Article Text

Abstract
Background/aims Survival after diagnosis of metastasis from uveal melanoma is poor. Identifying individuals at high risk for metastasis and developing adjuvant therapy to prevent clinically apparent metastasis could improve survival. We conducted an adjuvant trial of sequential, low-dose dacarbazine (DTIC) and interferon-alpha-2b (IFN-α−2b) in patients with cytogenetic high-risk uveal melanoma.
Methods Patients diagnosed with iris, ciliary body or choroidal melanoma with high-risk tumour cytogenetics (monosomy 3) were offered adjuvant treatment with low-dose DTIC and IFN-α−2b following primary therapy. Eligible but not enrolled patients were observed for comparison. DTIC was administered at 850 mg/m2 intravenously on days 1 and 28. IFN-α−2b was administered at 3 million units three times a week subcutaneously for 24 weeks beginning at week 9. Hepatic imaging was performed prior to adjuvant therapy and then at least every 6 months. Survival data were collected for 5 years after enrolment.
Results 33 patients (22%) were enrolled (treatment group), 29 (19%) were eligible but did not enrol (observation group) and 88 (59%) were not eligible. The 5-year metastasis-free survival (MFS) was 64%±9% for treated and 33%±10% for observed patients (p=0.05). The 5-year overall survival (OS) rate was 66%±9% for treated and 37%±10% for observed patients (p=0.02).
Conclusions When adjusted for differences in age, tumour size and initial treatment, survival between treated and observed patients was no longer significant (p=0.56 MFS and p=0.92 OS). Differences in baseline tumour characteristics between treated and observed patients can influence interpretation of results.
Trial registration number NCT01100528.
- uveal melanoma
- adjuvant therapy
- metastasis
Statistics from Altmetric.com
Introduction
While advances in local therapy for uveal melanoma have resulted in a 95% or greater local tumour control rate, the development of metastatic disease following primary treatment remains a challenge.1 2 Only 2.1% of patients with uveal melanoma present with metastatic disease at the time of diagnosis of their primary tumour.3 However, longitudinal follow-up from the Collaborative Ocular Melanoma Study showed that 34% of patients will develop metastatic disease within 10 years.3 4 Survival after diagnosis of metastatic disease is poor, with 80% of patients dying within 1 year of diagnosis of metastasis.4 Moreover, data derived from the Surveillance, Epidemiology, and End Results database indicate a lack of improvement in survival of patients with uveal melanoma between 1973 and 2013.5
Multiple lines of evidence suggest that micrometastatic disease likely occurs early in the disease course.6 7 Up to 18% of patients with uveal melanoma without clinical evidence of metastatic disease may have histopathological evidence of metastasis at autopsy.8 Proposed mechanisms by which tumour cells may remain dormant have included immunologic variables, angiogenic factors and tumour cell quiescence models.7
In the present era, neither chemotherapy, immunotherapy, nor small-molecule biologics have been shown to improve survival in patients with metastatic uveal melanoma.9 Therefore, identifying patients at high risk for metastatic disease at presentation and treating such individuals with adjuvant therapy to prevent the development of clinically apparent metastasis has the potential to improve survival.
Both dacarbazine (DTIC) and interferon-alpha (IFN-α) have shown efficacy in the treatment of metastatic uveal melanoma in murine models.10–12 Given that IFN-α exerts anti-tumour activity through its actions on natural killer cells in addition to other immune effectors, and that DTIC can sensitise tumours to immune effectors, these agents may work synergistically to prevent the development of clinically apparent metastatic disease.13 14 A meta-analysis of >3000 patients concluded that the combination of DTIC plus IFN-α produced a response rate 53% greater (95% CI: 1.10 to 2.13) than that seen with DTIC alone.15 Such a combination therapy could be effective in the adjuvant setting that is supported by a trial reported by Stadler et al involving 252 patients with cutaneous melanoma.12 Patients randomised to 6 months of sequential low-dose regimen of DTIC followed by IFN-α after surgery manifested a reduction of melanoma-associated deaths compared with those randomised to no systemic treatment,12 but a concurrent, DTIC-IFN-α regimen was not effective.12 16
Hence, we chose sequential low-dose DTIC and interferon-alpha-2b (IFN-α−2b) as adjuvant therapy for uveal in patients that had high-risk tumour cytogenetics. Herein, we present 5-year survival outcomes of patients enrolled in an adjuvant therapy open label phase II study.
Materials and methods
Patients and treatment
This trial was conducted in parallel with a trial of prognostic fine-needle aspiration biopsy which has been previously published.17 In all, 150 consecutive patients with a clinical diagnosis of uveal melanoma were enrolled in the prognostication study. Clinical diagnosis of melanoma was confirmed using slit lamp examination, gonioscopy, indirect ophthalmoscopy (where indicated) and with ancillary imaging as previously described.17 American Joint Committee on Cancer (AJCC) stage was calculated for each patient based on tumour clinical parameters. Fine-needle aspiration biopsy using a transcorneal, trans-scleral or transvitreal approach was performed depending on the location of the tumour.17 Cytology was performed for diagnosis in each case and where there was sufficient cellularity, the chromosome 3 status was assessed by fluorescent in situ hybridisation with directly labelled SpectrumGreen and SpectrumOrange enumeration probes for the alphacentromeric locus of chromosome 3 and a locus-specific probe, 3p26 (TelVysion 3 p, Abbott Molecular Vysis, Des Plaines, IL, USA).17 18 In all, 200 interphase cells were scored to determine the percentage of signals per locus.17 Based on previous studies, a cut-off of monosomy 3 in ≥20% of cells was used to define high-risk tumour cytogenetics.19 20
Inclusion criteria
Patients with high-risk tumour cytogenetics (monosomy 3≥20% of cells), adequate primary therapy (enucleation, brachytherapy or resection), negative baseline systemic staging with CT scan of the chest, abdomen and pelvis with contrast, performance status (Eastern Cooperartive Oncology Group) less than 2 and normal organ function were offered enrolment in the adjuvant therapy trial. Patients had to be entered within 56 days of completing primary therapy. DTIC was administered at 850 mg/m2 intravenously on day 1 and day 28. IFN-α−2b was administered at 3 million units (MU) three times a week subcutaneously for 24 weeks beginning at week 9. Toxicity was graded using National Cancer Institute Common Toxicity Criteria (Version 2.0). With the exception of haematologic toxicity, dosing was held and modified for grade 3 or 4 toxicities. IFN-α-2b was withheld for Grade 4 neutropenia, that is, absolute neutrophil count (ANC)<500/mm3, and restarted at 1.5 MU when ANC≥1000/mm3. Baseline staging was done with CT and subsequent surveillance (every 6 months) with by hepatic ultrasonography as per standard of clinical practice.21 Any suspicious findings on liver ultrasonography were confirmed by hepatic CT/MRI prior to liver biopsy. Follow-up data were collected for 5 years after enrolment of the last patient in the trial (figure 1).
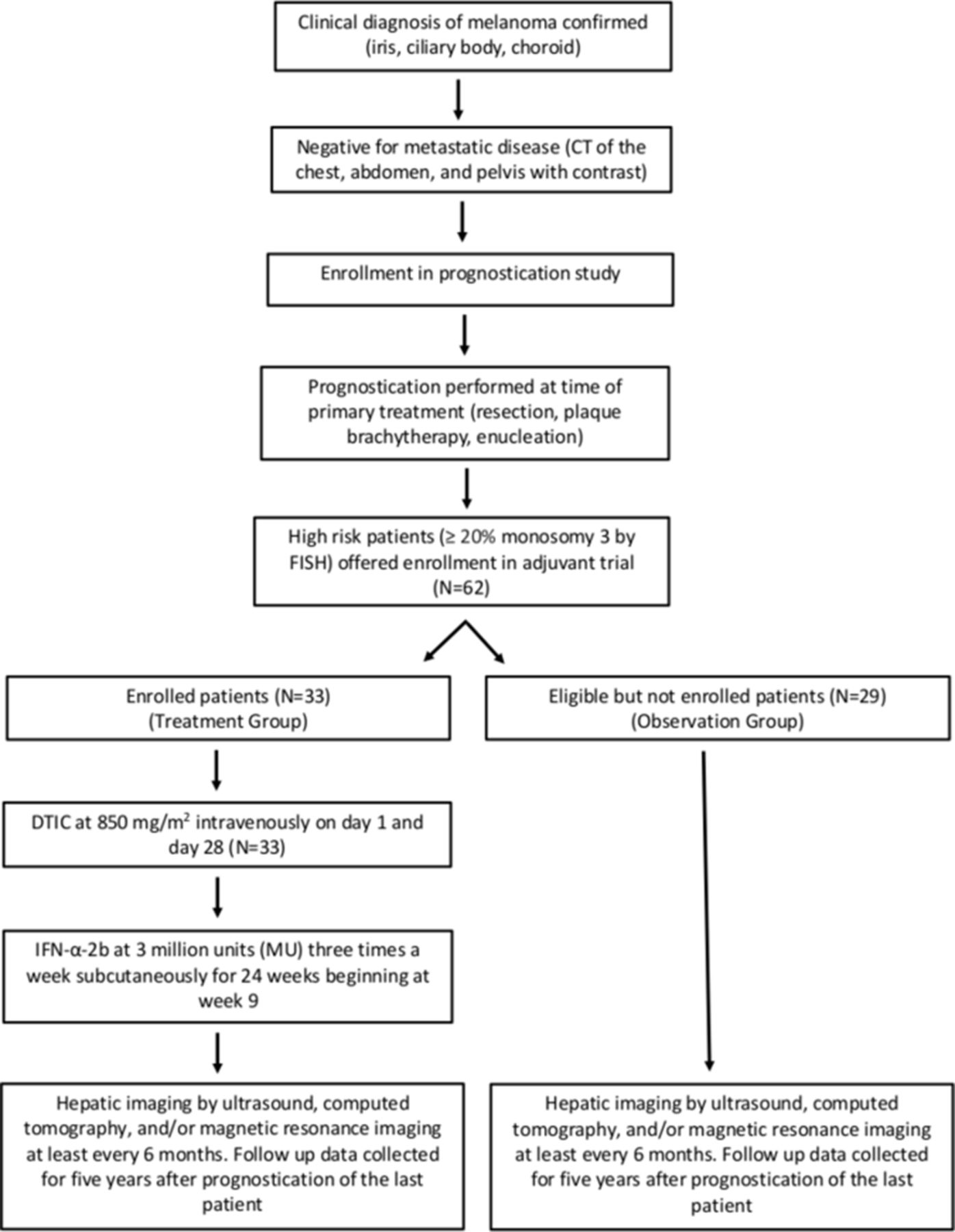
Study design of adjuvant therapy trial of DTIC and IFN-α−2b in patients with uveal melanoma and high-risk cytogenetics. Patients with a clinical diagnosis of choroidal melanoma (iris, ciliary body and choroid) were offered enrolment in a parallel prognostication study following a negative baseline metastatic evaluation. High-risk patients (≥20% monosomy 3) were offered enrolment in the adjuvant therapy trial with treatment with DTIC and IFN-α−2b per protocol. In all, 33 patients enrolled in the trial (treatment group) and 29 eligible patients did not enrol (observation group). Both groups of patients were followed with hepatic imaging at least 6 month intervals for 5 years after prognostication of the last patient. DTIC, dacarbazine;IFN-α−2b, interferon-alpha-2b.
Statistical analysis
Study sample size
Precher et al reported a 3-year metastasis-free survival (MFS) rate for patients with monosomy 3 of 50%.22 This translates to a 2-year rate of 63% with an assumption that MFS follows an exponential distribution. For the purposes of this clinical trial, treatment would be considered ineffective if the 2-year MFS was <60%, and the combination would be considered promising if the MFS was >80%.
Statistical power analysis
Based on the current status of accrual at our institution, it was estimated that over 3 years, a maximum of 36 eligible and evaluable patients would be needed to provide >80% power to detect an increase in the 2-year MFS from 60% to 80% base on a two-sided test with a type 1 error of 0.05
Analysis
Data were summarised as frequency counts and percentages (categorical variables) or median and range (continuous variables). Baseline characteristics were compared between treated and observed patients with χ2 test, Fisher’s exact test or Wilcoxon rank sum test. MFS was defined as the time from primary therapy to the first sign of metastatic disease or death from any cause; patients who were alive without disease at last follow-up were censored. Overall survival (OS) was calculated from the date of primary treatment to the date of death from any cause; patients who were alive at last follow-up were censored. Both outcomes were estimated with the method of Kaplan-Meier and compared between treated and observed patients with the log-rank test. Five-year estimates of MFS and OS are presented with 95% CIs. Cox proportional hazards analysis was used to assess the effect of treatment versus observation on MFS and OS after adjusting for other prognostic factors. Candidate adjustment factors included gender, age, involved eye, tumour location, monosomy 3, tumour diameter and initial treatment. Results were summarised as HR and 95% CI. All statistical analyses were performed using SAS software V.9.4 (SAS Institute, Cary, NC, USA).
Results
In all, 150 patients were enrolled in the prognostication trial. Of these patients, 33 patients with high-risk cytogenetics (22%) enrolled in the adjuvant therapy trial (treatment group), 29 (19%) were eligible for the trial but did not enrol (observation group) and 88 (59%) with low-risk cytogenetics were not eligible for the trial (figure 1). Overall, among 62 eligible patients with high-risk cytogenetics, 50% were men, median age at initial surgery was 64 years (range: 20–91), and 66% had choroidal tumours. The median tumour diameter was 14.5 mm (range: 2.4–25.0) and AJCC stage was distributed fairly evenly (18% stage 1, 29% stage 2, 24% stage 3 and 18% stage 4). Initial treatment was plaque brachytherapy in 52%, enucleation in 45% and local resection in 3% (table 1).
Patient characteristics (treated and observed patient groups)
Patients in the treatment and observation groups differed with respect to age, basal tumour diameter and AJCC stage with treated patients being younger (median age 59 vs 73 years, p=0.0002), having smaller tumours (median basal diameter 13.0 vs 16.0 mm, p=0.04) and lower AJCC stage (p=0.03) when compared with observed patients (table 1).
Therapy was well tolerated. All treated patients received the prescribed doses of DTIC and IFN-α−2b. Grade 1 or 2 fatigue, reported by 33 patients (87%), was most common. Grade 1 or 2 elevations in hepatic transaminases were observed in 14 patients (37%), and grade 1 or 2 depression, in five patients (13%). Grade-3 haematological toxicity was observed in six patients while on IFN-α−2b that was dose-limiting. No grade 4 adverse events were reported. Ocular toxicities were not observed.
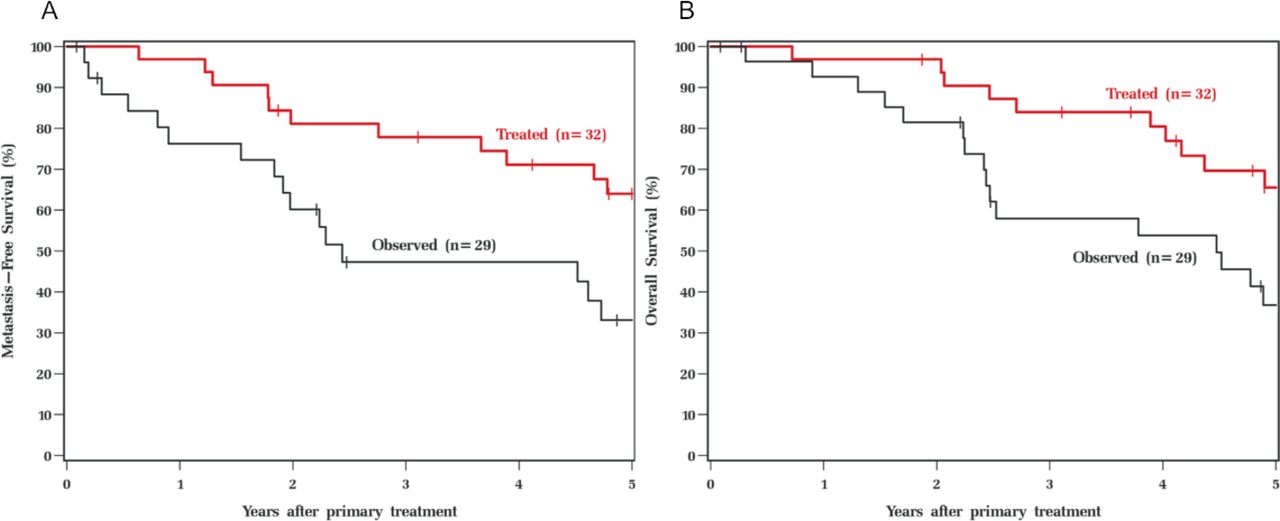
One patient was lost to follow-up and was not included in calculations of MFS or OS. Among 28 patients who were alive and metastasis-free, median follow-up was 62 months (range: 1–86), with 79% having at least 4 years and 64% having at least 5 years of follow-up. In univariable Cox analysis, observed patients had worse MFS (HR: 2.10, CI: 1.00 to 4.41, p=0.05) and OS (HR: 2.41, 95% CI: 1.13 to 5.16, p=0.02) relative to treated patients. Five-year and median MFS were 64% (44–78) and 79 months in treated patients and 33% (15–52) and 29 months in observed patients (figure 2A). Five-year median OS was 66% (45–80, median not observed) in treated patients and 37% (19–55, median 54 months) in observed patients (figure 2B).

{kind=link}
{kind=link}
Metastasis-free (A) and overall survival (B) of treated and observed patients. In univariable analysis, treated patients had improved and metastasis-free survival (A) and overall survival (B) compared with observed patients.
On multivariable analysis, using factors identified to be significant by univariate analysis (table 1), age and initial treatment modality were independent predictors of MFS and age and tumour diameter were independent predictors of OS; treatment versus observation was not significant for either outcome. When treatment versus observation was added to these models, the observed difference in MFS and OS between the groups was no longer significant (p=0.56 and p=0.92, respectively) (table 2).
Multivariable analysis of metastasis-free and overall survival
Discussion
Several published adjuvant studies conducted prior to the development of molecular methods of prognostication have been largely ineffective.23–25 Methanol-extract bacilli Calmette-Guerin vaccine, IFN-α−2a, IFN-α−2b, intra-arterial hepatic fotumustine and DTIC monotherapy have been unsuccessful in improving survival in patients at high risk for metastasis, prognosticated based on clinical features.23–27
Molecular strategies such as chromosome analysis, multiplex ligation-dependent probe amplification (MLPA) and gene expression profiling (GEP) have now enhanced our ability to accurately prognosticate and identify patients who would benefit the most from adjuvant therapy.28–30 There are several trials that are either in progress or were terminated due to lack of accrual. The decision to undergo prognostication test in a disease wherein adjuvant therapy is unavailable or ineffective can be emotionally complex.31 Although all patients with high-risk cytogenetics were offered enrolment in this adjuvant trial, only about half of the patients (47%, 29 of the 62 eligible patients enrolled). In general, several factors such as burden of excessive testing, older age, existing comorbidity, potential drug toxicity and frequent hospital visits can deter patients from prognostication32 and/or entering an adjuvant therapy trial.33 Given that this was an exploratory study, randomisation was not conducted. If the results were encouraging (positive), a confirmatory randomised study would have been conducted.
Excluding the present study, there are only two published adjuvant therapy trials using cytogenetic molecular risk stratification as inclusion criteria (table 3).34 35 A recent retrospective cohort study of the tyrosine kinase inhibitor sunitinib in high-risk patients as defined by tumour monosomy 3 and 8q amplification, monosomy 3 and AJCC class 3 or 4, or class 2 GEP profile showed promise in improving survival in patients with high-risk tumours.35 However, the patients in the treated group were both younger and with smaller tumours than the institutional controls used for comparison in the study.35
Published risk stratified adjuvant therapy trials for uveal melanoma using molecular techniques
While the findings of our study indicate that low-dose DTIC and IFN-α−2b therapy does not appear to be effective at reducing MFS or OS, these findings remain important given that they highlight the role that clinical features play in determining metastatic risk and therefore these variables must be carefully considered when interpreting the results of non-randomised adjuvant therapy trials when not matched for baseline prognostic characteristics. While there did initially appear to be a statistically significant improvement in MFS and OS, these differences were no longer significant after accounting for differences in age and tumour size. Larger tumours were more likely to be treated with enucleation rather than globe sparing therapy likely accounting for the difference in outcomes based on initial treatment modality. Patients in the treatment group had smaller tumours and were younger than patients in the observation group despite having similar high-risk tumour cytogenetics.
Although molecular methods of prognostication including tumour chromosome analysis and GEP testing provide validated methods prognostication for patients with uveal melanoma, incorporation of tumour size seems to enhance overall prognostication.28 30 36 Dogrusoz et al showed AJCC size criteria for prognosis were enhanced by the addition of tumour chromosome analysis.36 The findings of the present study support the need to consider both clinical and molecular data when designing and interpreting the results of adjuvant therapy trials.
As with any therapeutic trial of a rare disease, the number of patients treated in this study were relatively small (n=33). While there was no statistically significant improvement in survival after 5 years between treated and observed patients when adjusted for the variables described above, it is possible that with an increased number of patients, a significant treatment effect may have been observed.
In summary, we did not find a significant improvement in 5-year survival outcomes in patients with uveal melanoma with high-risk cytogenetics who were treated with adjuvant low-dose DTIC and IFN-α−2b. These data highlight the importance of considering both clinical and molecular data when designing and assessing outcomes in adjuvant therapy trials for uveal melanoma.
References
Footnotes
Contributors EB: Data interpretation, drafting, critical revision manuscript. PLT: Study design, data acquisition, data interpretation, drafting manuscript. LR: Data analysis and interpretation, critical revision of manuscript. SA: Data analysis and interpretation. WA: Data analysis and interpretation. AS: Study design, data acquisition, data interpretation, drafting and critical revision of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study was approved by the Institutional Review Board (IRB) at the Cleveland Clinic and Case Comprehensive Cancer Centre (note that the study was conducted at the Taussig Cancer Centre at the Cleveland Clinic, there is a combined IRB for the cancer centres at the Cleveland Clinic and Case Western Reserve University).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance