Article Text

Abstract
Background To identify and analyse the character and relationship between flat irregular pigment epithelial detachment feature (FIPED), choroidal thickness and choroidal neovascularisation (CNV) network seen on optical coherence tomography angiography (OCTA) in eyes with central serous chorioretinopathy (CSCR) in Chinese patients.
Method In the present study, 152 eyes of 144 Chinese patients, who were previously diagnosed with CSCR, were retrospectively studied. Patients’ baseline characteristics, the course of CSCR, best-corrected visual acuity, the pattern of CNV on OCTA, FIPED and choroidal thickness detected by enhanced depth imaging-OCT (EDI-OCT) were analysed.
Results It was disclosed that 7.23% of CSCR patients had CNV. Age and the course of CSCR were found to be correlated with the occurrence of CNV. Among the eyes with CNV network (11 eyes), 100% of them had FIPED, whereas, among the eyes without CNV (141 eyes), 18.04% had FIPED. The maximum width and en-face area of PED were greater in the CNV group compared with that in the non-CNV group (p<0.001). It also was revealed that female gender and a poor vision were risk factors for CNV in eyes with CSCR. The choroidal thickness detected by EDI-OCT was also statistically significant between eyes with CNV and eyes without CNV. The patients who have CNV complicated with FIPED are susceptible to have low vision.
Conclusion The present research demonstrated that the majority of CNV cases were linked to FIPED, and the thinner thickness of choroid. The greater width and en-face area of PED may point towards the presence of an underlying CNV network.
- retina
- imaging
- diagnostic tests/investigation
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Central serous chorioretinopathy (CSCR) is a disease in which a serous detachment of the neurosensory retina occurs over an area of leakage from the choriocapillaris through the retinal pigment epithelium (RPE). It is a self-limited macular disease marked by distortion, blurry vision and metamorphopsia. Other causes for RPE leaks, such as choroidal neovascularisation (CNV), inflammation or tumours, should be ruled out to make the diagnosis. CNV is also an uncommon complication of CSCR.
Previous studies reported that CNV is a major cause of vision loss in CSCR,1–3 because it is often difficult to clearly demarcate the presence of a CNV in the setting of chronic CSCR. Recently, by using more sensitive clinical detection instruments, such as optical coherence tomography angiography (OCTA) instruments, CNVs were found in the chronic CSCR cases,4 and those cases are mainly prone to severe visual debility. However, the diagnosis of CNV complicating chronic CSCR is still a serious challenge. Thus, increasing the detection rate of CNV and seeking the factors associated with CSCR accompany with CNV are important for diagnosis and treatment of CSCR.
Occult CNVs are often described as either fibrovascular pigment epithelial detachment (PED) or late leakage of undetermined source.5 The changed shape of PED is variable and correlated with the degree of acute or chronic disease. A typical dome-shaped PED correlates with acute CSCR, while flat irregular PED (FIPED) is more likely observed in chronic CSCR.4 6–8 Several studies assessed the presence of CNV in CSCR with variable and non-comparable results,4 9–11 due to different definitions of ‘flat’ or ‘shallow’ irregular PED. Thus, the characteristics of PED, such as area, width, height of PED and choroidal thickness,12 13 were involved in the present study to analyse the relationship between PED and CNV.
In addition, OCTA is a new non-invasive modality for analysing the retinal and choroidal vasculatures with the help of decorrelation of signal amplitudes obtained from repeated B-scans from the same site to detect non-static structures, such as blood in vessels against a static background.14 Numerous research has concentrated on the proportion of CNV in CSCR using OCTA worldwide,4 11 14–16 while a limited number of relevant studies have conducted in China. In the present study, we attempted to identify and analyse the characteristics of these CNVs in Chinese cases with CSCR using OCTA to evaluate correlation with the formation of these FIPED.
Methods and materials
Patients
A multicentric, retrospective, observational study was carried out on 152 eyes of 144 patients who were previously diagnosed as CSCR at Shandong Eye Hospital and Shandong Eye Institute, Shandong First Medical University and Shandong Academy of Medical School, between February 2017 and November 2018.Patients diagnosed with CSCR was based on the presence of idiopathic serous macular detachment associated with choroidal thickening (detected with OCT), and RPE focal leakage and choroidal vascular hyperpermeability (detected with fluorescein angiography (FA) and indocyanine green (ICG) angiography, respectively). We excluded patients without a documented history of CSC by FA that was related to early manifestations of the disease. We also excluded patients with other chorioretinal disorders that can cause macular exudation, such as drusen, pathologic myopia, intraocular inflammation, retinal vasculopathies, angioid streaks, trauma and hereditary dystrophies.17 The presence/absence of CNV was determined using clinical evaluations, OCT imaging and angiographic findings. For CNV, identified to have FIPED on spectral domain OCT (SD-OCT) B-scans, and CNV signs on multimodal imaging including SD-OCT, OCTA and dye angiography with FA and ICG.18
Eyes were diagnosed with non-neovascular CSCR if they exhibited SRF and focal or multiple serous PEDs without CNV. Eyes were diagnosed with neovascular CSCR if CNV associated with CSCR was present, as primarily indicated by OCTA findings. Patients that had age-related macular degeneration, pathologic myopia, idiopathic CNV, diabetic retinopathy and angioid streaks were excluded from the study.
OCTA parameters
Herein, OCTA was performed using AngioVue (Optovue, Fremont, California, USA). The eyes were analysed by using OCTA to indicate the presence of any CNV network in the outer retina or inner choroid. Various OCTA parameters were analysed, such as height of the neurosensory retinal detachment, and presence of double-layer sign (defined as PED with hyper-reflective content inner to an intact hyper-reflective Bruch membrane).19
Definitions
A scar on OCTA was defined as a hyper-reflective tissue accompanied by retinal atrophy. Double-layer sign was defined as irregular shallow PEDs with hyper-reflective or hypo-reflective content inner to an intact hyper-reflective bruch membrane.
Grouping
The eyes were classified into two groups depending on the presence or absence of CNV network on OCTA. Age, gender, course of disease, vision, characteristics of FIPED and choroidal thickness were analysed.
Statistical analysis
Data were statistically analysed by using SPSS V.10.0 software (SPSS). X2 or Fisher’s exact test was used for analysis of categorical variables. T-test was used for analysis of continuous variables. Binary-logistic regression analysis was used to explore factors influencing CNV. P<0.05 was considered statistically significant.
Results
Characteristics of CSCR patients with and without CNV
A total of 152 eyes of 144 patients (88 males and 56 females) who met the inclusion criteria were included (online supplementary file 1). The age of these 144 patients ranged from 26 to 77 years (mean age, 51±8.86 years). A total of 11 (7.23%) eyes (9 males and 3 females) had a CNV network. In the total patients, 32 cases (22.2%) were chronic CSCR cases, which was defined as persistence of serous retinal detachment for at least 6 months or widespread RPE decompensation with or without serous retinal detachment, which may or may not be associated with active leakage sites.18 20 These patients with chronic CSC with CNV have more severe visual impairment than these without CNV (p=0.002, table 1). There was a strong correlation between age and CNV occurrence (p<0.001, table 1). The cases with CNV had older age and longer disease course (p<0.01, table 1). The average duration of CSCR with CNV was 13.6±18.46 months, which is longer than these without CNV. However, no correlation between gender and CNV incidence was observed (p=0.239, table 1). Thus, age and the course of disease are risk factors for occurrence of CNV.
Supplemental material
Clinical characteristics and OCTA detection of patients with CSCR with and without CNV
Imaging features of CSCR patients with and without CNV
The eyes of patients with CNV had a significantly lower vision than those cases without CNV. Besides, 23.02% of CSCR cases had FIPED. In addition, all the patients with CNV had FIPED, while 18.04% of patients without CNV had flat irregular PED. The en-face area or width of flat PED of patients with CNV was notably different from patients without CNV (p<0.05 and p<0.001, table 1). The mean value width and en-face area in patients with CNV were greater than that in patients without CNV (table 1). However, the height of FIPED was not remarkably different between patients with CNV and patients without CNV (table 1). Representative eyes with and without CNV are shown in figures 1 and 2.

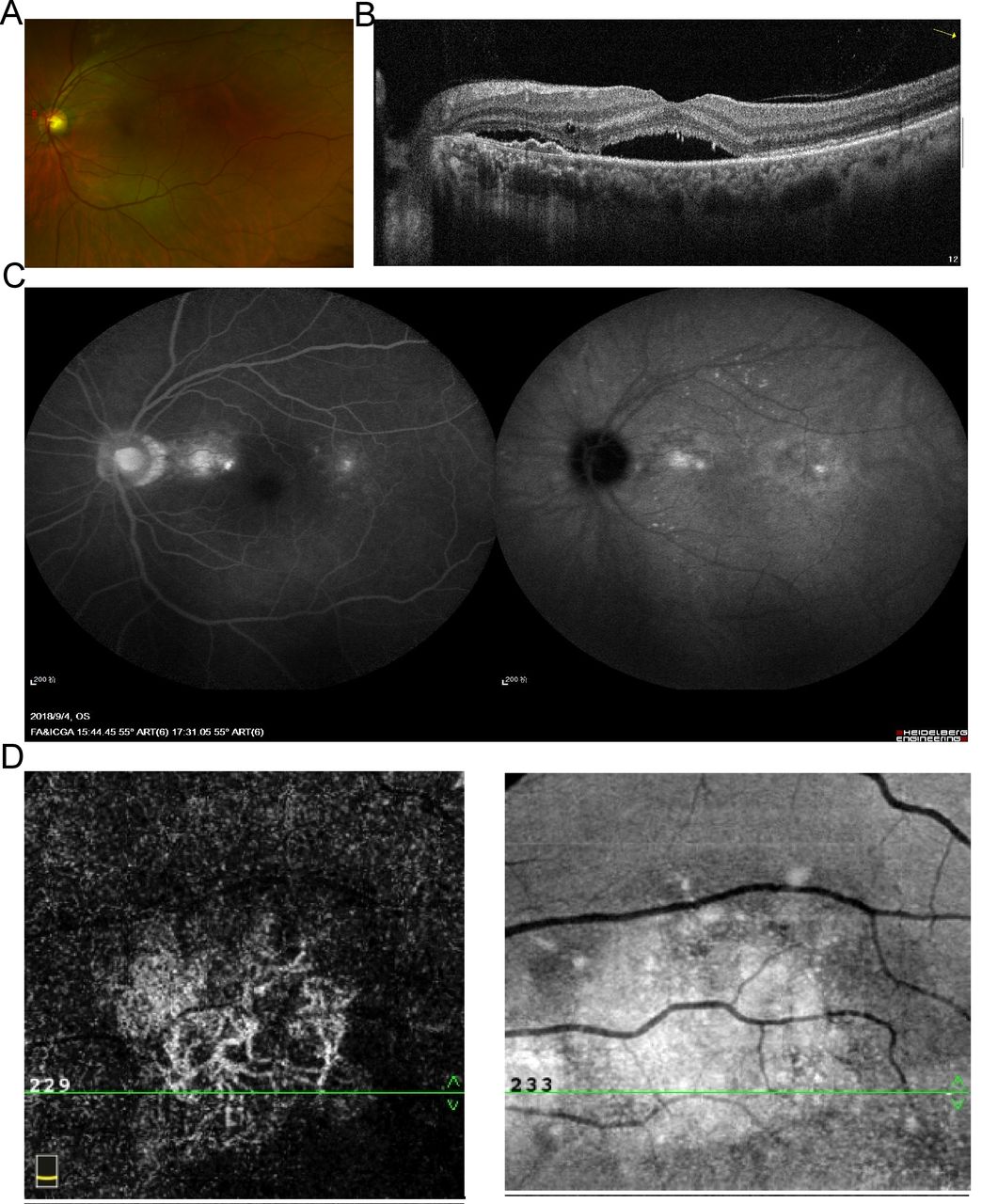
Multimodal imaging of a case with flat irregular PED with choroidal neovascularisation. (A) Confocal laser scanning microcopy demonstrates serous retinal neuroepithelial detachment in macular region. (B) Horizontal B-scan through the macula showing the serous retinal detachment and a small flat irregular PED. (C) Early and late indocyanine green angiography show the presence of two small areas of hyperfluorescence. (D) OCTA C-scan above the RPE (30 µm) to show thatwell circumscribed, with a clear hyperintense signal and finely vessels inside the lesion at the outer retina. OCTA, optical coherence tomography angiography; PED, pigment epithelial detachment; RPE, retinal pigment epithelium.

{kind=link}
{kind=link}
Multimodal imaging of a case with flat irregular PED and no choroidal neovascularisation. (A) Confocal laser scanning microscopy illustrates serous retinal neuroepithelial detachment in macular region. (B) OCTA B-scan showing the serous retinal detachment and a small flat irregular PED (C) early and late indocyanine green angiography show the presence of two small areas of hyperfluorescence featuring late leakage. (D) OCTA at outer retina and choriocapillaris illustrate no significant signal in vessels. OCTA, optical coherence tomography angiography; PED, pigment epithelial detachment.
Choroidal thickness was significantly different between eyes without CNV and eyes with CNV (table 1). The choroidal thickness in eyes with CNV was thinner than those without CNV (table 1).
Characteristics of patients with FIPED
All patients with CNV had FIPED. 31.5% of eyes with FIPED had CNV. These patients with FIPED were older than those without PED, and had longer disease course than those without FIPED (table 2). The individuals’ vision loss with FIPED was more severe than those without FIPED (table 2, best-corrected visual acuity: (0.8±0.09) and (0.5±0.23). However, patients without FIPED had thicker choroidal thickness detected by enhanced depth imaging (EDI)-OCT compared with those with FIPED. All chronic CSCR cases have FIPED. Although three acute CSCR cases have FIPED, they usually have a course of more than 2 months, without pigment epithelium damage. It is might be correlated with the gradually change from plateau to FIPED. Other features were not significantly different between the eyes with FIPED and those without FIPED (table 2).
Comparing characteristics of patients with or without FIPED
Characteristics of patients with thicker choroidal thickness
According previous report, the choroidal thickness in normal eyes detected by EDI-OCT was (256.8±75.8) μm,21 and the thicker choroidal in eyes with active CSCR was 338.05±31.42 µm.21 So the characteristics of patients with relatively thick choroidal (the thickness of choroidal >300 µm) and relatively thin choroidal (the thickness of choroidal <250 µm) were analysed. The patients with relatively normal or thinning choroidal were older than those who had thick choroidal, and their vision loss was markedly severed than those with thick choroidal (table 3). Additionally, 52.5% of patients with relatively thin choroidal had FIPED, which is more than these with thick choroidal (table 3). Furthermore, there was no significant difference in the en-face area, width and height of FIPED between eyes with thinning choroidal and thick choroidal (p>0.05; table 3). Almost chronic CSCR cases have thinner choroidal, compared with acute CSCR cases.
Comparing the characteristics of patients with or without thick choroidal
Comparing the characteristics of patients with thinning of choroidal between eyes with CNV or without CNV, age, gender and the course of disease showed that there were no statistically significant differences (table 4). The eyes with CNV and thinning choroid had significantly higher rate of vision loss compared with eyes without CNV (table 4). The en-face area of FIPED in eyes with CNV was notably different from the en-face area of FIPED in eyes without CNV (table 4). However, no significant difference was noted in choroidal thickness between eyes with CNV and eyes without CNV (table 4).
Comparing characteristics of patients with relatively thin choroidal between eyes with CNV or without CNV
Discussion
The application of OCTA is extremely beneficial for neovascularisation detection using clinical and imaging findings being further consistent with long-standing CSCR. CNV in the setting of chronic CSCR is relatively infrequent.22–24 With the advent of OCTA, an increased incidence of CNV has been reported in chronic CSCR.4 9 25 In the present study, we found that 7.23% of CSCR patients had CNV. With the help of OCTA, 34.4% of cases with chronic CSCR were found to have CNV. The cases with CNV had longer disease course than these with no CNV. Female gender and a poor vision were risk factors for CNV in eyes with CSCR. Visual prognosis is completely different between acute and chronic CSCR. Chronic CSCR are more likely to be poor visual prognosis. CNV as a complication of chronic CSC is correlated with a decreased visual acuity of chronic CSC. That might because the widespread RPE alterations or photoreceptor damage in chronic CSC lead to poor vision. CNV are more frequent in older people, with thinner choroid and FIPED. This is probably mainly because CNV complicated chronic CSC with widespread RPE damages.
The incidence and characteristics of patients with CNV in CSCR cases have not been well described. A recent study demonstrated that long-standing CSCR was shown to be associated with type 1 neovascularisation,26 which is consistent with the present study. It is of great importance to realise that an abnormal choroidal vascular pattern is not always associated with CNV. During study of the characteristics of FIPEDs, we found that FIPED correlated with the long course of disease. Moreover, FIPED correlated with impairment of vision. These results indicated that CNV with FIPED is correlated with the severity of the disease, which is in agreement with a previous research.19 Additionally, the en-face area and width of FIPED in CNV were significantly different from those cases without CNV, indicating that the en-face area and width of FIPED might be helpful for diagnosing FIPED and CNV.
Pachychoroid pigment epitheliopathy (PPE) is a newly presented clinical entity characterised by a range of RPE abnormalities, overlying the areas of choroidal thickening. A number of scholars reported that PPE could reside within a wide range of diseases (eg, CSCR). Three similar cases of type 1 neovascularisation associated with choroidal thickening were reported, and were named ‘pachychoroid neovasculopathy’.27 All three patients did not have any evidence of antecedent acute or chronic CSCR. A recent study revealed that changes of choroidal thickness in the fovea or parafovea were independent of age.28 Elevated choroidal thickness was associated with a risk of developing circumscribed choroidal hemangioma, as well as CSCR in patients with different ages.28 The present research showed that the majority of CNV cases were linked to thinner thickness of choroid, and the thicker choroid was associated with non-CNV cases. It may be caused by increased or decreased depth of OCT signal penetration due to such factors, involving RPE abnormalities or artefacts associated with overlapping superficial retinal vessels. Manual adjustment of the segmentation level often improves visualisation and removes several artefacts. A case with thinner choroid and CNV was found to be significantly different in vision loss and the positive percentage of FIPED compared with cases with thinner choroid and non-CNV. Daruich et al demonstrated increased choroidal thickness as a factor, influencing episode duration in acute CSCR,29 indicating that a thicker choroid is a predictor of the worse course of the disease. However, a relatively thin or slightly thicker is associated with CNV and FIPED. Hence, there may be a dynamic change in choroidal thickness during the process of acute to chronic exacerbation of the disease. However, further researches with a larger sample size are required to confirm the above-mentioned findings.
Conclusion
The majority of CNV cases were linked to FIPED, and the thinner thickness of choroid, especially, the width and en-face area of FIPED may point towards the presence of an underlying CNV network. Further studies are required to evaluate the follow-up and prognosis of these patients in order to better understand diagnosis of CSCR with CNV.
References
Footnotes
TL and WL contributed equally.
Contributors Study conception and design: TL and WL. Data collection and Data analysis: TL, WL and SZ. First article draft and article review: TL and WL.
Funding This work was supported by grants from the Natural Science Foundation of China (No.81500710) and the projects of medical and health technology development programme in Shandong province (No. 2016WS0526); Shandong Key Research and Development Project (2016 GSF 201088, 2019GSF108189); Shandong Province TCM Science and Technology Development Plan Project (2015-150); Shandong Medical and Health Science and Technology Development Plan (2015BJYB28).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The Human Research and Ethics Committee of Shandong Eye Hospital, Shandong Eye Institute, Shandong First Medical University and Shandong Academy of Medical School (2019-G-012) granted ethical approval for the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Patients were previously diagnosed at Shandong Eye Hospital and Shandong Eye Institute, Shandong First Medical University and Shandong Academy of Medical School, Data about patients are available on reasonable request.
Linked Articles
- At a glance