Article Text

Abstract
Background/Aims Locally advanced (T4 per American Joint Committee on Cancer (AJCC) 8th edition) periocular basal cell carcinoma (BCC) can lead to loss of the eye. We report the neoadjuvant use of vismodegib followed by surgery in patients with such lesions with eye preservation as primary goal.
Methods This retrospective interventional study includes all patients with a T4 periocular BCC (per 8th edition AJCC for eyelid carcinoma) treated by the senior author between 2013 and 2017 with neoadjuvant vismodegib prior to definitive surgery.
Results Eight patients had a T4 tumour. Six patients presented with recurrent disease. Indications for neoadjuvant treatment were an unresectable tumour in one patient, an attempt to avoid an orbital exenteration in six patients and an attempt to avoid disfiguring facial surgery in one patient. Patients were treated for a median of 14 months (range: 4–36 months). All patients underwent an eye-sparing surgery following neoadjuvant vismodegib and all final surgical margins were negative for tumour. Five patients had a complete response to vismodegib with no microscopic residual BCC found during surgery; three patients had a significant partial response with residual tumour found on pathology. At last follow-up, a mean of 18 (range: 6–43) months after surgery, all patients were off-vismodegib and alive without evidence of disease.
Conclusions Neoadjuvant vismodegib for locally advanced (T4) periocular BCC enabled an eye-sparing surgery in all patients in our cohort. Prolonged treatment was well tolerated by most patients. Over half of patients achieved a complete response with no residual microscopic disease. Careful long-term follow-up is needed to confirm long-term disease-free survival.
- neoplasia
- treatment medical
- treatment surgery
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Sonic hedgehog (SHH) inhibitors, vismodegib (Erivedge, Genentech, given orally at 150 mg daily) and sonidegib (Odomzo, Novartis, given orally at 200 mg daily) block activation of the SHH pathway. Patients with sporadic basal cell carcinoma (BCC) have been shown to harbour mutations that cause abnormal activation of this pathway.1 Vismodegib is FDA-approved for treatment of a locally advanced BCC that has recurred after surgery, for patients who are not candidates for surgery or radiation therapy and for metastatic disease.2
Locally advanced BCC of the periocular region presents special therapeutic challenges given the complex anatomical and functionally important nature of the orbital structures and aesthetically obvious location of tumour. Total surgical excision in many patients with locally advanced periocular BCC may result in orbital exenteration. Radiation is an optional therapy in unresectable tumours, but carries the risk of considerable ocular toxicity and lower efficacy compared with surgery.
The concept of neoadjuvant therapy practiced for large tumours aims to reduce tumour size and enable a less radical, organ-sparing, surgery. Experience in recent years have shown increasingly favourable clinical outcomes with SHH inhibitors for treatment of BCC both in the periocular region and elsewhere in the body.3 4 We herein present our observations in patients with locally advanced periocular BCC using neoadjuvant vismodegib followed by surgery with ocular preservation and local control as main objectives.
Materials and methods
All consecutive patients with a locally advanced periocular BCC that were under the care of the senior author (BE) between 2013 and 2017 and received vismodegib prior to surgery were included.
Institutional review board approval was obtained for this retrospective report. The work was carried out in compliance with the Health Insurance Portability and Accountability Act. All patients took oral vismodegib (150 mg/day) until one of the following outcomes was observed: gross total response on clinical examination and imaging, partial significant response to the point where the ophthalmic surgeon (BE) felt eye preservation was possible with surgery, maximum clinical benefit reached (patient stopped responding), disease progression or until patient was unable to tolerate treatment due to side effects. The clinical records, pathology data, and imaging studies for each patient were reviewed.
Each target lesion was staged according to the American Joint Committee on Cancer (AJCC) 8th edition cancer staging manual for eyelid carcinoma and based on baseline findings on clinical examination and imaging.5
Response to treatment
Clinical response to treatment was evaluated according to the Response Evaluation Criteria in Solid Tumours (RECIST) V.1.1.6 Response to treatment was assessed at 1-month intervals and was based on findings of clinical examination and/or imaging studies. Clinical improvement entailed a reduction in size of the skin lesion, resolution of ulceration and reduction in size of the periocular lesions seen on imaging.
Drug-related adverse events
Grade and type of all drug-related adverse effects were determined according to the Common Terminology Criteria for Adverse Events (CTCAE) V.4.03.7
Results
Eight patients, all men, with a median age at presentation of 69 years (range: 55–84 years), and a T4 periocular BCC (defined by the AJCC 8th edition criteria for eyelid carcinoma as any carcinoma invading adjacent ocular, orbital or facial structures), who were treated with neoadjuvant vismodegib prior to surgery, were included. Clinical and histological data for each patient are presented in table 1. Two patients (25%) had a primary BCC and six patients (75%) had a recurrent BCC after a mean of 4.8 (range 2–12) years from definitive surgical resection of a primary tumour at other institutions. Histopathological evaluation before therapy revealed exclusively nodular pattern in one patient and combined nodular and infiltrative patterns in the rest (table 1). Focal squamous differentiation was noted in five patients. Two patients had extratumoural perineural invasion.
Clinical and histologic characteristics (n=8)
The AJCC (8th edition) stage for all eight patients was T4N0M0 using the eyelid carcinoma staging criteria.5
Treatment indications and clinical outcomes
Indications for treatment were to avoid orbital exenteration in six patients, an unresectable tumour in one patient and to avoid an extensive surgery that was anticipated to result in a large facial defect necessitating a free-flap reconstruction and significant facial deformity and impairment of eye function, in one patient.
We documented a significant clinical response in all patients after the first month of treatment. Duration of treatment with vismodegib prior to surgery ranged from 4 to 36 months (median of 14 months). All patients were seen at monthly intervals by either the medical oncologist or the ophthalmic surgeon to evaluate treatment response and assess treatment related side effects.
At the time of surgery, four patients had achieved an excellent clinical response with no macroscopic residual tumour, and four patients had partial (but significant) response to vismodegib. Vismodegib therapy was electively stopped in six patients after observing the desired clinical response at a median of 5 (range 2–20) days prior to surgery. In the two other patients, vismodegib was stopped due to intolerable side effects 3 and 43 days prior to surgery, respectively.
Surgery and pathological findings
All patients underwent an eye-sparing surgery following neoadjuvant therapy with vismodegib. Surgery included excision of any tissue clinically suspected for residual tumour, with frozen section control of the margins (en face section and analysis of each margin) and biopsies as needed (figure 1). In all cases, some reconstructive surgery was needed given the degree of periocular soft tissue destruction and loss or eyelid malposition due to tumour infiltration at baseline (figure 2).
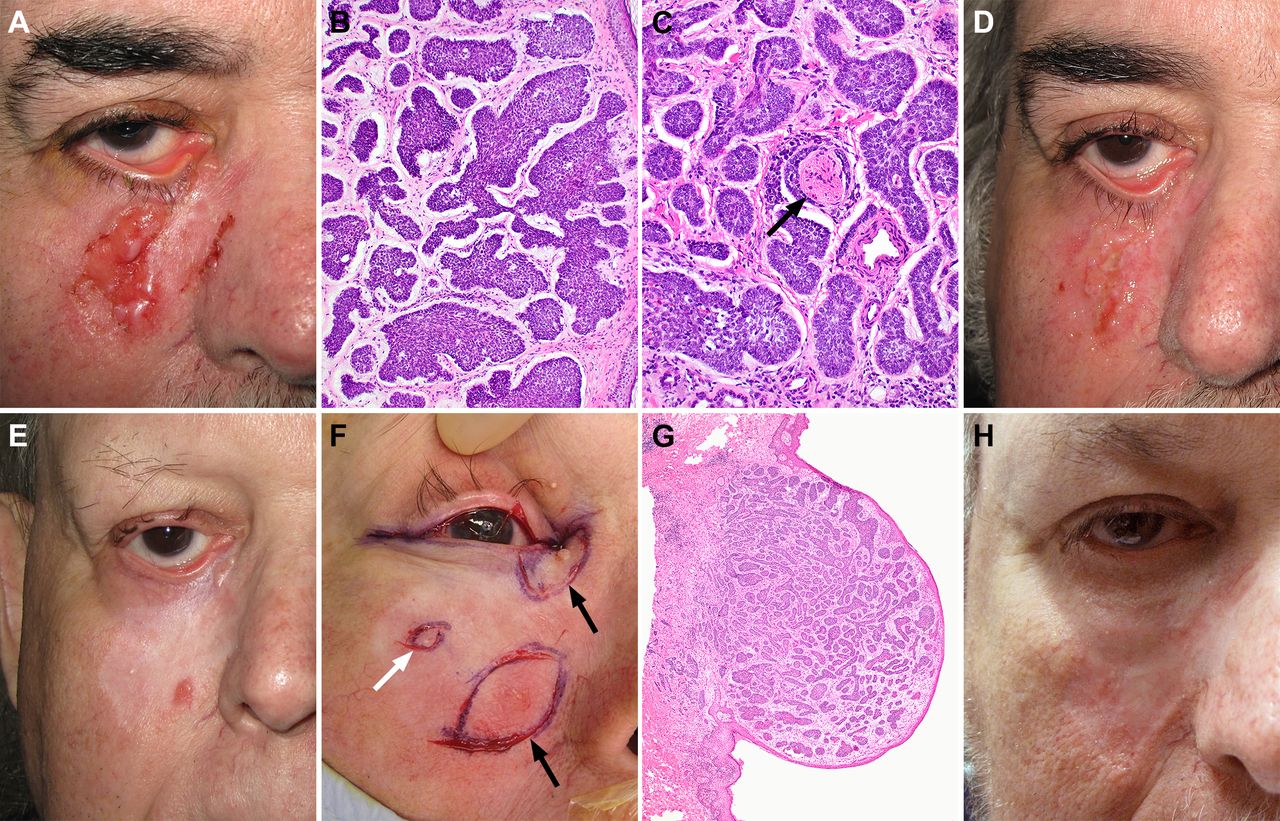
Locally advanced periocular BCC. (A) This is a 67-year-old man (patient no. 2 in the table) who presented with a T4aN0M0 BCC involving the right lower eyelid, medial canthus and cheek. Surgery was anticipated to result in a very large facial skin defect that will require a free flap and impair ocular function. (B) Histopathological evaluation revealed a large BCC with nodular and infiltrative patterns (H&E, magnification 100×), (C) with extratumoural perineural invasion of a small nerve fibre <0.1 mm (arrow, H&E, magnification 200×). (D) He was treated with neoadjuvant vismodegib, with significant response after the first month. (E) The treatment was continued for 10 months to achieve maximal stable clinical response. (F) He then underwent surgical excision of residual lesions that were clinically suspicious. Some (white arrow) were found to contain only dermal fibrosis with no residual tumour, and others (black arrows) were confirmed as BCC on histological evaluation (G, H&E, magnification 40×), with all margins negative for tumour. (H) Patient at 11 months of follow-up with a good functional and aesthetic result and no recurrence. BCC, basal cell carcinoma.

{kind=link}
{kind=link}
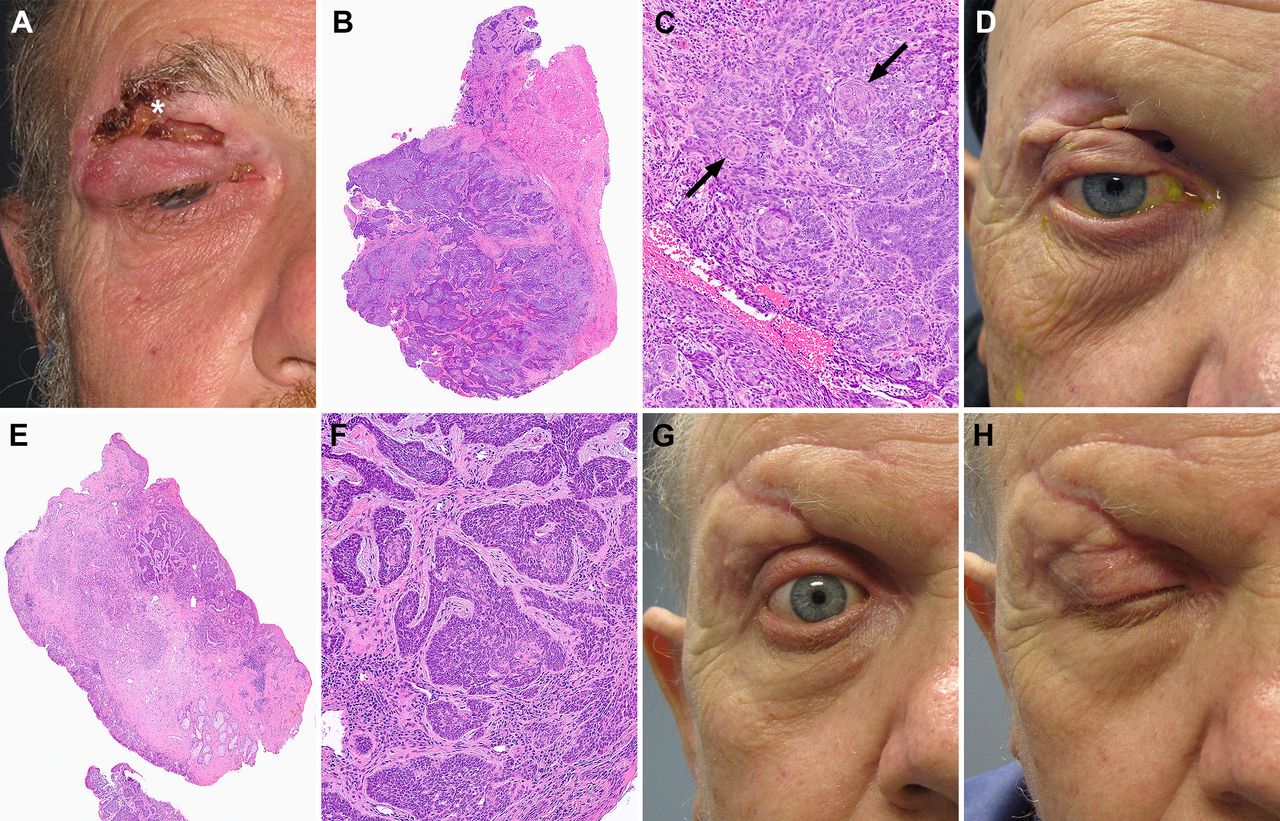
Locally advanced periocular BCC. (A) This is a 55-year-old man (patient no. 4 in the table) who presented with a T4aN0M0 right upper eyelid and brow BCC, invading the anterior orbit. Orbital exenteration was discussed but the patient denied this option. (B) Histopathological evaluation revealed a large BCC with nodular and infiltrative patterns (H&E, magnification 20×), (C) with focal squamous differentiation (arrows) (H&E, magnification 200×). (D) He was treated with neoadjuvant vismodegib over 18 months with an excellent clinical response. He then underwent and eye-sparing surgery with a wide local excision of the residual lesion and reconstruction. (E,F) Pathological evaluation found residual BCC, and all surgical margins were negative for tumour (H&E, magnification (E) 20×, (F) 200×). (G,H) Clinical photos from 6 months postoperatively with good functional ocular and eyelid results and no sign for recurrence. BCC, basal cell carcinoma.
Histopathological analysis of the surgical specimens revealed viable tumour in only three patients, while five patients were free of tumour and determined to have achieved a complete response. Eye preserving surgery and reconstruction was possible in all patients. Final margins were free of tumour in all patients. After surgery, all patients were followed every 3 months for surveillance. All patients were without evidence of recurrent or metastatic disease at last follow-up with a mean follow-up time of 18 months (range: 6–43) months.
All three patients with residual tumour had nodular and infiltrating patterns of growth before vismodegib therapy, which persisted in the residual tumours as well. Of the five patients with focal squamous differentiation, two patients had residual BCC, of which one retained only small foci of squamous differentiation.
Side effects
Vismodegib was tolerated well by most patients, and no serious (grade 3–5) adverse events were observed during the study period. Five patients had only mild (grade 1) side effects that included fatigue, alopecia, changes in taste, loss of appetite and weight and muscle cramps. Three patients had grade 2 side effects, and a dose reduction to five times/week instead of a daily dose alleviated some of the symptoms in two of them (patients no. 1 and 3). Eventually two patients had to stop treatment due to intolerable side effects after 5 and 18 months of treatments, respectively, having achieved clinically significant partial response. The residual BCC in these two patients was removed surgically and even in these two patients, an eye-preserving surgery was possible.
Discussion
Our observations in this report suggest that neoadjuvant use of vismodegib in patients with locally advanced BCC of the periocular region (T4 by AJCC criteria for eyelid carcinoma) is promising and merits further studies. This approach enabled us to achieve eye preservation in all patients and avoid orbital exenteration or major disfiguring facial surgery with compromise of ocular function.
We observed 100% (8/8) clinical response rate with over half (5/8) achieving complete response prior to surgery. Only three out of eight patients had some residual BCC that was resected during eye preserving surgery. Two patients had their treatment with vismodegib stopped due to intolerable side effects but even in these patients, significant clinical response had been achieved prior to eye-preserving surgery. Most importantly, vismodegib therapy provided ocular preservation for all seven patients who would have otherwise required orbital exenteration. Our response rates are similar to those reported in a recent review of vismodegib therapy for locally advanced BCC (in all anatomic sites) or metastatic BCC in 704 patients pooled from eight reports. The authors reported an overall response rate of 65% with 31% complete response rate.3 Careful follow-up surveillance is needed to confirm long-term response rates after surgery.
Eye-sparing surgery has been previously suggested in selected cases.8 Madge et al reported their experience with 20 patients with locally advanced medial canthal BCC with orbital invasion and focused on the desired surgical technique for achieving clear margins while sparing the eye.9 Two of their patients (10%) failed to achieve clear margins and were treated with adjuvant radiation therapy, and one patient had an orbital exenteration later. These large resections were also noted to result in restriction in 60% of patients and revision procedures in 60% of patients. A review of the literature by Sun et al suggests adjuvant RT or chemotherapy as an option for patients with positive margins after surgery. Both these reports discuss eye preserving surgical approaches combined with chemotherapy or radiation but do not discuss the option for neoadjuvant drug treatment which has the potential to result in less extensive surgery and greater possibility of preservation of the eye and ocular function.
It is important to note that the neoadjuvant use of vismodegib prior to surgery as in our patients is considered off-label use. The FDA-approved indications for vismodegib are for treatment of a locally advanced BCC that has recurred after surgery, for patients who are not candidates for surgery or radiation therapy and for metastatic disease. Most previous reports in the literature are isolated cases that have been reported in terms of overall response of periocular BCC to vismodegib but not neoadjuvant use prior to surgery. Gill et al reported their experience with seven patients with recurrent periocular BCC, treated for only 11 (range 4–16) weeks with vismodegib.10 They observed complete response in two patients, partial response in four patients and progressive disease in one patient. The AJCC T category for patients’ BCC was not reported but judging by some of the photographs, some patients had smaller than locally advanced T4 tumours. In this report, there was no mention of surgery and the follow-up time was relatively short. Ally et al reported 11 patients with ‘large BCCs’ although this was defined as tumours greater than 5 mm and only 2 were in the periocular area and reported about 27% reduction in size of tumours compared with baseline.11 The authors stated that vismodegib was not effective in patients who received it for less than 3 months. Kahana et al reported in a letter to the editor of a single patient with an orbital BCC 10 years after initial excision who was treated with oral vismodegib for 4 months with a partial response and about 70% reduction in tumour size.12 The patient stopped treatment due to intolerable muscle spasms and surgery was carried out with globe-preservation. Pathology found mostly fibrotic tissue with small clusters of residual cancer foci. Wong et al recently reported a review of 15 patients with locally advanced periocular or orbital BCC, with treatment duration of 13 months and a mean follow-up of 36 months.13 They found that 67% of patients had complete response, 20% had partial response and 13% had progressive disease. Of note, only three patients in this report underwent surgery: two patients with progressive disease underwent orbital exenteration and one patient had recurrence 21 months after observation of a complete response and was treated with orbital exenteration. A major advantage of our current study design is that we systematically assessed all residual periocular and orbital lesions with surgical resection in all patients, after a median of 14 months of vismodegib treatment. This significantly improved our ability to assess true microscopic response rate.
The median duration of neoadjuvant treatment with vismodegib in our cohort was 14 months, although some patients had complete response seen as early as 3 months after treatment on vismodegib. The duration of treatment with vismodegib can vary depending on the trajectory of tumour response, which is influenced by the size and extent of the lesion at presentation and may vary depending on the exact histological variety of BCC and the heterogeneity of tumour biology.
In the current study, seven patients had nodular and infiltrative patterns of growth, of which five had focal squamous differentiation and two had perineural invasion. The residual tumours also had nodular and infiltrative patterns of growth, one of which had focal squamous differentiation. Extensive squamous areas were not identified in any of the residual BCCs. Long-term results of the ERIVANCE BCC study have shown vismodegib treatment to be effective for all histological subtypes of BCC including infiltrative.14 Basosquamous carcinoma refers to a BCC with squamous differentiation, which tend to run a more aggressive course, has a higher rate of recurrences and metastases.15 A recent review on basosquamous carcinoma did not find specific reports on the efficacy of vismodegib for basosquamous carcinoma.15 In the current study, three out of five patients with squamous differentiation had a complete response to neoadjuvant vismodegib therapy, while two had partial response, of which one (case #6) had focal squamous differentiation in the residual tumour as well. All five patients who had squamous differentiation before therapy are alive without evidence of disease at last follow-up after surgery.
Several reports suggest that Vismodegib therapy may promote squamous differentiation in BCCs and/or promote development of new squamous cell carcinomas.16–19 In contrast, a recent retrospective cohort study has demonstrated that Vismodegib therapy for BCC may not increase the risk of developing subsequent squamous cell carcinomas.20 To our knowledge, development of new squamous carcinomas while on vismodegib treatment have been reported only in the setting of resistance to Vismodegib therapy. In our current report, all patients responded to Vismodegib therapy to some extent (five complete and three with significant partial responses). Tumours of none of our patients progressed or recurred during or following therapy to date. Thus, it appears that most BCCs, even those with squamous differentiation may respond to vismodegib therapy, while resistance may develop due to (1) inherent SMO or SUFU mutations or MYCN amplifications (primary) or (2) acquisition of SMO mutations and/or activation of Ras/MAP kinase pathway after exposure to vismodegib (secondary).21 22 The lack of development of vismodegib resistance in our patients could explain why BCCs with squamous differentiation have responded to therapy and why there was only focal squamous differentiation in the residual tumour.
Most of the patients in the current report were able to tolerate vismodegib well over several months, and most symptoms were low grade and medically manageable. Similar to our observations, the ERIVANCE study reported most (93%) of side effects to be low to intermediate in severity (Grade 1–2).23 A recent review of nine studies confirmed that the majority of patients experienced only mild (grade 1/2) side effects with the most common being muscle spasms (66.4%), alopecia (61.1%), dysgeusia (57.3%), weight loss (33.4%), amenorrhea (32.9%), fatigue (20.1%). The same report suggests a weighted average of 28.2% (95% CI, 27.3% to 29.1%) of patients discontinued vismodegib treatment due to adverse effects.3 Based on these findings, we recommend that the possibility of several months of neoadjuvant treatment with vismodegib with a relatively well-tolerated safety profile be discussed with the patient. Close collaboration with an oncologist is critical in managing side effects and allowing to extend the treatment duration in order to achieve maximal reduction in tumour burden prior to surgery.
The current report has some limitations. The retrospective nature of the report may have introduced some unintended biases in our observations. For some of the patients in the cohort, the follow-up time after surgery is short. Surgery did not always include the entire area of the original tumour for lack of macroscopically residual tumour (figure 1), and given that BCC is a slow-growing tumour, a longer follow-up time of up to 5 years may be needed to fully assess the risk for local recurrence. We believe the risk of local recurrence should be kept in mind, but given that the risk of distant metastasis from BCC is exceedingly small, this neoadjuvant approach to decrease surgical morbidity and preserve the eye and its function makes sense. All of the patients in our cohort are still under active surveillance and will continue for at least 5 years after discontinuation of vismodegib. Future prospective trials with eye preservation as primary endpoint should be designed and are currently planned.
In conclusion, our report suggests that the neoadjuvant use of vismodegib or other available SHH inhibitors is a sensible option to try in patients with locally advanced (T4 by 8th edition AJCC criteria) BCC of the periocular region and this approach can prevent the need for orbital exenteration or other major disfiguring surgery in the periocular region. We believe that surgical removal of gross residual tumour as well as targeted map biopsies are appropriate after complete or partial response to vismodegib in this setting (figure 1). In most patients with locally advanced periocular BCC, some reconstructive surgery is also needed given the degree of soft tissue destruction secondary to tumour. Physicians need to consider the extent of posterior orbital involvement and the patient’s ability to maintain a long-term follow-up when recommending this treatment. The risks of a possible local recurrence and its implications need to be discussed with patients. We recommend close follow-up surveillance for up to 5 years after neoadjuvant vismodegib and surgery given the risk of late recurrence.
References
Footnotes
Contributors All authors contributed to the planning, conduct and reporting of the work described in the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study obtained ethics approval by the University of Texas MD Anderson Cancer Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note At the time of writing this paper, vismodegib is not recommended by the National Institute for Health and Care Excellence (NICE) within its marketing authorisation for treating symptomatic metastatic basal cell carcinoma, or locally advanced basal cell carcinoma that is inappropriate for surgery or radiotherapy, in adults. However, the drug is available for purchase to patients in the UK outside the NHS authority. For more information, see: https://www.nice.org.uk/guidance/ta489/chapter/1-Recommendations.
Linked Articles
- At a glance