Article Text

Abstract
Aim To investigate the change in posterior corneal elevations (PCEs) of eyes with extremely high myopia 2 years after small incision lenticule extraction (SMILE).
Methods We evaluated 39 eyes of 39 patients with spherical equivalent higher than −10.00 dioptres (D). Using a Scheimpflug camera (Pentacam), we measured change in PCEs at 1 day, 3 months, 6 months and 2 years after SMILE. Another 34 eyes of 34 patients who underwent femtosecond laser-assisted in situ keratomileusis (FS-LASIK) were examined before, at 1 day and long-term after surgery as the control group. For each eye, elevations at central, thinnest, maximal points and 24 other predetermined points were measured.
Results No significant forward displacements of PCEs were observed in both surgeries. The maximal but not significant forward displacement occurred around 3–6 months following SMILE, and all returned to original levels 6 months postoperatively except superior area. The peripheral area tended to displace backward, while the central area tended forwardly. In both procedures, elevations along horizontal meridians, inferior and temporal hemispheres were significantly higher than those along vertical meridians, superior and nasal hemispheres, respectively (p<0.05). Elevation on the 4 mm, 6 mm diameters at 1 day and on the 6 mm diameter and temporal hemisphere at long-term follow-up postoperatively were significantly higher in FS-LASIK than SMILE (p<0.05). Change in elevations on the 6 mm diameter circle correlated with residual bed thickness (p=0.047).
Conclusions SMILE is a safe way to correct for myopia higher than −10 D, with PCEs remaining stable 2 years after surgery.
- optics and refraction
- treatment surgery
- treatment lasers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Small incision lenticule extraction (SMILE), first introduced by Sekundo and Shah in 2011, is a flap-free and minimally invasive variant of femtosecond lenticule extraction.1 Its safety, efficacy, predictability and stability have been widely confirmed,2 3 leading to increased researches on its effects on corneal morphology and biomechanical properties.
Due to its flap-free procedure, more of the anterior stroma remains intact after SMILE. This theoretically contributes to better preservation of corneal biomechanics.4 Keratoconus is one of the most serious postoperative complications.5 Posterior corneal elevation is a highly specific and effective indicator for early stage corneal ectasia.6 7 Many studies were done on the forward displacement of the posterior surface after undergoing laser-assisted in situ keratomileusis (LASIK).8 9 However, studies on elevations after SMILE have been insufficient. Previous studies show a higher risk of postoperative ectasia in patients with high myopia.8 Considering the thinner cornea and weaker corneal strength caused by the increased tissue removal in patients with high myopia, the stability of their posterior corneal surface needs better assessment.
Methods
Patients
This prospective non-randomised cohort study evaluates the long-term stability of posterior corneal elevation in eyes with extremely high myopia after SMILE and femtosecond laser-assisted in situ keratomileusis (FS-LASIK). Patients were recruited in a continuous cohort between June 2015 and February 2016 at Eye and ENT Hospital of Fudan University (Shanghai, China).
Patient inclusion criteria: spherical equivalent (SE) ≥ −10 dioptres (D), astigmatism <5 D, corrected distance visual acuity (CDVA) ≥20/32, sufficient corneal thickness (estimated postoperative corneal thickness >400 μm and residual bed thickness [RBT] >250 μm), stable refractive error in the preceding 2 years and no use of contact lenses within preceding 2 weeks.
Patient exclusion criteria: systemic or other ocular diseases, history of ocular surgeries or trauma, suspicion of keratectasia or dry eye.
All individuals were healthy, routinely screened and met the criteria for two surgeries. Thirty-nine participants (12 male and 27 female) who underwent SMILE were examined before, at 1 day, 1 month, 3 months, 6 months and 2 years after surgery. Another 34 participants (12 males and 22 females) who underwent FS-LASIK were examined before, at 1 day and at least 1 year (18.2±5.9 months, range from 12 to 33 months) after surgery as the control group. One random eye from each participant was analysed. Detailed patient information is shown in table 1.
Eye measurements before SMILE and FS-LASIK
Surgical procedures
SMILE was performed using VisuMax femtosecond laser system (Carl Zeiss Meditec, Jena, Germany) with a repetition rate of 500 kHz and a pulse energy of 130 nJ. Lenticule diameter was set to 6 mm. The intended corneal cap thickness was set to 100–120 μm with a diameter of 7.5 mm. The procedure is described previously.10
In the FS-LASIK procedures, the same femtosecond laser system was used for flap creation with a pulse energy of 185 nJ, followed by a MEL 80 excimer laser (Carl Zeiss Meditec, Oberkochen, Germany) for stromal ablation with a repetition rate of 250 Hz and a pulse energy of 1.00±0.15 mJ. The intended flap thickness was set to 100 μm with a diameter of 8 mm. The hinges were located at a superior 12 o’clock with a length of 4.0 mm.
All surgeries were performed by an experienced surgeon (XTZ). Prior to surgery, 0.5% topical levofloxacin (Cravit; Santen, Osaka, Japan) was applied four to six times daily for 3 days. A bandage soft contact lens was applied for 1 day after FS-LASIK. After both procedures, 0.5% topical levofloxacin, 0.1% fluorometholone solution and non-preserved artificial tears (carboxymethylcellulose sodium eye drops; Allergan, Irvine, California, USA) were applied.
Clinical examinations
Posterior corneal elevation measurements were obtained using the Pentacam HR (Oculus GmbH, Wetzlar, Germany).11 For each measurement, three consecutive readings were taken just after blinking twice to minimise the effect of tear films. Image quality labelled with ‘OK’ under the inspection window was accepted. All images covered the central 10.0 mm of corneal surface, without extrapolation in the central 9.0 mm zone. All measurements were taken between 10:00 and 17:00 by a trained operator (XYZ).
Routine examinations like uncorrected distance visual acuity (UDVA), CDVA and SE were also performed.
Data collection
For each eye, the best-fit sphere (BFS) in the central 8.0 mm zone of the preoperative cornea was used as the reference surface. The change in elevation is equal to postoperative elevation minus preoperative elevation, where a positive difference indicates forward displacement of the posterior surface.
Elevations were measured at the thinnest (posterior elevation at the thinnest point (PTE)) and maximal (posteriormaximal elevation (PME)) points in relation to preoperative BFS, in addition to the central (posteriorcentral elevation (PCE)) and at 24 other predetermined points on three concentric circles (1, 2 and 3 mm from the centre, along the 0°, 45°, 90°, 135°, 180°, 225°, 270° and 315° semimeridians). PME is the highest elevation in the central area within 6 mm (taken directly from mouse-over read-out values). Posterior average elevation was calculated from the centre and 24 predetermined points. The average values of each concentric circle are denoted by PCE0 (one point, centre), PCE2 (eight points, 1 mm out from the centre), PCE4 (eight points, 2 mm out) and PCE6 (eight points, 3 mm out). These points are split symmetrically into nasal (posterior corneal elevation in nasal hemisphere (NPCE)) and temporal (posterior corneal elevation in temporal hemisphere (TPCE)) hemispheres by the 90°−270° meridian, and superior (posterior corneal elevation in superior hemisphere (SPCE)) and inferior (posterior corneal elevation in inferior hemisphere (IPCE)) hemispheres by the 0°−180° meridian. 0° of the right eye is defined along the horizontal semimeridian pointing towards the right, with clockwise positive angles. Vice versa for the left eye, with counterclockwise positive angles.
Statistical analysis
Statistical analysis was performed using SAS system software V.9.4. The one-sample Kolmogorov-Smirnov test was used to test for normality. Continuous variables with normal distributions were denoted as average ± SD. Mixed linear models for repeated measurements were employed to analyse the change in elevations over time and to compare the changes between different surgeries. Average change in elevations in different hemispheres and meridians were compared using paired T tests. Pearson correlation analysis was used to evaluate the linear relationships between elevation changes and several variables, including preoperative refraction, preoperative intraocular pressure (IOP), preoperative thinnest corneal thickness, ablation depth (AD) and RBT. P<0.05 was considered statistically significant.
Results
Refractive outcomes
Refractive outcomes are summarised in figure 1. The safety index and effectiveness index at the 2-year follow-up was 1.29 and 0.96, respectively. UDVA was ≥20/32, ≥20/25 and ≥20/20 in 34 (100%), 29 (85.29%) and 21 (61.76%) eyes, respectively. The SE of 14 (41.18%) and 26 (76.47%) eyes were within the range of ±0.50 and ±1.00 D, respectively. Thirty-three (97.06%) eyes remained stable or gained Snellen lines. Twenty-eight (82.35%) gained one to three lines, while only one (2.94%) lost one line. None lost two or more.

Refractive outcomes during the follow-up period after small-incision lenticule extraction (SMILE). CDVA,corrected distance visual acuity;D, dioptres; UDVA, uncorrected distance visual acuity.
Posterior corneal elevation
See table 2 for postoperative elevation differences. With the exception of △TPCE (p=0.026) in SMILE group and △PTE (p=0.042) in FS-LASIK group, no significant changes over time were observed. △PME at 1 day, △PCE, △PME, △NPCE, △SPCE, △PCE0, △PCE2 at 3 months and △SPCE at 6 months after SMILE displayed non-significant forward displacements (p>0.05). SPCE reverted to original levels within 2 years, while the rest reverted within 6 months. In FS-LASIK group, all elevations displayed non-significant forward displacements at 1 day postoperatively except △PTE and △SPCE, and most reverted to original levels at long-term follow-up except △PCE6 and △IPCE. △TPCE at 6 months (p=0.002), △PTE at 2 years (p=0.015) after SMILE and △PTE at long-term follow-up (p=0.019) after FS-LASIK displayed significant backward displacements. See figure 2 for the variation of elevations in SMILE group on different points (A), hemispheres (B) and radii (C). Most parameters reached peak anterior protrusion 3 months after surgery. Peak anterior protrusion occurred later at larger radii. No significant differences were detected between surgeries except TPCE (p=0.003), PCE4 (p=0.045) and PCE6 (p=0.013) (figure 2D,E,F). TPCE at long-term follow-up was higher in FS-LASIK than SMILE (p=0.015). Meanwhile, PCE4 (p=0.032) and PCE6 (p=0.019) at 1 day, and PCE6 (p=0.036) at long-term postoperatively were higher in FS-LASIK than SMILE.
Changes in posterior corneal elevations after SMILE and FS-LASIK

Change in posterior corneal elevations after small-incision lenticule extraction (SMILE) and comparison with femtosecond laser-assisted in situ keratomileusis (FS-LASIK). (A) Posterior central (PCE), maximal (PME), posterior average elevation (PAE) and at the thinnest point (PTE). (B) Changes in nasal (NPCE), temporal (TPCE), inferior (IPCE) and superior (SPCE) hemispheres. (C) Changes at centre (PCE0), 2 mm (PCE2), 4 mm (PCE4) and 6 mm (PCE6) diameters. With the exception of △TPCE (p=0.026), no significant changes over time were observed after SMILE. Significant differences between surgeries in TPCE (D), PCE4 (E) and PCE6 (F). Individual points and error bars represent the estimated mean and SD. *P<0.05 between SMILE and FS-LASIK.
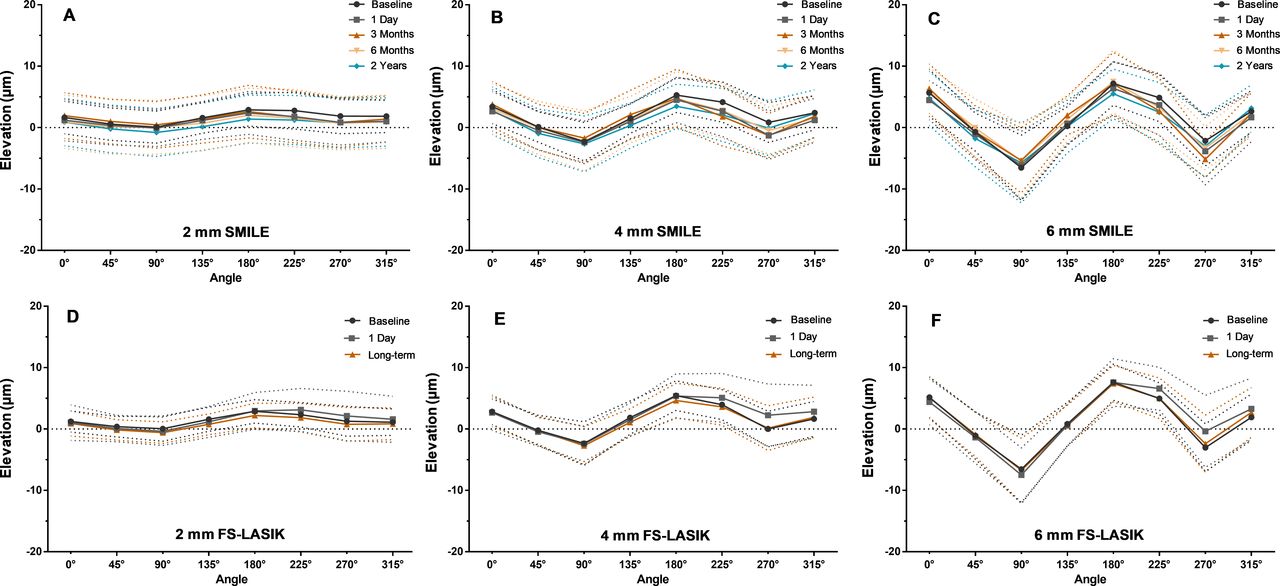
Figure 3 shows the variation of elevations at different radii and different angles. The trends in elevation change remain roughly consistent position-wise across time. Elevation fluctuations increased from the centre (difference at 2 mm diameter: SMILE, 1.41 μm; FS-LASIK, 2.82 μm) to the periphery (difference at 6 mm diameter: SMILE, 12.26 μm; FS-LASIK, 14.18 μm). In both procedures, elevations rose above the BFS along the 0°−180° meridian and dropped below the BFS along the 90°−270° meridian except at 2 mm diameter (SMILE: 2 mm, horizontal, 2.01±2.73 μm, vertical, 0.72±2.63 μm, p<0.001; 4 mm, horizontal, 3.99±2.56 μm, vertical, −1.12±2.41 μm, p<0.001; 6 mm, horizontal, 5.96±3.05 μm, vertical, −1.12±2.41 μm, p<0.001. FS-LASIK: 2 mm, horizontal, 1.98±2.08 μm, vertical, 0.61±2.03 μm, p<0.001; 4 mm, horizontal, 4.05±1.84 μm, vertical, −0.93±1.78 μm, p<0.001; 6 mm, horizontal, 6.30±2.43 μm, vertical, −4.55±2.30 μm, p<0.001), forming two distinct peaks and valleys at all diameters. Furthermore, average elevations were significantly higher on the inferior hemisphere than on the superior hemisphere at all diameters (SMILE: 2 mm, inferior, 1.28±3.19 μm, superior, 0.12±2.72 μm, p=0.005; 4 mm, inferior, −0.15±3.35 μm, superior, −2.03±3.21 μm, p=0.011; 6 mm, inferior, −3.08±3.70 μm, superior, −5.72±3.45 μm, p=0.008. FS-LASIK: 2 mm, inferior, 1.68±2.45 μm, superior, 0.50±2.22 μm, p=0.008; 4 mm, inferior, 2.21±2.79 μm, superior, −0.30±2.58 μm, p=0.003; 6 mm, inferior, 1.80±3.15 μm, superior, −2.32±3.38 μm, p<0.001). Elevations were also significantly higher on the temporal hemisphere than on the nasal hemisphere at all diameters apart from 6 mm in SMILE group (SMILE: 2 mm, temporal, 2.40±2.95 μm, nasal, 1.59±2.89 μm, p=0.011; 4 mm, temporal, 4.52±2.97 μm, nasal, 3.29±2.87 μm, p=0.016; 6 mm, temporal, 6.39±3.69 μm, nasal, 5.38±3.45 μm, p=0.086. FS-LASIK: 2 mm, temporal, 2.13±1.92 μm, nasal, 0.96±2.34 μm, p<0.001; 4 mm, temporal, 3.50±1.70 μm, nasal, 1.73±2.32 μm, p<0.001; 6 mm, temporal, 4.38±1.63 μm, nasal, 2.34±2.32 μm, p<0.001).
{kind=link}
{kind=link}
{kind=link}
Posterior corneal elevations changes at various diameters from the perspective of the meridian after small-incision lenticule extraction (SMILE) and comparison with femtosecond laser-assisted in situ keratomileusis (FS-LASIK). (A–C) Variations at 2, 4 and 6 mm diameter in SMILE group. (D–F) Variations at 2, 4 and 6 mm diameter in FS-LASIK group. Individual points and dotted lines represent the estimated mean and SD.
Correlation analysis
In SMILE group, △PCE6 negatively correlates with RBT (r=−0.450, p=0.047) at 3 months. Both △TPCE and △PME positively correlate with AD at 6 months (r=0.534, p=0.033 and r=0.489, p=0.043, respectively). △TPCE, △PCE4 and △PCE6 correlate positively with preoperative IOP at 2 years (r=0.349, p=0.043; r=0.352, p=0.048 and r=0.380, p=0.032, respectively).
Discussion
Orbscan II and Pentacam HR are the most commonly used instruments for measuring posterior corneal elevation. However, the accuracy of Orbscan II has been disputed,12 13 being susceptible to overestimation of corneal elevations.14 Pentacam is accurate at measuring posterior elevations, which can be further improved by repeated measurements.15 Studies have confirmed that Pentacam can effectively distinguish the posterior elevations of keratoconus, subclinical keratoconus and normal corneas with high sensitivity and specificity,6 which serves as one of the most effective parameters for corneal ectasia diagnosis.16
The average PCE and PTE at 2 years postoperatively were 0.15 and 1.38 μm, respectively, close to the results (median of 0.0 and 3 μm) reported by Ying et al, who conducted a large cross-sectional study of 1500 Chinese corneal refractive surgery patients.17 Furthermore, all elevation changes were within Pentacam's ±5 µm measurement error range (95% limits of agreement: 4.27 to −5.29 μm at the 5 mm zone).15 This indicates that the posterior corneal surface remains stable 2 years after SMILE for extremely high myopia.
Only a few studies researched corneal elevations after SMILE, and all reported elevation changes within measurement error range of ±5 µm.11 18–20 No significant forward displacements were observed postoperatively except during early stages of recovery.18 Zhao et al 11 and Wang et al 19 reported stable posterior corneal surfaces in eyes with moderate to high myopia the first year following SMILE, which is supplemented by our research group’s 3 years study (mean change at 3 years: PCE, −2.39±2.85 μm, p<0.05; PME, 0.50±3.33 μm, p=1.000; PTE, −2.33±2.90 µm, p<0.05).20 This study provides long-term evidence for myopia higher than −10 D with slightly different results (mean change at 2 years: PCE, −1.18±3.06 μm, p>0.05; PME, −0.47±3.07 μm, p>0.05; PTE, −1.94±3.21 µm, p<0.05). Grewal et al 21 found forward displacements of 5.13±4.16, 5.78±4.42 and 6.68±4.72 µm 18 months after LASIK with three different methods of flap creation, respectively. These displacements seem all higher than that of SMILE and beyond Pentacam's measurement error range. Moreover, posterior elevation following FS-LASIK is significantly higher than that of SMILE one year postoperatively for high myopia.19 Our results agree with the previous study and provide complementary evidence for extremely high myopia. It is reasonable to presume that posterior surface was more stable after SMILE compared with LASIK.
Interestingly, there were slight but significant backward changes of NPCE in SMILE and PTE in FS-LASIK group. These backward shifts were previously observed after various refractive surgeries including photorefractive keratectomy (PRK),22 LASIK23 and SMILE,20 but the reason is still unclear. One possible explanation may be the hyperopic shift caused by flattening of the central cornea and thickening of peripheral stroma postoperatively, as demonstrated following PTK.20 Considering those backward shifts are still within measurement error, we need further investigation to explore the practical implications.
Some postoperative corneal biomechanical properties may partly explain the advantage of the posterior surface stability after SMILE. Corneal strength decreases non-linearly with increasing depth, with the anterior 40% of the surface bearing most of its strength, culminating on the Bowman's membrane.24 25 Several mathematical models and clinical studies confirmed that SMILE is better at preserving the corneal surface and biomechanical stability compared with LASIK, and the difference is even more pronounced for thinner corneas in high-myopia cases.4 26–28
In this study, the vast majority of elevations returned to original levels 6 months after SMILE. We found a slight overall backward displacement the first day postoperatively, followed by continued backward trend in the peripheral area, and a reversed forward trend in the central area after 3–6 months. This is in alignment with previous study, which revealed similar variability in elevations after LASIK, with the 2 mm diameter circle being the boundary between forward and backward displacements.29 Ganesh et al found an increase of negative keratometric power and prolate asphericity following ReFlex SMILE, especially in the central area, with higher impact as diopters increased.30 Conversely, Yu and associates18 found a backward trend in the central area and a forward trend in the peripheral area after SMILE. This may be due to the lower severity of myopia in their study (preop SE: −5.58±1.29 D). Higher myopia calls for thicker extractive lenticule and deeper ablation, leaving more interspace behind. Together with the remaining tensile strength of the uncut peripheral corneal cap, this may cause the posterior central elevation to compensate more than the peripheral elevation via a higher forward displacement.
The elevation was significantly higher on the horizontal meridian, inferior and temporal hemisphere than the vertical meridian, superior and nasal hemisphere, except for PCE6 in SMILE. The elevation differences between the orthogonal meridians and corresponding hemispheres grew larger as distances from the centre increased. The above results agree with previous reports.29 The difference between horizontal and vertical meridians maybe closely associated with the high incidence of with-the-rule astigmatism among young people.31
△PCE was found to negatively correlate with RBT, and positively with AD and preoperative IOP, corresponding to previous study.8 Curiously, our research group reported opposite results in a previous study: △PCE positively correlated with RBT and negatively with AD at 12 months postoperatively.11 In this study, the negative correlation between RBT and △PCE was found in the peripheral cornea, while the previous study focused on the central 4 mm area. The opposite displacements of the central (forward) and peripheral (backward) cornea in our study are likely the explanation. Notably, Reinstein et al 28 found that deeper lenticule tissue removal and lower RBT leads to a 0.08%/μm increase in corneal tensile strength, challenging earlier understandings of SMILE. Moreover, other studies have found that SMILE with deeper ADs have counterintuitively less impact on corneal biomechanics.32 Thus, more evidence is needed to disentangle the effects of AD and RBT on corneal biomechanics.
One limitation of our study is that we currently lack standard guidelines for measuring posterior corneal elevation. Given the complexity and asphericity of the cornea, a toric or aspheric reference surface may better reflect its real shape and biomechanical behaviour, compared with a spherical shape. The large-sample cross-sectional analysis found a correlation between BFS-based posterior corneal elevations and astigmatism,17 in this regard, best fit toric ellipsoid (BFTE) is less affected by astigmatism and superior to BFS at differentiating between normal cornea, keratoconus and forme fruste keratoconus.33 34 We chose BFS based on the habit of clinical practice, but possibly BFTE could be a better choice for patients with high astigmatism in this study (up to −4.50 D).
In conclusion, this study confirms the long-term stability of posterior corneal elevation in eyes with myopia higher than −10.00 D following SMILE and shows advantage of stability over FS-LASIK. Narrowing the scope of this study to extreme myopia is a limitation which can be mitigated with additional investigation of patients with more diverse degrees of myopia and astigmatism.
References
Footnotes
XZ and JS contributed equally.
Contributors XYZ, JS and XTZ: design of the study. XYZ, JS and BQ: conduct of the study. XYZ, JS, BQ and YZ: data collection. XYZ, JS and XTZ: analysis and interpretation of data. XYZ, YZ and XTZ: edits and revisions. XTZ: final approval of article.
Funding This study was supported by the National Natural Science Foundation of China (Grant No. 81770955, No.81570879) and the Project of Shanghai Science and Technology (Grant No. 17140902900, No. 17411950200).
Competing interests None declared.
Patient consent for publication Not Required
Ethics approval This study was approved by the Ethical Committee of the Fudan University EENT Hospital Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Linked Articles
- At a glance