as the inverted ILM flap technique for the closure of large MHs. However, the latter technique results in better recovery of photoreceptor layers and, consequently, better postoperative visual acuity.
- internal limiting membrane
- inverted flap
- large macular hole
- optical coherence tomography
- visual acuity
Statistics from Altmetric.com
Introduction
Idiopathic macular holes (MHs) can be successfully closed by vitrectomy, internal limiting membrane (ILM) peeling and gas tamponade, which provide major visual improvements in most cases.1–5 However, the surgical closure rate is relatively low in complicated cases, such as large MHs, myopic MHs or MHs that are refractory to primary surgery.6–9 Recently, several techniques have been introduced that use the inverted ILM flap to improve anatomical and visual outcomes in complicated MH cases.10–14 These inverted ILM flap techniques may facilitate the proliferation of glial cells, which then fill the hole and facilitate its closure. However, these techniques are not indicated for eyes with previous ILM removal around the hole. To overcome this limitation, Morizane et al 15 directly transplanted an ILM sheet inside the hole, following the creation of a free flap at the peripheral macula. This ILM insertion technique has reportedly achieved successful anatomical and visual outcomes in cases of refractory MHs13 16 and has been applied for the initial treatment of large MHs.17 18
However, there are potential problems regarding the direct insertion of an ILM sheet into the MH, including the possibility of damage to the retinal pigment epithelium (RPE) in the fovea. We recently evaluated the microstructure of the fovea following ILM insertion into large MHs in a small case series18; we found foveal discolouration and incomplete recovery of the photoreceptor layers in all eyes with hole closure, although the visual acuity improved in these eyes. However, the heterogeneous features of MHs, including both MHs that are refractory to initial surgery and treatment-naïve large MHs, may limit understanding of the effects of the ILM insertion technique on postoperative outcomes. Moreover, there is a paucity of literature regarding surgical outcomes associated with ILM insertion as the initial surgical technique for large MHs.
The aim of the present study was to determine the comparative efficacies of the ILM insertion technique and the inverted ILM flap technique for the initial surgical treatment of eyes with large idiopathic MHs.
Methods
Patient inclusion and exclusion criteria
This retrospective, interventional, comparative study included patients with idiopathic MHs (minimum diameter >500 µm) who underwent vitrectomy, with either the ILM insertion technique or the inverted ILM flap technique, at the vitreoretinal services of Pusan National University Hospital and Pusan National University Yangsan Hospital, South Korea, from August 2014 to March 2016. All patients were followed for at least 6 months after surgery. Patients were excluded if they had a history of ocular surgery or diabetic retinopathy, or if they exhibited high myopia (a spherical equivalent ≥−6.0 dioptre or an axial length ≥26.5 mm) or retinal detachment associated with MHs. Patients with media opacities, including cataracts, were also excluded, in order to ensure detailed and accurate image analysis.
Each patient was informed about the risks and benefits of the surgery, and written informed consent was obtained. This study adhered to the tenets of the Declaration of Helsinki.
Surgical procedures
Pars plana vitrectomy was performed by one of three expert surgeons (SWP, JEL, ISB) using the sutureless, 25-gauge vitrectomy system (Constellation, Alcon Laboratories, Fort Worth, Texas, USA) and the non-contact viewing system (Resight 700, Carl Zeiss Meditec, Jena, Germany). Phacoemulsification and intraocular lens implantation were performed simultaneously in all cases. On the basis of the type of surgical technique used, patients were divided into an insertion group and an inverted flap group. The surgical procedures were selected by the surgeons.
The surgical procedures for the two groups were as follows. In the insertion group, we peeled off >2 disc areas of the ILM around the hole, following removal of the core and posterior cortical vitreous. The peeled ILM flap was trimmed and placed inside the hole using intraocular forceps. The quantity of ILM used for the insertion depended on the minimum MH diameter in each patient. After confirmation of appropriate positioning of the transplanted ILM pieces inside the hole, fluid-air exchange was slowly performed. In the inverted flap group, we inverted approximately one disc area of the ILM attached to the superior margin of MH in order to cover the hole, then placed perfluoro-n-octane (Perfluoron, Alcon Laboratories) on the flap to maintain the position of the ILM sheet; we left a small amount without lavage at the completion of air-fluid exchange. The residual perfluoro-n-octane liquid was eliminated by evaporation.14 During both surgical procedures, the ILM was stained with 0.025% Brilliant Blue G (BBG; Sigma-Aldrich, St Louis, Missouri, USA).
At the end of surgery, the vitreous cavity was filled with 18% sulfur hexafluoride, depending on the condition. All patients assumed a face-down position for >3 days and were discharged after MH closure was ascertained via swept source optical coherence tomography (SS-OCT; DRI OCT-1 Atlantis; Topcon, Tokyo, Japan) imaging. Anatomical success was defined as complete MH closure, visible on the SS-OCT images.
Ocular parameters
The patients underwent comprehensive ophthalmological examinations, including best corrected visual acuity (BCVA) measurements, indirect ophthalmoscopy, fundus photography (Canon CR-2 digital non-mydriatic retinal camera, Canon, Tokyo, Japan) and SS-OCT; these examinations were performed at baseline, as well as at 1, 3 and 6 months postoperatively. BCVA was measured using the Snellen chart and converted to the logarithm of the minimum angle of resolution (logMAR) scale for statistical analysis.
The minimum and base diameters of the MHs, as well as hole closure, foveal configuration and the sizes of ellipsoid zone (EZ) and external limiting membrane (ELM) defects, were assessed by SS-OCT. The scan protocol comprised a 12 mm×9 mm-wide, three-dimensional (3D) volumetric scan, consisting of 512×256 A-scans and 9 mm radial images obtained in the 5 Line Cross mode with 0.25 mm spacing in both the horizontal and vertical directions. The 3D macular scan images were used to determine the foveal configuration following hole closure, whereas the 5 Line Cross images were used to measure the hole diameter and defects in both the EZ and ELM. The foveal configuration was characterised as U-shaped, V-shaped, W-shaped or open.13 19–21 The U shape was defined as a contour similar to that of a healthy fovea, whereas the V shape was defined as a steep contour with a thin fovea centralis. The W shape was a closed but irregular contour that could not be defined as the U shape or the V shape. Using the embedded manual calliper function of the OCT machine, the hole diameter and the EZ and ELM defects were measured, using a line drawn roughly parallel to the RPE. The sizes of the holes were calculated by averaging the vertical and horizontal diameters at the narrowest area of each hole. EZ and ELM defect sizes were calculated by averaging the vertical and horizontal discontinuous lengths of the hyper-reflective lines corresponding to the EZ and ELM.
Statistical analysis
Changes in BCVA and the EZ and ELM defects after surgery were analysed using the Wilcoxon signed-rank test. Age, BCVA, minimum and base hole diameters, and EZ and ELM defect sizes were compared between the two groups using Mann-Whitney U tests; the postoperative foveal configuration and foveal discolouration were compared using linear-by-linear association and Fisher’s exact test. All statistical analyses were performed using SPSS V.22.0 for Windows. A p value of <0.05 was considered to be statistically significant.
Results
A total of 41 eyes were included in this study; 15 eyes comprised the insertion group, whereas 26 eyes comprised the inverted flap group. Baseline characteristics, including age (66.3 vs 65.7 years, respectively), BCVA (1.2 vs 1.0 logMAR, respectively), minimum hole diameter (662.1 μm vs 657.1 μm, respectively), base hole diameter (1016.2 μm vs 1028.9 μm, respectively), EZ defect size (1308.5 μm vs 1225.4 μm, respectively) and ELM defect size (1077.0 μm vs 1012.1 μm, respectively), revealed no significant differences between the insertion and inverted flap groups (table 1).
Baseline characteristics
MH closure and postoperative foveal configuration
Postoperative OCT scans confirmed MH closure in all eyes (figures 1 and 2). At 6 months postoperatively, the foveal configuration in the insertion group was identified as U-shaped in nine eyes (60.0%), V-shaped in two eyes (13.3%) and W-shaped in four eyes (26.7%). In the inverted flap group, 20 (76.9%), 2 (7.7%) and 4 (15.4%) eyes demonstrated U-shaped, V-shaped and W-shaped foveas, respectively. The foveal configuration following hole closure was not significantly different between the two groups (table 2).

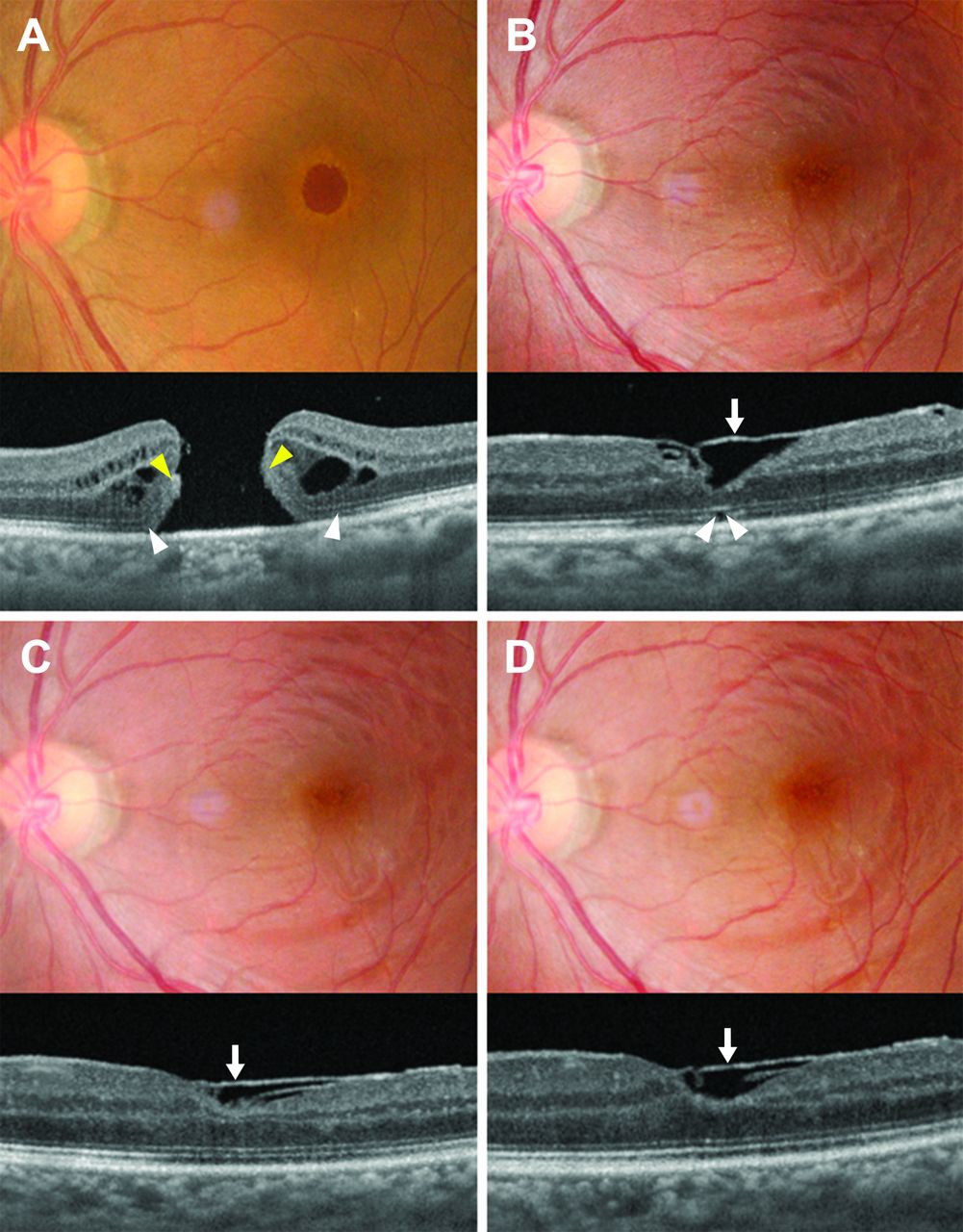
Representative case of a large macular hole that was treated by internal limiting membrane (ILM) insertion. (A) Baseline fundus photographs showed a large full-thickness macular hole. Optical coherence tomography (OCT) showed a large hole with a minimum diameter of 758 µm. The defects in the ellipsoid zone (EZ, white arrowhead) and external limiting membrane (ELM, yellow arrowhead) measured 1809.5 µm and 1746.5 µm, respectively. (B) At 1 month after vitrectomy and ILM insertion, hole closure was visible on fundus photography. OCT showed that the fovea was completely filled with glial tissues (white arrow). (C,D) Foveal discolouration developed and progressed over 3 and 6 months after vitrectomy, respectively. OCT showed an improvement in the foveal configuration, accompanied by continuous glial proliferation (white arrow). The EZ and ELM defects decreased to 1093 µm and 828 µm, respectively, although complete resolution was not observed at 6 months. The best corrected visual acuity improved from 20/200 to 20/100.

Representative case of a large macular hole that was treated by the inverted internal limiting membrane (ILM) flap technique. (A) Baseline fundus photographs showed a large full-thickness macular hole. Optical coherence tomography (OCT) showed a large hole with a minimum diameter of 579 µm. The defects in the ellipsoid zone (EZ, white arrowhead) and external limiting membrane (ELM, yellow arrowhead) measured 1162 µm and 860.5 µm, respectively. (B) At 1 month after surgery using the inverted ILM flap technique, hole closure was visible on a fundus photograph. OCT showed resolution of the ELM and EZ defects. The inverted ILM flap was visible over the fovea (white arrow). (C,D) The foveal contour improved over 3 and 6 months after surgery using the inverted ILM flap technique, and the EZ and ELM defects were completely resolved. The best corrected visual acuity improved from 20/125 to 20/40.
Foveal features on fundus photography and optical coherence tomography, compared between insertion and inverted flap groups
Foveal discolouration was observed in 13 eyes (86.7%) in the insertion group and 2 eyes (7.7%) in the inverted flap group; thus, there was significantly more foveal discolouration in the insertion group than in the inverted flap group (p<0.001). SS-OCT images showed that the fovea was filled with amorphous tissues, such as glial tissues, in eyes exhibiting foveal discolouration (figure 1).
Postoperative EZ and ELM defects
Cross-sectional OCT images demonstrated a significant decrease in the sizes of EZ and ELM defects over time in both groups (figure 3). At 6 months, the mean EZ defect size was 761.1±417.9 µm in the insertion group and 192.0±274.8 µm in the inverted flap group, whereas the mean ELM defect sizes were 550.0±267.7 µm and 80.5±140.3 µm, respectively. Significant improvements in EZ and ELM defects were observed in both groups (p<0.001 and p<0.001, respectively, compared with the baseline size). The mean EZ and ELM defects were significantly smaller in the inverted flap group than in the insertion group (p<0.001 and p<0.001, respectively).

Graphs showing changes in the ellipsoid zone (EZ) and external limiting membrane (ELM) defects after large macular hole surgery using the internal limiting membrane (ILM) insertion technique (solid line) or the inverted ILM flap technique (dashed line). The mean EZ and ELM defect sizes significantly reduced after surgery in both groups (p<0.001 and p<0.001, respectively). Defect resolution was significantly better in the inverted flap group than in the insertion group (p<0.001 and p<0.001, respectively). The error bars indicate SD. *P<0.05 between the two groups.
Complete recovery of the EZ and ELM was observed in 7 and 18 eyes, respectively, in the inverted flap group. However, none of the eyes in the insertion group exhibited complete recovery of the EZ and ELM until 6 months postoperatively. Therefore, complete recovery of EZ and ELM differed significantly between the two groups (p=0.035 and p<0.001, respectively).
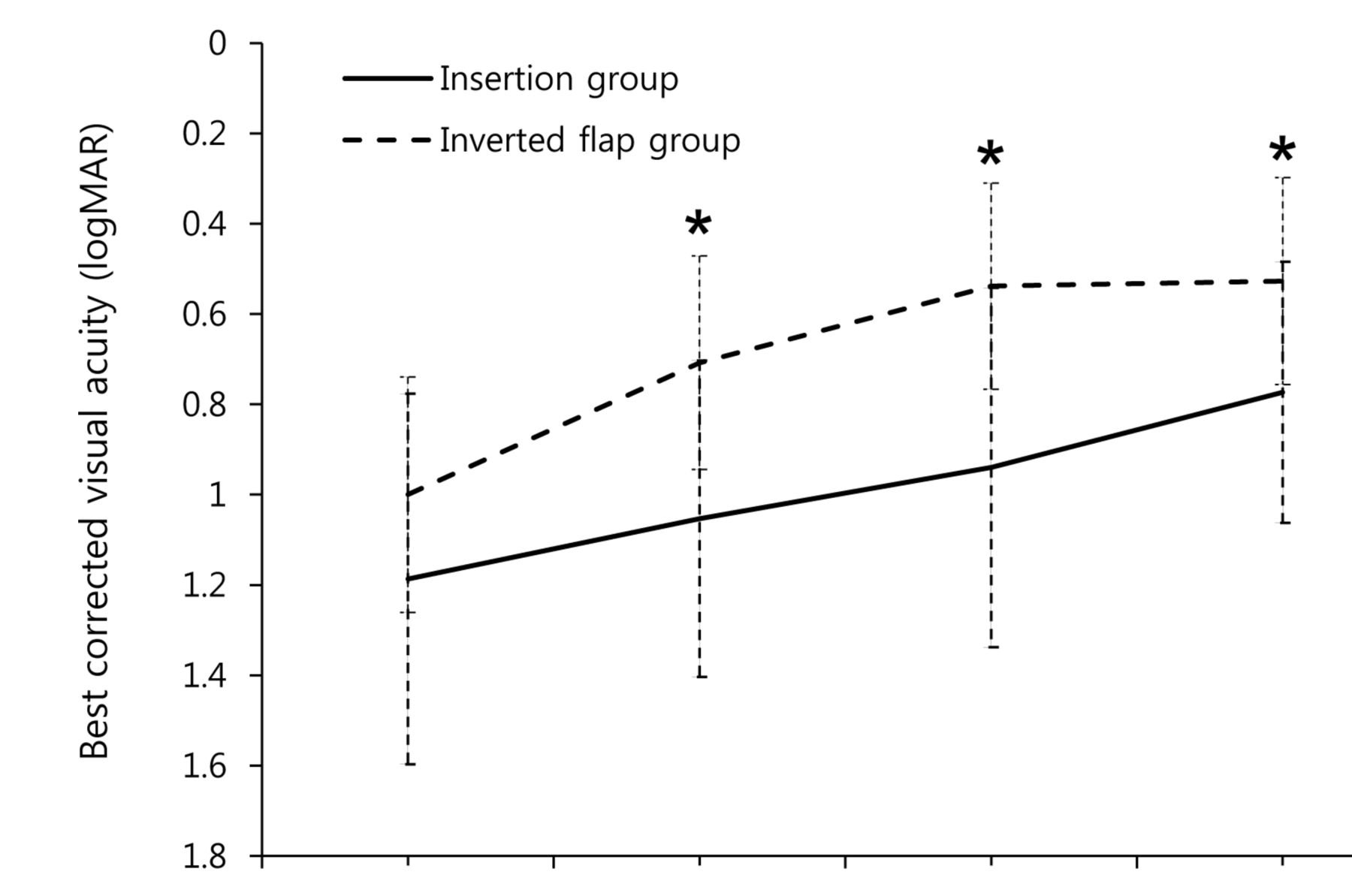
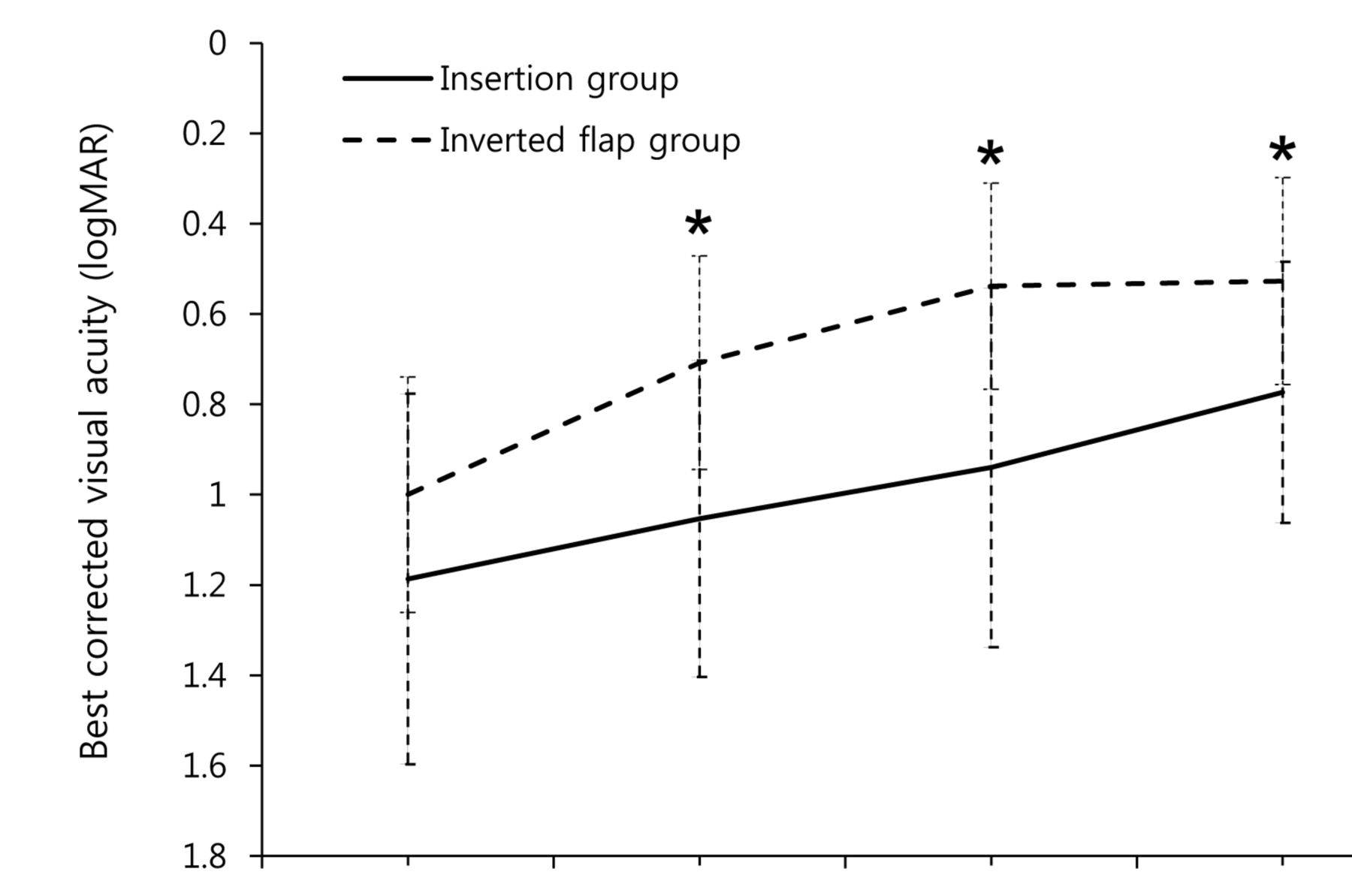
Changes in visual acuity
The mean BCVA was 0.773 logMAR in the insertion group and 0.527 logMAR in the inverted flap group at 6 months; BCVA significantly improved in both groups (p<0.001 and p=0.010, respectively). However, the postoperative BCVA was better in the inverted flap group than in the insertion group throughout the follow-up period (p=0.001, p=0.001 and p=0.006 at 1, 3 and 6 months, respectively; figure 4). An improvement of two lines or more was observed for 13 eyes (86.7%) in the insertion group and 24 eyes (92.3%) in the inverted flap group; this improvement did not significantly differ between the two groups.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph showing changes in the mean best corrected visual acuity (BCVA; logarithm of the minimum angle of resolution (logMAR)) after large macular hole surgery using the internal limiting membrane (ILM) insertion technique (solid line) or the inverted ILM flap technique (dashed line). BCVA significantly improved after surgery in both groups (p<0.001 and p=0.010, respectively). However, the inverted flap group exhibited better values than the insertion group at every follow-up visit after surgery (p<0.001). The error bars indicate SD. *P<0.05 between the two groups.
Discussion
The current study revealed the efficacy of the ILM insertion technique for the initial surgical treatment of eyes with large idiopathic MHs; this technique exhibited similar efficacy to the inverted ILM flap technique. Both surgical techniques achieved a high closure rate and significant visual improvements in eyes with large MHs. A U-shaped foveal configuration was the most common outcome. Longitudinal SS-OCT images revealed significant reductions in the sizes of EZ and ELM defects. BCVA significantly improved in both groups, although the postoperative BCVA and photoreceptor layer integrity were superior in the inverted flap group, relative to the insertion group.
Since Kelly and Wendel22 first described pars plana vitrectomy for the treatment of MHs, additional ILM peeling has achieved a high success rate.5 However, a low closure rate has been reported for large MHs (minimum diameter ≥500 µm), even in cases treated with extensive ILM peeling.6 23 Michalewska et al 11 reported that the inverted ILM flap technique results in a high closure rate for eyes with large MHs. Since then, modified techniques using the inverted ILM flap have been described, which result in favourable surgical outcomes.10 12 14 During this surgical procedure, it is important to retain the attachment of the ILM flap with the hole margin. To prevent accidental ILM detachment, we used the perfluoro-n-octane-assisted inverted ILM flap technique in the present study. We previously reported the usefulness of perfluoro-n-octane to settle the ILM flap over the hole in eyes with large or refractory MHs.14 24
The ILM insertion technique, which involves insertion of the ILM into the MH, was first introduced by Morizane et al 15 for eyes with MHs that were refractory to previous ILM peeling surgery. Subsequently, De Novelli et al 17 performed the ILM insertion technique as an initial surgery for eyes with large and chronic MHs. Whereas Morizane et al 15 placed viscoelastic material over the free flap for stabilisation, De Novelli et al 17 slowly removed the fluid to prevent dislodging of the ILM sheet from the hole. In the present study, we performed slow fluid-air exchange to retain the ILM sheet inside the hole. Previous studies15–18 have shown a hole closure rate of >90% and significant visual improvements for eyes with large and/or refractory MHs that were treated with the ILM insertion technique. In the present study, all eyes in both groups achieved successful hole closure without loss of the ILM sheet.
The commonly suggested mechanism for MH closure is as follows. Macrophage-like cells, which are stimulated when the retina is mechanically damaged by ILM peeling, may infiltrate the retinal tissue and activate Müller cells, thereby inducing glial cell proliferation that facilitates hole closure.25–28 In the inverted ILM flap technique, preservation of the ILM, which contains Müller cells, around the hole margin can help induce gliosis and provide a scaffold for glial cell proliferation, thereby facilitating the closure of large holes.11–13 29 Inserted ILM pieces inside holes may play a role similar to that played by inverted ILM flaps placed over the hole in the process of large hole closure. Moreover, long-lasting glial cell proliferation can be stimulated by the ILM sheet after hole closure; this may result in a favourable, U-shaped foveal contour. In the present study, a high closure rate was observed; further, a U-shaped fovea was observed in 63.6% of eyes in the insertion group and 76.9% of eyes in the inverted flap group. Both rates were relatively higher than those (43%–60%) reported following conventional ILM peeling for large MHs.19 20 23 We found no significant differences between the insertion and inverted flap groups, in terms of the hole closure rate and foveal configuration, and our anatomical results reinforced the efficacy of both techniques for the initial surgical treatment of large MHs.30
Despite the high closure rate for large MHs, there are several concerns related to the insertion of an ILM inside hole. First, the ILM pieces transplanted inside holes may become a barrier against the approximation of the neurosensory retina and the rearrangement of photoreceptor cells, even though the ILM pieces assist in hole closure. In the present study, prominent glial tissues were observed in the fovea following hole closure in the insertion group. No eyes showed complete recovery of the photoreceptor layers indicating EZ and ELM integrity in the fovea. Second, the RPE can be damaged: when the ILM piece is inserted into the MH, the RPE can be mechanically injured. Moreover, the safety of 0.025% BBG has been reported only for short-term use in peeling of the ILM.31 Direct, long-term contact between BBG-stained ILM and the RPE may induce chemical damage within the RPE. In a previous study, RPE atrophy was reported in 2 of 10 eyes (20%) that underwent the ILM insertion technique.17 In the present study, foveal discolouration was more common in the insertion group (86.7%) than in the inverted flap group (7.7%). The above-mentioned findings may account for the better postoperative BCVA in the inverted flap group, relative to that in the insertion group. We previously evaluated the microstructural changes that followed use of the ILM insertion technique for eyes with refractory MHs and large MHs. In this small case series, we found incomplete recovery of photoreceptor layers and foveal discolouration.18
The limitations of our study include its retrospective nature, a small sample size, a relatively short follow-up period and possible bias from the surgeon factor. Nevertheless, our findings can suggest a new information for the ILM insertion technique in the initial surgery for large MHs, compared with the inverted ILM flap technique.
In summary, we found that the insertion of ILM sheets inside hole may be as effective as the inverted ILM flap technique for the initial surgical treatment of eyes with large MHs, to achieve the hole closure. However, the latter technique results in better recovery of the photoreceptor layers and, consequently, superior postoperative visual acuity. Therefore, the inverted flap technique is recommended as the preferred surgical technique for initial treatment in large MHs.
References
Footnotes
Contributors Design and conduct of study: JEL and ISB; data collection: JHP, SML, SWP, JEL, and ISB; data management, analysis, and interpretation: JHP, SML, SWP, JEL, and ISB; and manuscript preparation, review, and approval: JHP, SML, SWP, JEL, and ISB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (approval no PNUYH 05-2017-092).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance