Article Text

Abstract
Purpose To assess changes in the position of lamina cribrosa pores (LCPs) induced by acute intraocular pressure (IOP) elevation.
Methods A prospective observational study. Acute angle-closure suspects who underwent the 2-hour dark room prone provocative test (DRPPT) were included. At baseline and within 5 min after the DRPPT end, tonometry, fundus photography and optical coherence tomography were performed. Optic disc photos taken before and after the DRPPT were aligned and moving distance of each visible LCP was measured (LCPMD).
Results 38 eyes from 27 participants (age: 52.5±10.8 years) were included. The IOP rose from 16.7±3.2 mm Hg at baseline to 23.9±4.3 mm Hg at the DRPPT end. The mean lateral LCPMD was 28.1±14.6 µm (range: 5.0–77.2 µm), which increased with higher IOP rise (p=0.01) and deeper optic cup (p=0.02) in multivariate analysis. The intralamina range and SD of the LCPMD increased with younger age (p=0.01 and p=0.02, respectively) and with wider optic cup (p=0.01 and p=0.02, respectively). The LCP movements were headed to the superior direction in 12 (33%) eyes, inferior direction in 10 (28%) eyes, temporal direction in 9 (25%) eyes, and nasal direction in 5 (14%) eyes.
Conclusions IOP rise is associated with LCP movements in the frontal plane, which are more pronounced with higher IOP rise and deeper optic cup. The intralamina variability in the IOP rise-associated LCPMD increased with younger age and wider optic cup. IOP variation-associated lateral LCP movements may be of interest to elucidate glaucomatous optic nerve damage.
- Glaucoma
- Imaging
- Intraocular pressure
- Optic Nerve
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Glaucoma is one of the leading causes for irreversible blindness worldwide.1 Intraocular pressure (IOP) plays a key role in the pathogenesis and progression of glaucomatous optic neuropathy, for both high-tension glaucoma and normal-tension glaucoma.2 3 Bearing the IOP-related strain and stress, the lamina cribrosa has been assumed to be the principal site where the damage to the retinal ganglion cell axon occurs.4 The tissue compliance of the optic nerve head and the sclera with respect to the IOP has been examined ex vivo and in vivo in previous investigations.5–9 These and other studies suggested that the lamina cribrosa undergoes a posterior displacement and backward bowing in eyes with an increased IOP.10–14
The lamina cribrosa is composed of lamina cribrosa pores (LCPs) which differ in their size, shape and visibility between various regions of the optic nerve head and between glaucomatous eyes and normal eyes.15 16 The biomechanical properties of the lamina cribrosa have been assessed using models in most of which the lamina cribrosa was considered to be mainly a uniform structure, in contrast to its complex three-dimensional anatomy.7 10 13 14 It has remained unclear whether the various lamina cribrosa regions react differently to variations in IOP. While it has remained technically difficult to visualise the deep lamina cribrosa layers, it is possible to image and analyse the structure of the superficial lamina cribrosa layer with its ophthalmoscopically detectable pores. Since the assessment of changes in the superficial lamina cribrosa layer and its pores under conditions of a varying IOP may give some hints for IOP-related changes in the deep lamina cribrosa layers and may thus be helpful to further elucidate the biomechanics of the lamina cribrosa, we performed the present study in which we compared optic disc photographs taken in angle-closure suspects at baseline of a 2-hour dark room prone provocative test (DRPPT) and shortly after the test end. We chose angle-closure suspects as study participants since their eyes may experience an almost physiological or pathophysiological rise in their IOP when their pupils get dilated under dark room adaptation conditions.
Methods
Study design and participants
This is a prospective observational study, which included angle-closure suspects who routinely and consecutively underwent a DRPPT from February 2016 to May 2017. Participants who had an IOP rise of >2 and <20 mm Hg during the DRPPT were recruited. Additional inclusion criteria were the visibility of at least three LCPs on the optic disc photographs taken at baseline of the DRPPT and shortly after its end, with the superior disc half and the inferior disc half each having at least one visible LCP. Exclusion criteria were any disorders of the optic nerve including glaucoma, fundus images too low in their quality for analysis and an age of <18 years.
DRPPT and examinations
The DRPPT has routinely been performed in the Beijing Tongren Hospital for the examination of individuals suspected to be prone to acute primary angle closure.9 17 The patients were asked to sit in a chair in a dark room for 2 hours and to rest their foreheads on a pillow placed on a desk. Shortly before the test and at 1 hour and at 2 hours after start of the test, the IOP was measured by non-contact tonometry (Topcon CT-60, Topcon, Tokyo, Japan). All tonometric measurements were performed three times and the mean value of the three measurements was taken for further statistical analysis. Shortly before start of the DRPPT and within 5 min after its end, we took swept-source optical coherent tomographic (OCT) images and conventional photographs of the optic disc and the macula (Topcon DRI OCT Triton, Topcon). The 45° photographic images were centred on the optic disc and on the macula. The head position of the study participants was checked before the image acquisition, and the tracking system of the OCT was applied to align the fundus photograph with the OCT scan. In addition, ocular biometry (optical low-coherence reflectometry; Lenstar 900 Optical Biometer, Haag-Streit, 3098 Koeniz, Switzerland) was carried out on the same day of the test, after the IOP had returned to normal values. Some eyes additionally underwent an OCT examination of the optic nerve head on the following day.
Image processing and measurements
The fundus photos of the optic disc taken at baseline and at the end of the DRPPT were superimposed on each other using a commercial imaging software (Adobe Photoshop, Adobe Systems, San Jose, California, USA). Applying the move tool and the arbitrary rotation tool, both optic disc images were colocalised with the major retinal vessels disc borders as reference structures and using a flicker method (figure 1A). Care was taken to primarily adjust the retinal vessels with each other and to secondarily align the disc borders with each other. It showed that for most eyes included into the study, the retinal vessels and the optic disc border moved parallel to each other, while the intrapapillary region including the central retinal vessel trunk and the LCPs moved in a disparate manner as compared with the disc border and extrapapillary retinal vessels. The contrast of the images was adjusted to optimise the recognition of the LCPs (figure 1B). The centre of LCPs was marked pair by pair on the photographs taken at baseline and on the images taken after DRPPT at a higher IOP. The dots representing the higher IOP status were extracted and superimposed on the images of the baseline examination, with the two reference points overlying each other (figure 1C).

Measurement of the lamina cribrosa movement in an eye with the intraocular pressure increased from 16 to 23 mm Hg induced by a dark room prone provocative test. Fundus photographs of an optic disc with visible lamina cribrosa pores (LCP) are shown in figure A-1 (taken at baseline) and figure A-2 (at the end of the test). figures B-1 and B-2 show the same lamina cribrosa with increased contrast. The centre of LCPs was marked in green on the photograph taken at baseline (figure C-1) and in blue on the photograph taken at the end of the test (figure C-2). After colocalisation of both images with the major retinal vessels and disc borders coinciding, the marks for LCPs were superimposed on each other; the distance between both markers of the same LCP was measured as the LCP moving distance (LCPMD) (figure D-2). The mean LCPMD within one eye was calculated as the mean value of the movement of the four visible LCPs located closest to the optic border, in the superior, inferior, nasal and temporal border, as shown in the dotted circles.
Four (or three if there were only three) visible LCPs located closest to the optic disc border in the superior, inferior, nasal and temporal quadrants were chosen for analysis. The LCP moving distance (LCPMD) of each pore was measured as the distance between its location at lower IOP and its location at higher IOP, using the image analysis software ImageJ (https://imagej.nih.gov/ij/) (figure 1D). The mean value of the movements of all LCPs per eye was defined as the mean LCPMD. The intralamina range and the intralamina SD of the LCPMD were defined as the difference between the largest LCPMD and the smallest LCPMD, and the SD of the LCPMD was calculated.
Since the area with visible LCPs varied among eyes and since this variation might have had an effect on the results, we measured the distance between the visible LCP located most superiorly and the visible LCP located most inferiorly, as the scope of measurements. Additionally, we measured the vertical diameter and horizontal diameter of Bruch’s membrane opening (BMO), the optic cup width and the cup depth as visualised on the OCT images, the maximum width of parapapillary beta zone and the degree of optic disc tilting. We defined the latter as the ratio of the horizontal disc diameter divided by the vertical disc diameter.9
The alignment of the images and the marking of the LCPs was performed by a single examiner (YXW). To evaluate the intraobserver and interobserver reproducibility of LCPMD, 10 eyes were randomly selected and re-evaluated by two independent observers (YXW and QZ) for all the steps from alignment to measurement.
Statistics
Statistical analysis was performed using a commercially available statistical software package (SPSS for Windows, V.25.0, IBM-SPSS, Chicago, Illinois, USA). The measurements were described as mean±SD. Associations between the LCP movements and other parameters such as age and the IOP rise were assessed first in a univariate analysis and then in a multivariable analysis. The multivariable analysis included those parameters as independent variables, which had a significant association with the LCP movement in the univariate analysis. In a step-by-step manner, we then dropped those variables out of the list of independent parameters which were no longer significantly associated with the main outcome parameter. The standardised regression coefficient beta, the non-standardised regression coefficient B and the 95% CIs were calculated. The intraobserver and interobserver agreement of the measurements on the mean LCPMD by eye were calculated by the intraclass correlation coefficient (ICC). The agreement was also assessed with mean differences (bias), 95% limits of agreement and using Bland-Altman plots. All p values were based on two-sided tests and were considered statistically significant if <0.05.
Results
Out of 101 eyes of 61 individuals suspect of acute primary angle closure (mean age: 54.8±9.3 years; range: 30–70 years) that were initially examined, 38 eyes from 27 participants (19 women) fulfilled the additional inclusion criteria that three LCPs were visible at both times. The mean age was 52.5±10.8 years (range: 30–67 years). The IOP increased from 16.7±3.2 mm Hg (11.7–24.0 mm Hg) at baseline to 23.9±4.3 mm Hg (18.3–34.3 mm Hg) at the end of DRPPT, with a mean elevation of 7.2±2.4 mm Hg (3.3–11.6 mm Hg). The horizontal and vertical BMO diameters, the horizontal and vertical optic cup width, the cup depth and the optic disc tilt was 1.76±0.18 mm (1.42–2.27 mm), 1.84±0.22 mm (1.48–2.59 mm), 0.97±0.24 mm (0.54–1.48 mm), 1.00±0.20 mm (0.65–1.62 mm), 0.55±0.22 (0.17, 0.99) and 0.90±0.08 (0.74–1.06), respectively. The mean axial length, anterior chamber depth and corneal thickness was 22.7±0.6 mm, 2.09±0.29 mm and 557±32 µm, respectively (table 1).
Characteristics of participants of the dark room prone provocative test (DRPPT) and basic measurements
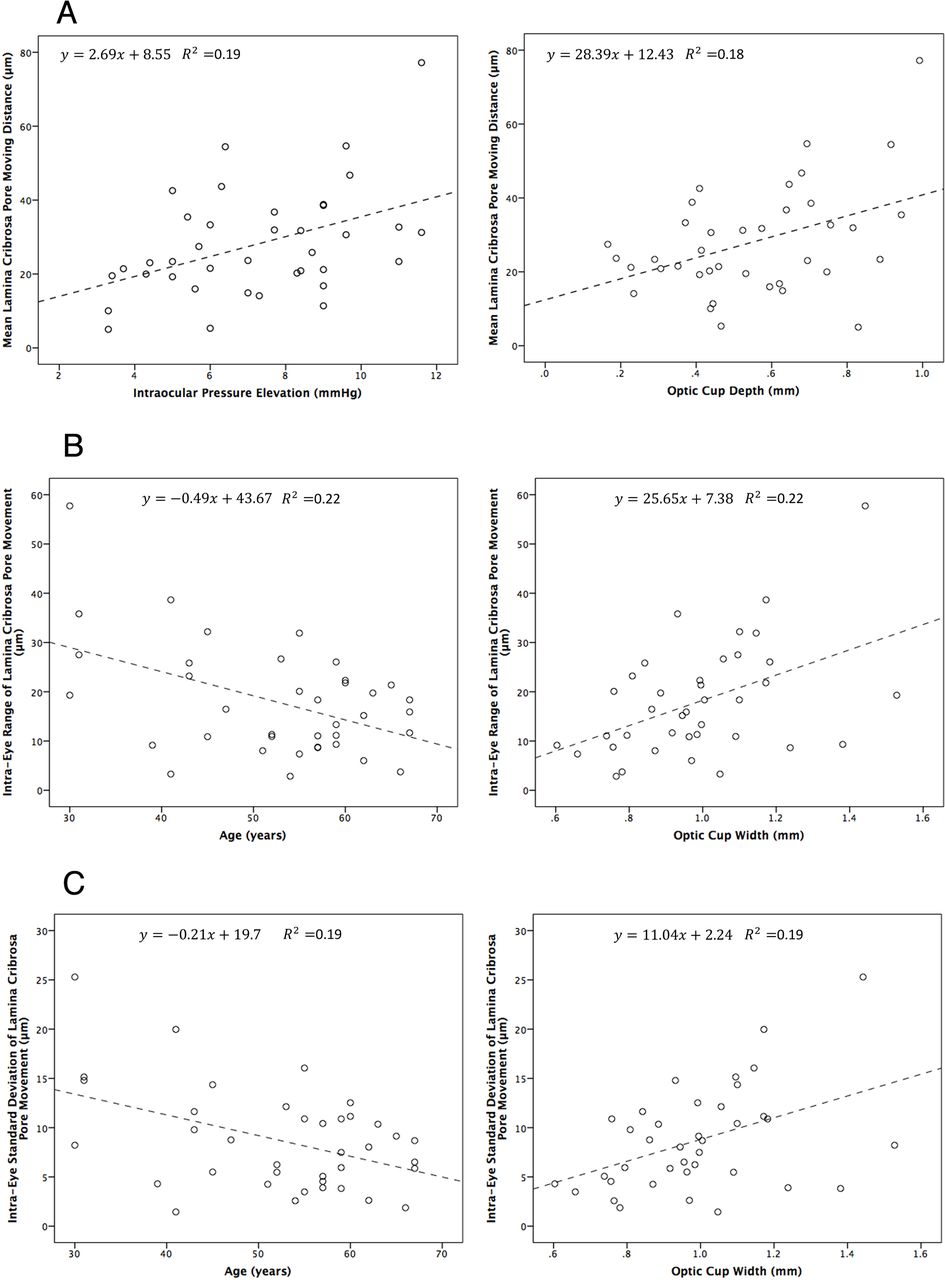
The mean LCPMD of the 38 eyes was 28.1±14.6 µm (5.0–77.2 µm). A larger LCPMD was associated with a higher rise in IOP (p=0.006) and a larger cup depth (p=0.008) (table 2, figure 2A). It was not significantly correlated with age, gender, IOP at baseline, axial length, anterior chamber depth, horizontal and vertical BMO diameter, cup diameter, disc tilting and the maximum width of parapapillary atrophy (table 2). In multivariate analysis, the LCPMD remained to be positively related with a higher rise in IOP (p=0.01) and a larger cup depth (p=0.02) (table 3).

Scatter plots showing the relationship of the mean lamina cribrosa pore moving distance (LCPMD) with the rise in intraocular pressure or the deepening of the optic cup depth (A); the intra-eye range of the LCPMD with age or optic cup width (B) and the intra-eye SD variation of the LCPMD with age or optic cup width (C).
Associations of the mean lamina cribrosa pore moving distance (LCPMD), the intralamina range and intralamina SD of LCPMD in a multivariate analysis
Associations of the mean lamina cribrosa pore moving distance (LCPMD), the intralamina range and intralamina SD of LCPMD in a univariate analysis
The intralamina range (17.9±11.3 µm) and SD (8.7±5.2 µm) of the LCPMD were significantly associated (multivariable analysis) with younger age (p=0.01 and p=0.02, respectively) and a larger cup width (p=0.01 and p=0.02, respectively) (table 3, figure 2B and C). They were not significantly correlated with the IOP rise (p>0.05).
The movements of the LCPs within each eye occurred parallel to each other into similar directions. The LCP movements were headed into the superior direction in 12 (33%) eyes, the inferior direction in 10 (28%) eyes, the temporal direction in 9 (25%) eyes and the nasal direction in 5 (14%) eyes.
If one eye per participant was chosen, the mean LCPMD was still related with the rise of IOP (p=0.040), however not with the cup depth (p=0.067). The same results were obtained for the intralamina range and intralamina SD of LCPMD (p=0.016 and p=0.023 for age; and p=0.006 and p=0.010 for optic cup width, respectively).
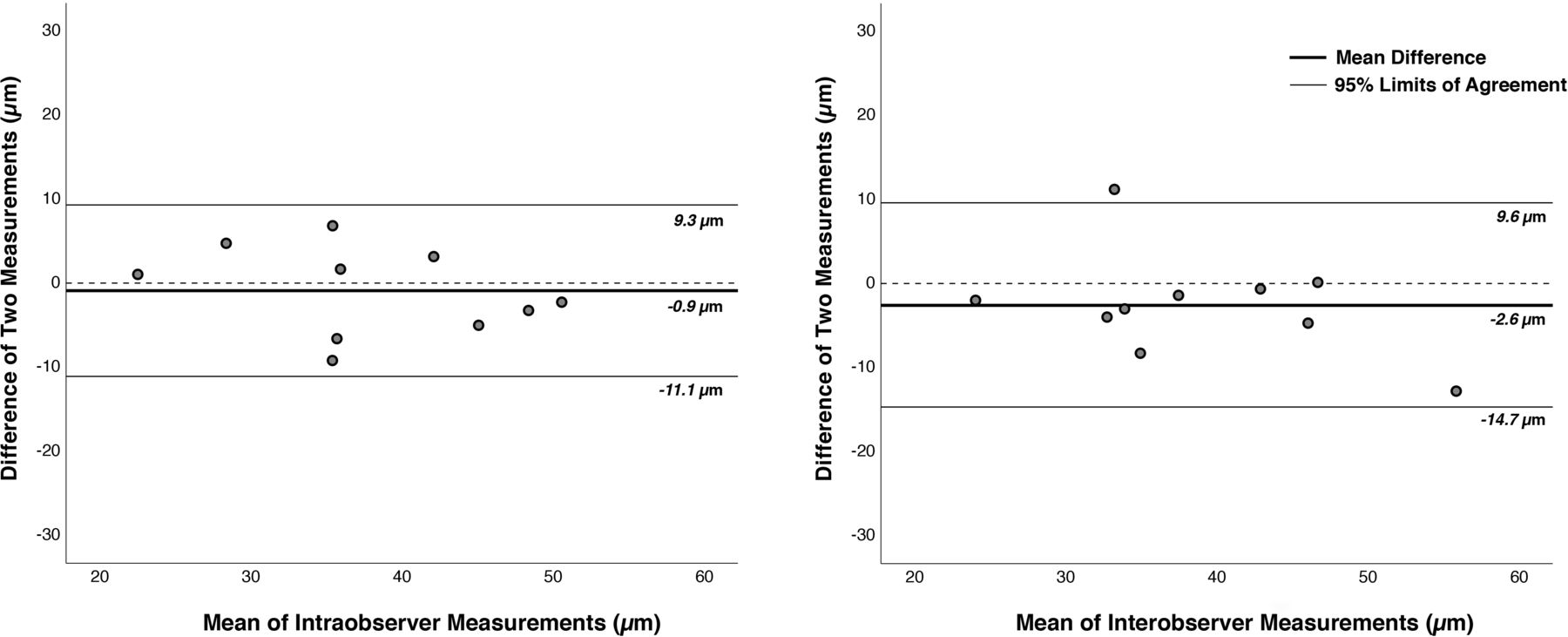
Using the criteria described by Fleiss, the mean LCPMD measured by two observers showed good intraobserver agreement (ICC=0.911; 95% CI 0.643 to 0.978; p=0.001) and interobserver reproducibility (ICC=0.884; 95% CI 0.533 to 0.971; p=0.002).18 The mean difference between the two measurements and the 95% limits of agreement was −0.9 (−11.1 to 9.3) µm and −2.6 (−14.7 to 9.6) µm, for the intraobserver reproducibility and interobserver reproducibility, respectively. It was presented in the Bland-Altman plots (figure 3).

{kind=link}
{kind=link}
{kind=link}
Bland-Altman plots of the intraobserver agreement (left) and interobserver agreement (right) on the measurement of the lamina cribrosa pore moving distance (LCPMD) in 10 random eyes. The mean difference between the two measurements and the 95% limits of agreement was −0.9 (−11.1 to 9.3) µm and −2.6 (−14.7 to 9.6) µm, for the intraobserver reproducibility and interobserver reproducibility, respectively.
Discussion
In this observational study with a dark room test-induced, almost natural, mild increase in IOP by 7.2±2.4 mm Hg (range: 3–12 mm Hg) in angle-closure suspects, we observed a shift of visible LCPs in the frontal plane. A larger LCPMD was associated with a higher IOP rise and a deeper optic cup. The variation in the LCPMD within the same optic disc was larger in younger participants and in eyes with a wider optic cup.
A movement of the lamina cribrosa and changes in the optic nerve head tissue compliance after a short-term rise in IOP has been examined in previous investigations.5–9 19 Experiments in monkeys showed that the lamina could deform anteriorly or posteriorly in response to an acute IOP rise, scleral canal expansion and contraction due to the interaction of the structural stiffness of the lamina cribrosa and sclera in normal eyes. There was also a scleral backward bowing in eyes with experimental glaucoma as compared with normal eyes.19 Yan et al reported on a posterior displacement of the lamina cribrosa in postmortem human eyes, with the biomechanical stress being highest in the periphery and lowest in the centre of the optic nerve head.7 In a clinical study on optic nerve head changes during an acute IOP rise, we observed a thinning mainly of the prelaminar tissue, while the lamina cribrosa showed morphological changes mostly with an IOP elevation by >15 mm Hg.9 Applying sonography, Pavlatos et al20 found that a posterior displacement of the sclera and optic nerve head was associated with the IOP in a non-linear manner. The current study suggested that the IOP rise-associated displacement in the lamina cribrosa may occur in the anterior-posterior direction (ie, thinning of the prelaminar tissue and backward bowing of the lamina cribrosa) and in the frontal plane leading to a lateral movement of the LCPs.
The connective tissue sheets of the lamina cribrosa are penetrated by 200–400 pores, through which the optic nerve fibre bundles and the retinal vessels pass.15 16 21 In a study on 87 glaucomatous eyes, Miller and Quigley reported that the size and shape of the LCPs changed with the severity of glaucoma.22 In eyes with early or moderate glaucoma, the shape of the LCPs was round to oval, while in eyes with advanced glaucoma, the LCPs tended to be slit-shaped. Tezel et al observed 39 glaucoma patients and found that during a period of 3 years the configuration of the LCPs changed in some eyes, while the overall LCP area and the ratio of total LCP area to optic disc area remained constant.23 In the population-based Blue Mountains Eye Study, Healey and Mitchell described that the detectability of the LCPs was higher in eyes with a higher cup/disc ratio, a larger optic disc diameter and a more hyperopic refractive error.24 Correspondingly, the LCPs could more frequently be detected in patients with open-angle glaucoma than in healthy individuals (70.8% vs 29.3%). Performing a three-dimensional reconstruction and segmentation of the lamina cribrosa beams, Reynaud et al found that the LCPs had a larger pore diameter, a larger volume and a larger connective tissue volume in normal monkeys than in monkeys with experimental glaucoma.25 In a longitudinal study, Ivers et al concluded that the increase in the LCP diameter was among the first structural changes in four of seven eyes with experimental glaucoma.26 In another study, the LCP was found to be more tortuous in 48 glaucoma eyes as compared with healthy eyes.27 All these studies highlighted the importance of the morphometry of the LCPs, however none of them focused on a lateral movement of the LCPs and of the lamina cribrosa.
The mechanisms have remained elusive by which IOP-induced changes lead to a damage of the retinal ganglion cell axons when passing through the lamina cribrosa. It has been discussed that the backward displacement of the lamina cribrosa was associated with the onset and progression of glaucomatous cupping.4 15 16 It has been reported that the permanent deformation and hypercompliance of the tissue at the optic nerve head surface and the lamina were manifestations of an early connective tissue damage.12–14 28 Studies on monkeys with an experimental IOP elevation showed that the onset of a fixed posterior deformation and hypercompliance of the optic nerve head surface developed within 4–8 weeks after onset of an IOP elevation. It was hypothesised that the damage to the connective tissues of the lamina and anterior scleral canal wall were responsible for these findings.28 In the current study, we observed a lateral movement of the LCPs and the amount of the LCP movement were associated with the height of the moderate rise in IOP. The observation of a lateral movement of the LCPs might have been a direct result from the in-plane stretch caused by the tensile force of the sclera driven by the IOP. Previous studies suggested that there were three types of strains that co-existed and which differed in their magnitude from the anterior region to the posterior region and from the peripheral region to the central region of the optic nerve head.29 Due to the technology applied in the present study, we could assess only the LCPs located in the superficial layer of the lamina cribrosa. If one assumes that the LCPs in the deep lamina cribrosa layers may undergo a lateral shift different from the lateral shift in the superficial lamina cribrosa layer, a shearing force may develop between the lamina cribrosa layers. This shearing force may potentially play a role in the process of glaucomatous damage to the optic nerve fibres within the lamina cribrosa. Future studies may aim to examine the different layers of the lamina cribrosa in their response to an acute moderate IOP rise.
In the present study, we found that the variability in the LCP movements within the optic disc decreased with older age after adjusting for the amount of the IOP rise. It agrees with a decrease in the compliance of the lamina cribrosa with older age.12 Correspondingly, population-based investigations and hospital-based studies have shown that older age was a major risk factor for the development and progression of glaucomatous optic nerve damage.30 31 Morrison et al found an increased collagen deposition and thickening of astrocyte basement membranes in the lamina cribrosa of older individuals.32 Albon et al showed that the lamina cribrosa had less elastin and was stiffer and less resilient to pressure with ageing.33 Examining 64 donor eyes, Girkin et al found a significant deepening of the lamina cribrosa with older age in individuals of African ethnicity.34
Previous studies showed that the size of the optic cup was a risk factor for the development and progression of glaucoma.35 36 Fan et al found that single nucleotide polymorphisms (rs1063192 and rs10483727) were both associated with a larger optic cup and with the prevalence of open-angle glaucoma.37 In our study, the IOP rise-associated movement of the LCPs and its regional variability within the same optic disc were associated with a deeper and wider optic cup. The three-dimensional morphology of the optic cup might play a role in the biomechanical behaviour of the posterior eye. Future studies may thus address whether a larger, IOP rise-induced LCP movement is associated with higher glaucoma susceptibility. If that is the case, one may discuss that the movement of the LCPs in the frontal plane may pathogenetically be correlated with the glaucoma-induced damage to the retinal ganglion cell axons when passing through the lamina cribrosa.
Limitations of our study should be discussed. First, we used fundus photographs so that the assessment of the LCPs occurred in a two-dimensional manner. A three-dimensional aspect in the LCP movement, such as in association with a backward bowing of the lamina cribrosa, could thus not be examined. Although we also took OCT images of the lamina cribrosa at baseline and at the height of IOP elevation, we were not able to clearly re-identify the same LCPs on the image taken at baseline and on the image taken 2 hours later. The IOP rise-induced changes in the lamina cribrosa occurred in a three-dimensional manner so that, due to the backward bowing and rotation of the lamina cribrosa, the plane at which the LCP were visualised changed.9 17 A future study may focus on the three-dimensional reconstruction of the lamina cribrosa architecture based on serial OCT images and it may allow precisely re-locating the LCPs. It may give additional hints towards an IOP rise-associated LCP movements. Second, the ophthalmoscopical visibility of the LCPs had a strong influence on their selection to be assessed and included into the study. It might have led to a profound selection bias. To cite examples, the visibility of the LCPs clearly depended on the disc size since small discs without cups have no visible LCPs. In a similar manner, the LCP visibility may be better in large discs with a medium-sized optic cup than in medium-sized discs with a small cup. The disc size, among other parameters, may thus have had a major influence on the inclusion of LCPs into the study, and this disc size-dependent influence might have caused a bias in the study results. Future studies may investigate the LCP movements in dependence of other parameters by employing OCT-based three-dimensional re-constructions of the lamina cribrosa. Third, we measured the LCPMD on two-dimensional fundus photographs. Although this technique has been shown having a reasonable intraobserver reproducibility and interobserver reproducibility, inaccuracies during the subjective and arbitrary superimposition and colocalisation of the images might have occurred. Fourth, we studied only the superficial aspect of the LCP and did not obtain information on IOP rise-associated changes in the deeper layer of the lamina cribrosa. Fourth, parallel to the aforementioned limitations, the study included only eyes with visible LCPs so that this preselection of the eyes included into the study prevents a generalisation of the findings.
In conclusion, eyes experiencing a mild-to-moderate IOP rise for 2 hours showed a lateral movement of their LCPs. A larger LCPMD was associated with a higher IOP rise and a deeper optic cup. The intralamina variability of the IOP rise-associated LCP movements decreased with older age and increased with a wider optic cup. The findings may be of interest to elucidate the biomechanical properties of the lamina cribrosa and open the question whether a lateral movement of the LCPs in the frontal plane may be associated with the glaucomatous damage of the optic nerve fibres.
References
Footnotes
Correction notice The paper has been slightly amended since it was published Online First. There were a couple of typographic errors which have since been corrected.
Contributors YXW: design, concept, analysis, writing. QZ: application, data collection, analysis. HY: analysis. JDC: patient examination, data collection. NW: patient examination. JBJ: design, writing.
Funding National Natural Science Foundation of China #81570835.
Competing interests None declared.
Ethics approval The Ethical Review Committee of Beijing Tongren Hospital approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request.
Linked Articles
- At a glance