Article Text

Abstract
Aims To investigate morphological changes in type VI collagen in the human trabecular meshwork associated with the rho kinase inhibitor ripasudil.
Methods This cross-sectional study evaluated the effects of ripasudil eye drop administration (RA) or no ripasudil eye drop administration (NRA) in patients with primary open-angle glaucoma (POAG; age range 60–80 years) who underwent conventional outflow reconstruction between December 2015 and September 2016 at Tokai University Hachioji Hospital. The juxtacanalicular tissue was removed and imaged using transmission electron microscopy. Type VI collagen comprises cross-banded aggregates with transverse bands 30 nm apart repeating every 105 nm. The transverse bands are called the outer rod-like region (ORR) and the intervals are called the inner rod-like region (IRR). The waveform intensity in the type VI collagen was analysed in electron micrographs using Fourier transformation to detect the IRR and ORR borders.
Results Ten eyes of 10 patients were included (n=5/group). The baseline characteristics did not differ significantly between groups. ORR width was significantly smaller in the RA group (37.85±3.43 nm) than in the NRA group (50.62±5.23 nm, p<0.05), whereas IRR width was significantly greater in the RA group (70.68±10.84 nm) than in the NRA group (58.19±5.34 nm, p<0.05). Morphological changes in the type VI collagen total width tended to correlate with the duration of ripasudil administration (r=0.9, p=0.08).
Conclusions Ripasudil administration in patients with POAG induced morphological changes in type VI collagen. Patients with POAG administered RA had a significantly smaller ORR width and a significantly greater IRR width than patients with POAG not administered RA.
- glaucoma
- pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In human eyes, the major outflow pathways of the aqueous humour are the trabecular meshwork (TM), Schlemm’s canal, collector channels and aqueous veins. Several experimental studies suggest that aqueous outflow resistance is generated in the juxtacanalicular tissue (JCT) region of the TM in human eyes.1–4 Abnormal accumulation of extracellular matrix (ECM) material in the JCT region in glaucoma is considered to increase outflow resistance.5–13 In primary open-angle glaucoma (POAG), the elastic fibres in the ECM are surrounded by increased amounts of type VI collagen and various other components of the ECM.14
Type VI collagen is a primary component of the ECM of many connective tissues.15–17 Type VI collagen monomers comprise a central 105 nm long triple-helical segment with an amino-(N-)terminal globular domain at one end and a carbon-(C-)terminal globular domain at the other end.18 19 Dimers are formed by two coiled type VI collagen molecules with a 30 nm axial shift. The basic structural unit of type VI collagen microfibrils is a tetramer formed by two laterally associated dimers with no axial shift. The N-terminal and C- terminal globular domains at each end of the outer rod-like regions (ORR) of two adjacent tetramers form non-covalent bonds, resulting in end-to-end, cross-banded and pseudofibrillar aggregates. The aggregates comprise transverse double bands approximately 30 nm apart that repeat axially every 105 nm. In the TM in human eyes, aggregates mainly present as single transverse bands.20
Rho-associated protein kinase (ROCK) inhibitors are a recently developed group of antiglaucoma medications that reduce intraocular pressure (IOP) in animal and human eyes. ROCK inhibitors increase aqueous humour outflow by loosening TM and JCT cells and thus decreasing the resistance in conventional outflow routes. These changes, based on the observations of Schlemm’s canal endothelial cells, alter the production and contraction of the ECM.21–24 ROCK inhibitors also affect a number of cellular reactions in corneal endothelial cells, such as differentiation, proliferation, cell adhesion cytoskeleton reorganisation and cell–matrix interactions.25–31
The molecular mechanisms underlying the effects of ROCK inhibitors on JCT cells in patients with POAG are not clear. Ripasudil hydrochloride hydrate (Glanatec ophthalmic solution 0.4%; hereafter referred to as ripasudil), a ROCK inhibitor (K-115) developed by Kowa, was approved in Japan for the treatment of glaucoma and ocular hypertension.32 In the present study, we investigated the morphological changes in type IV collagen associated with ripasudil in patients with POAG.
Methods
Subjects
In this cross-sectional study, we compared the morphological changes in type VI collagen between patients with POAG treated with or without ripasudil eye drops. Informed consent was obtained from all patients for the use of tissue obtained during surgery, including their descriptions in medical congresses and journals. Patients with POAG administered ripasudil eye drops (RA) for more than 6 months or not administered ripasudil eye drops (NRA) who underwent conventional outflow reconstruction to reduce IOP between December 2015 and September 2016 at Tokai University Hachioji Hospital were evaluated. Exclusion criteria included patients outside the age limit (range: 60–80 years); patients with other glaucoma types, diabetes, uveitis or history of retinal photocoagulation; and those who had undergone a previous intraocular procedure, such as cataract surgery, glaucoma surgery or vitreoretinal surgery. Patients who used ripasudil drops for less than 6 months were also excluded. Patient information regarding ripasudil treatment was masked by an observer (NN) using an index number. The masked information was opened after completing all of the analyses.
Surgical procedures
All patients underwent conventional outflow reconstruction combined with phacoemulsification. A 4.0 mm fornix-based conjunctival peritomy was performed, followed by the creation of a partial-thickness superficial scleral flap (3.0×3.0 mm U-shape flap) that extended into the clear cornea. Phacoemulsification and intraocular lens implantation were performed, and a deep scleral flap was created 0.5 mm inside the border of the superficial scleral flap. The deep scleral flap was then excised with Vannas scissors, taking care not to rupture Descemet’s membrane. Ab externo Schlemm’s canal dilation with a 30 G cannula (meshwork shaver, NIPRO, Japan) was performed at least 90° away from the deep scleral sidewalls. The JCT adjacent to Descemet’s membrane was gently removed with fine forceps. The superficial scleral flap was securely sutured in position with 10-0 nylon sutures. Conjunctival sutures were placed with 9-0 silk.
Specimen preparation and transmission electron micrography
The JCT was removed from the patient’s eyes by the same surgeon (MN). The surgical specimens were prepared for transmission electron micrography by a pathologist (TT). The JCT was immediately fixed in 2.5% glutaraldehyde and then washed in sodium acetate buffer to remove the glutaraldehyde fixative. Dehydration was accomplished by exposing the tissue to a graded ethanol series (50%–100%). Following conventional processing with epoxy resin embedding (Agar Scientific, Stansted, UK), semithin sections (~2 µm) were cut on a microtome (PYRAMITOME, LKB, Sweden) and stained with toluidine blue to confirm tissue location with light microscopy. Ultrathin sections (~90 nm thick) were cut on an ultramicrotome (LKB8800, LKB) and stained for transmission electron micrography with saturated aqueous uranyl acetate for 20 min, followed by washing with filtered distilled water. Finally, the JCT tissue was stained with lead for 10 min, followed by washing in filtered distilled water. Sections were examined with a JEM-1400 transmission electron microscope (Jeol UK, Welwyn Garden City, UK) operating at 80 kV. We evaluated three to five sections and selected one section with a good location for observing the elastin fibres and type VI collagen. Electron micrographs were obtained by a pathologist (NF) with an ORIUS SC1000 charge-coupled device camera (Gatan, Pleasanton, CA) at 30 000X magnification. Information regarding ripasudil treatment was masked to prevent biased analysis by the observer (NN). The observer was not involved in data acquisition or data analyses.
Measurements of morphological changes
Type VI collagen has cross-banded aggregates characterised by a pattern of transverse bands approximately 30 nm apart and occurring approximately every 105 nm. The transverse bands are referred to as the ORR and the intervals are referred to as the inner rod-like region (IRR).18–20
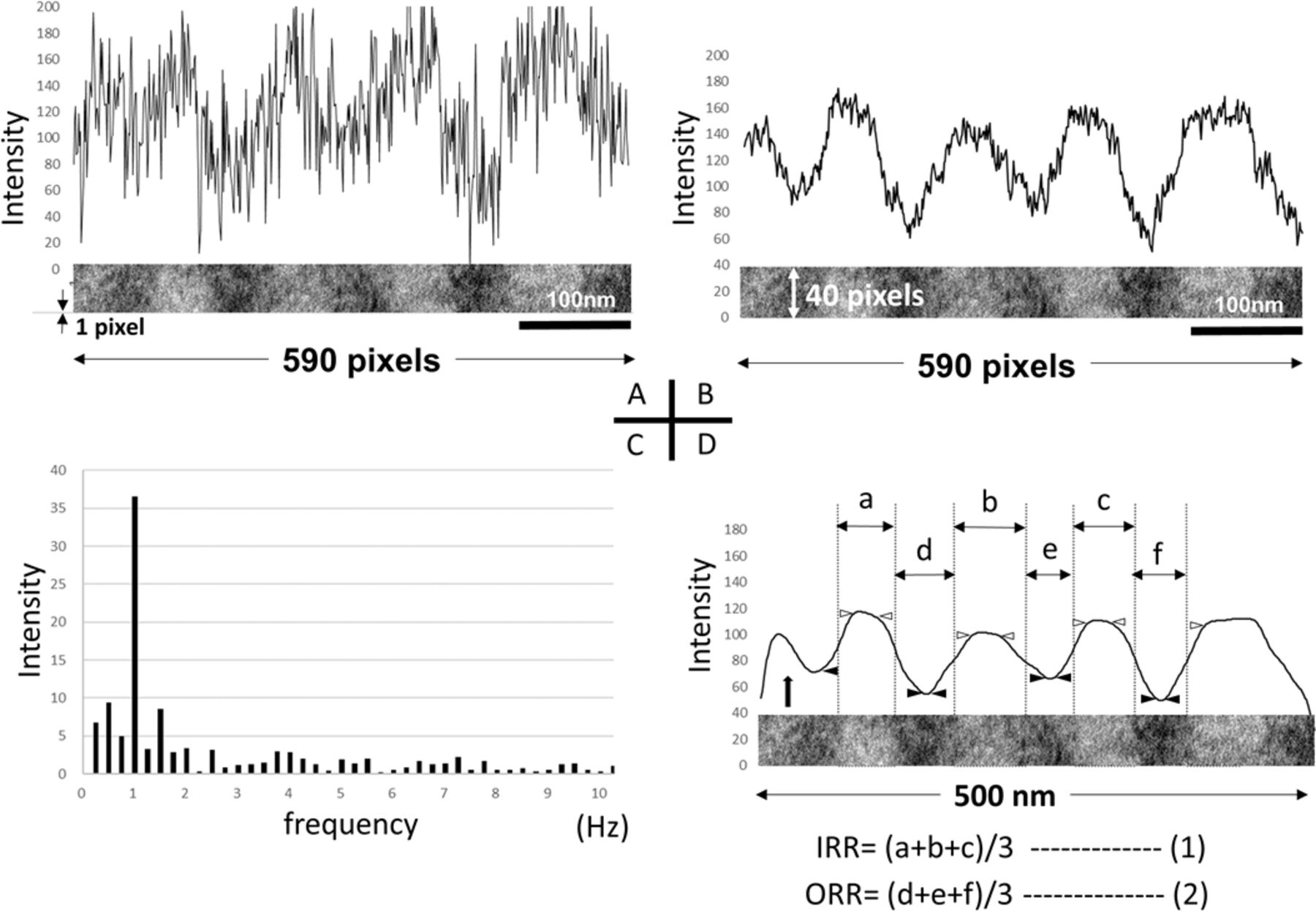
The intensity of the greyscale images was divided into 256 (0–255) values from black to white. The image intensity value on the one-pixel line in the periodic component with the IRR and the ORR formed periodic waves in electron micrographs at 30 000X magnification (figure 1A). To increase the accuracy, we calculated the mean values of the periodic waves in an area of type VI collagen 34 nm (40 pixels) vertically and 500 nm (590 pixels) horizontally in electron micrographs at 30 000X magnification (figure 1B). The periodic waves in each case were analysed using a Fourier transform to detect the major modulation cycle based on 1/105 nm frequency (figure 1C). The major waveform, which excluded the other waves, was used to detect the IRR and ORR borders (figure 1D).

Measurement procedure for type VI collagen. An electron micrograph image (34×500 nm) obtained at 30 000X magnification of type VI collagen located around elastin fibres. Due to the large variation in the amplitudes of the waveform of a single line (1×590 pixels, A), the mean of 40 vertical pixels was used to smooth the waveform (B). The averaged waveform data were transformed by Fourier transform to detect the major frequencies. The highest intensity frequency was detected at around 1 Hz (1/105 nm) (C). The major waveform that excluded the other waves (>10 Hz) from the averaged waveform (D, black arrow) was used to detect the IRR and ORR borders. The IRR and ORR borders were detected using a mathematical method (D, dotted lines) with median intensity values having variations greater than 0.2 in the border area between the IRR and ORR (D, white and black arrowheads). The width of each segment was measured (D, a–f) and averaged (D, (1) and (2)) for the continuous waveform data. IRR, inner rod-like region; ORR, outer rod-like region.
The IRR and ORR borders were defined mathematically. The median value of pixel intensity on the waveform (figure 1D, point where the dotted line and the waveform line intersect) with variations over 0.2 in the border area between the IRR and ORR (figure 1D, between the black arrowhead and white arrowhead) was calculated as the border of the IRR and ORR. The width of the IRR and ORR was calculated in three successive regions to obtain a mean value (figure 1D). These measurement processes were repeated three times in each case. Measurement images for analysis in each case were obtained by an analyst (MO) using image analysis software (PopImaging, VECTOR, Japan) and mathematical analyses were performed by a mathematician (KN).
Statistical analysis
Data are presented as means±SD. Comparisons of the two groups were performed using the Mann-Whitney U test. Correlations of the two variables were tested using the Spearmen’s rank correlation coefficient. Differences were considered statistically significant at p<0.05.
Results
Ten eyes of 10 patients were included in the study. Table 1 shows the patient characteristics. Mean deviation (MD) of the Humphrey visual field analyser programme central 24-2 was measured before surgery. Medication score was defined as the number of antiglaucoma agents. Mixed drops were counted as two agents. Drops of the prostaglandin F2α analogues tafluprost, bimatoprost and latanoprost, mixed with timolol were instilled once daily at approximately 08:00. Drops of dorzolamide mixed with timolol, brimonidine and ripasudil were instilled twice daily at approximately 08:00 and 20:00. Drops of brinzolamide and dorzolamide were instilled three times a day at approximately 08:00, 14:00 and 20:00. When multiple drops were administered, the drops were applied at least 5 min apart. All surgeries were performed in the afternoon from 14:00 to 17:00. The time interval from instilling the ripasudil to the surgery ranged from 6 to 9 hours. The surgical time was approximately 40 min in every case. IOP was measured at 17:00 on the day before surgery. Postoperative IOP was measured for follow-up observation at 14:00 2, 4, 8 and 12 weeks after surgery in an outpatient clinic. The NRA group comprised five eyes of five patients (five men; mean age (mean±SD) 71.4±3.2 years, range 67–76; mean MD −9.89±4.14 dB, preoperative mean IOP 19.0±5.2 mm Hg, range 11–24; postoperative mean IOP 11.6±1.8 mm Hg, range 10–14; preoperative mean medication score 2.0±1.2, range 0–3; and postoperative mean medication score 0.6±1.3, range 0–3). The RA group comprised five eyes of five patients (three men, two women; mean age (mean±SD) 72.6±7.8 years, range 61–79; mean MD −16.73±8.43 dB, preoperative mean IOP 17.8±2.2 mm Hg, range 14–20; postoperative mean IOP 12.6±2.1 mm Hg, range 10–15; preoperative medication score 3.6±1.1, range 2–5; and postoperative mean medication score 1.2±1.6, range 0–3). The baseline patient characteristics did not differ significantly between the two groups. Mean IOP and mean medication score were significantly decreased after surgery in both groups (p<0.05).
Patient characteristics
In each case, electron micrographs at 10 000X and 30 000X magnifications of type VI collagen near the elastin fibres, a photographic condition considered good for analysis, were selected. Figure 2 shows representative measurement processes in case 4 of the NRA group and case 6 of the RA group. The areas depicted by the white rectangle at 10 000X magnification in figure 2A-1(case 4) and figure 2A-2(case 6) are shown at 30 000X magnification in figure 2B-1 and B-2, respectively. The 34×500 nm area located around the elastin fibres indicated by the white rectangle in figure 2B-1 and B-2 was used to measure the width of the IRR and ORR. Figure 3 shows the IRR and the ORR measurement results in the remaining cases in both the NRA group (cases 1, 2, 3 and 5) and RA group (cases 7, 8, 9 and 10). The measurement repeatability error after three measurements was under 1% in each case. Figure 4 shows the statistical analysis of the mean width of the IRR and ORR for each case. The ORR width was significantly smaller in the RA group (37.85±3.43 nm, n=5) than in the NRA group (50.62±5.23 nm, n=5, p<0.01), whereas the IRR width was significantly greater in the RA group (70.68±10.84 nm, n=5) than in the NRA group (58.19±5.34 nm, n=5, p<0.05).

Representative measurement procedure of type VI collagen in case 4 of the no ripasudil eye drop administration (NRA) group and case 6 of the ripasudil eye drop administration (RA) group. Electron micrographs of the juxtacanalicular tissue obtained at 10 000X magnification (A-1, case 4 of the NRA group; A-2, case 6 of the RA group, black bar, 2.0 μm) and 30 000X magnification (B-1, case 4 of the NRA group; B-2, case 6 of the RA group, black bar, 500 nm) are shown. The elastic fibres (asterisks) in the extracellular matrix (ECM) are surrounded by type VI collagen and various other components of the ECM. One section was selected that was well suited for visualising the elastic fibres. The areas depicted by the white rectangles at 10 000X magnification in A-1 and A-2 are shown at 30 000X magnification in B-1 and B-2, respectively. The averaged waveform (C, case 4 of the NRA group; D, case 6 of the RA group, white arrow) was transformed by Fourier transform to detect the major frequencies. The highest intensity frequency was detected at around 1 Hz (1/105 nm). The major waveform that excluded the other waves (>10 Hz) from the averaged waveform (C, case 4 of the NRA group; D, case 6 of the RA group, black arrow) was used to detect the IRR and ORR borders. The width of each segment was measured (C, case 4 of the NRA group; D, case 6 of the RA group, a–f) and averaged (C, case 4 of the NRA group; D, case 6 of the RA group, mean± SD) in the continuous waveform data. IRR, inner rod-like region; ORR, outer rod-like region.

Measurement of the IRR and ORR width in the NRA and RA groups. Measurement of type VI collagen in four cases in each group is shown. The intensity and contrast of the greyscale images varied among the cases due to the staining conditions for transmission electron micrography. Although the greyscale intensity in cases 1 and 2 had low variability, the IRR and ORR borders were accurately detected by the measurement process as described in figure 2. The averaged width of the IRR and ORR in each case of the NRA group ranged from 52.26 to 63.84 nm and from 45.20 to 57.62 nm, respectively, whereas those in the RA group ranged from 59.04 to 88.98 nm and from 34.75 to 41.24 nm, respectively. IRR, inner rod-like region; NRA, no ripasudil eye drop administration; ORR, outer rod-like region; RA, ripasudil eye drop administration.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Statistical analysis of the mean width of the IRR and ORR in each group. The mean width of the IRR and ORR for each case is shown. The ORR width was larger in the NRA group (cases 1–5) than in the RA group (cases 6–10), whereas the IRR width was smaller in the NRA group than in the RA group, except for case 7. The mean ORR width was significantly greater in the NRA group than in the RA group (p<0.01), whereas the IRR width was significantly smaller in the NRA group than in the RA group (p<0.05). IRR, inner rod-like region; NRA, no ripasudil eye drop administration; ORR, outer rod-like region; RA, ripasudil eye drop administration.
We also evaluated the association between the length of ripasudil administration and the type VI collagen width. The correlation coefficient between the ripasudil use period and the IRR or the ORR width was 0.41 (p=0.52) and −0.051 (p=0.95), respectively, whereas the type VI collagen total width (IRR width+ORR width) was 0.9 (p=0.08). Therefore, the progression of morphological changes in the IRR and the ORR width may differ with the ripasudil use period as the type VI collagen total width tended to correlate with number of months of ripasudil administration. The transverse double bands were not observed in any case of the major waveform.
Discussion
In this study, we investigated morphological changes in the type VI collagen of human TM associated with the ROCK inhibitor ripasudil in patients with POAG. Previous reports indicated that type VI collagen is a key ECM component of the TM.16 17 In an in vitro human TM cell experiment, prostaglandin F2α differentially regulated the aqueous humour outflow pathway via two mechanisms: decreasing ECM accumulation to reduce outflow resistance and increasing TM contraction.32 In the NRA group, case 5 did not administer the eye drops before surgery, yet there was no significant difference in the IRR or ORR width compared with the other cases in the NRA group who administered the prostaglandin F2α analogues, suggesting that prostaglandin F2α analogues do not markedly affect the morphological changes in type VI collagen.
Postoperative IOP was significantly reduced after conventional outflow reconstruction surgery, which included ab externo Schlemm’s canal dilation and JCT removal. Antiglaucoma medication was still necessary after surgery in case 3 in the NRA group and in cases 7 and 9 in the RA group. In these cases, outflow resistance may have extended beyond the collector channel.
Tanihara et al 33 reported a clinical evaluation of the effects of ripasudil on IOP reduction in patients with POAG. According to their report, twice-daily (09:00 and 21:00) ripasudil administration reduced IOP (obtained at 11:00) by approximately 18% within 2 hours for up to 6 months, and the IOP was further reduced when ripasudil was administered twice-daily (09:00 and 21:00) for more than 6 months. Kaneko et al 22 reported that ripasudil transiently induces retraction and rounding of cell bodies, which disrupts actin bundles in TM cells at 1 hour after administration. Recovery of actin bundles was observed 2 hours after removing the agent. These findings suggest that IOP reduction within 2 hours is due to a decrease in the outflow resistance associated with the modulation of TM cell behaviour.
We considered the possible reasons for the slightly greater IOP reduction following ripasudil administration for more than 6 months. Koga et al 34 reported that Y-27632, a selective ROCK inhibitor, reduced type I collagen production and prevents contraction in an in vitro experiment using human trabecular cells. Last et al 35 reported that the stiffness of the human donor TM is increased and the thickness of the TM is reduced in glaucomatous eyes compared with normal eyes. Yan et al 36 reported a significantly lower TM thickness in patients with POAG compared with normal eyes, as measured by ultrasound imaging. The TM in patients with POAG is very thin, and significantly stiffer than that in normal eyes. In the present study, the RA group included a patient with moderate to severe glaucoma that may have had increased stiffness and reduced thickness of the JCT before ripasudil administration. Although IOP reduction is not sufficient to prevent glaucoma progression, the morphological changes in the type VI collagen total width tended to correlate with the duration of ripasudil administration. These results suggest that the progression of morphological changes in type VI collagen in the RA group may be associated with the duration of ripasudil administration and reduced tissue stress in the JCT.
Type VI collagen aggregates also have additional transverse double banding halfway between the main pairs of bands in Bruch’s membrane in the human retina,19 whereas the aggregates in TM in human eyes generally have only single transverse banding that repeats axially every 105 nm. Koudouna et al 20 reported that single-banded assemblies are prevalent, suggesting that extra material accumulates in the space between the globular domains. In the present study, the width of the ORR and IRR in the NRA group was modified by 68.7% and 22.4%, respectively, compared with the basic structure, whereas the width of the ORR and IRR in the RA group was modified by 26.1% and 5.8%, respectively, compared with the basic structure. We observed no transverse double bands in any case and the width of the ORR was increased compared with the basic structure. These findings suggest that changes in the ORR are morphological and include the accumulation of extra materials around the ORR in the space of non-covalent bonds between the N-terminal and C-terminal of the globular domains. Type VI collagen aggregates underwent morphological changes with compression and collapse by accumulation and contraction of the ECM and IOP elevation, whereas ripasudil may have decreased these stressors depending on the duration of the administration period.
Potential limitations of the present study include the small number of patients (n=10), the limited age range and older age (60–80 years) and the unclear disease period. Further studies are needed to examine a larger number of patients, a younger sample and a well-defined disease period.
Conclusions
Morphological changes associated with ripasudil in the type VI collagen of human TM were evident on electron micrographs. Changes in the ORR width were significantly smaller and those in the IRR width were significantly greater in patients with POAG with ripasudil.
References
Footnotes
Presented at American Academy of Ophthalmology in 2017.
Contributors All authors were involved in the research design. MO collected the data, interpreted the data and prepared the manuscript. MN performed the glaucoma surgery, interpreted the data and submitted the manuscript. TT prepared the surgical specimens for transmission electron micrography. NN masked patient information regarding ripasudil treatment. NF obtained electron micrographs and interpretation. KN conducted the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study adhered to the tenets of Declaration of Helsinki and was approved by the Institutional Review Board of Tokai University Hachioji Hospital (approval number R-115).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no data in this work.
Linked Articles
- At a glance