Article Text

Abstract
Background/Aims Charles Bonnet syndrome (CBS) is a complication of sight loss affecting all ages; yet, few childhood cases have been reported. Our aim is to raise awareness of this under-reported association occurring in children and young adults in order to prevent psychological harm in this age group.
Methods A retrospective case series reviewing medical notes of patients <25 years of age with sight loss and reported CBS at a single centre hospital eye service in London, United Kingdom. Search of electronic patient records identified 13 patients experiencing hallucinatory events over a 9-year period. Outcomes were patient demographics including ocular diagnosis, visual acuity at time of onset, characteristics of hallucinations, clinical management strategies and patient-reported affliction.
Results Eight patients were diagnosed with progressive inherited retinal diseases, primarily Stargardt disease (N=5). Clinical history indicated patients had significantly reduced best-corrected visual acuity (BCVA) in at least one eye at onset; median (IQR) worse eye BCVA was 1.0 (0.86–1.6) logarithm of minimum angle of resolution(LogMAR). CBS significantly affected patients’ personal lives including education, diet and sleep. Clinical management was varied, mostly relating to reassurance at the point of contact.
Conclusion We describe the clinical features of young patients with CBS, with management strategies and aspects of negative outcomes. High potential caseload and risk of psychological harm merit further research. Increased awareness among healthcare professionals and patient education to forewarn susceptible individuals may reduce the overall impact and improve coping with symptoms.
- Child health (paediatrics)
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Charles Bonnet syndrome (CBS) is characterised by the subjective experience of visual hallucinations secondary to sight loss. Hallucinations are often associated with sudden or progressive loss of vision, with no psychiatric or cognitive basis.1 Studies of cortical function suggest that changes in the visual cortex may have a role in the onset of visual hallucinations.2 A common theory for the genesis of CBS relates to ‘deafferentation’, whereby reduced visual input due to systemic or retinal dysfunction results in spontaneous hyperexcitability and disinhibition of the visual cortex, producing hallucinatory experiences.3 4 However, the precise pathophysiology of CBS remains poorly understood. Visual hallucinations in CBS are diverse and may manifest in a number of ways, including scenes of landscapes or moving patterns, small figures, distorted faces and delayed palinopsia.5 Symptoms of CBS may persist for several years6 and can have a significant impact on an individual’s quality of life.7
The prevalence of CBS is estimated to be in the range of 11–15% of adults with visual impairment8 and is typically associated with elderly patients, likely because age is a risk factor for a number of sight-threatening eye diseases including age-related macular degeneration and glaucoma. Yet, the causal theories suggest that CBS can affect individuals with visual loss at any age, inclusive of children.9 Indeed, a small number of case reports have described young patients experiencing CBS.10 11 This may reflect the lack of awareness among healthcare professionals or a difficulty in diagnosis, for example, CBS may be investigated as schizophrenia/schizoaffective disorder, migraines, seizures or tumours.12 13 Moreover, diagnosis of CBS can be confused with childhood imaginings, and children may have difficulties describing symptoms.9 Consequently, ascertainment of CBS in paediatric patients remains low and seldom discussed in the context of a routine clinical eye consultation. The purpose of this report is to expand on the associated clinical background and evidence of CBS in paediatric and young persons through a retrospective case series identified at Moorfields Eye Hospital NHS Foundation Trust.
MATERIALS AND METHODS
The study adhered to the tenets set out in the Declaration of Helsinki and was approved by the London—Camden & Kings Cross Research Ethics Committee (12/LO/0141). Using a search engine of electronic patient records with no date restriction, we filtered the keywords ‘Charles Bonnet’ and ‘visual hallucinations’ and set an age limit of under 25 years old. This search strategy was designed to flag patients where a description of suspected CBS symptoms had been reported. OpenEyes (Across Health, Ghent, Belgium) electronic database and the patient’s medical notes were used to retrieve data on demographics and clinical features. Records were reviewed for the following information: sex, ethnicity, age, principal diagnosis, genetic result if relevant and best-corrected visual acuity (BCVA) at time of hallucination onset. Details of CBS descriptors, the reporting healthcare professional and subsequent management of symptoms were included where available. BCVA was reported using LogMAR, where higher scores are indicative of poorer vision. Where very low vision was recorded (hand motion (HM) and perception of light (PL)), LogMAR numerical values were imputed in line with recognised conversion methods;14 for this study, HM and PL were valued as 2.3 and 2.7 LogMAR, respectively.
RESULTS
This retrospective study identified 13 patients who had attended Moorfields Eye Hospital between March 2011 and January 2020. The medical case notes were reviewed to reveal the demographics of these patients summarised in table 1. Men accounted for 9 of the 13 patients (69.2%). Median (IQR) age of CBS onset was 11 (9–19) years. Most patients had significantly reduced visual acuity at onset, median (IQR) better and worse eye BCVA was 0.81 (0.53–0.96) LogMAR and 1.0 (0.86–1.6) LogMAR, respectively. At the time of analysis, six patients were registered as sight-impaired or severely sight-impaired.
Patient demographics, clinical features and genetic details
The majority of patients (61.5%, n=8) were diagnosed with an inherited retinal disease (IRD), the most common being Stargardt disease (STGD) with five molecularly confirmed ABCA4-affected individuals. STGD is one of the most common macular dystrophies presenting in childhood, with a prevalence of ~1:8000–10 000.15 Patients present with progressive central vision loss with reduced visual acuity, dyschromatopsia and reduced contrast sensitivity (figure 1 A,B). One patient (ID: 13) had a rare form of Leber congenital amaurosis caused by TULP1 variants, presenting with profound visual deficits including nyctalopia, peripheral visual field loss and nystagmus, followed by cone dysfunction resulting in reduced central vision and dyschromatopsia. One patient (ID: 9) had non-syndromic retinitis pigmentosa caused by USH2A variants, where the patient initially experienced nyctalopia, followed by peripheral visual field loss but has preserved central vision (figure 1 C,D). There was one syndromic IRD case (ID: 4) of CLN3-related juvenile neuronal ceroid lipofuscinosis (also known as Batten disease, figure 1 E,F). This is a neurodegenerative disorder where the first sign is of a maculopathy resulting in a rapidly progressive deterioration in central vision between the ages of 4 and 10, leading to legal blindness within 3 years of onset. Later signs are progressive mental deterioration, loss of speech, epileptic seizures and premature death. Three patients had congenital eye disorders including microphthalmia and ocular coloboma (ID: 3), orbital anomaly with phthisis bulbi (ID: 7) and vitreoretinal dysplasia with persistent hyperplastic primary vitreous, anterior segment dysgenesis and primary congenital aphakia (ID: 1). These are non-progressive; however, case ID: 1 developed secondary glaucoma following bilateral retinal detachment surgery which would have further impacted on existing poor vision. One patient (ID: 08) had a spontaneous intracranial haemorrhage of unknown cause resulting in subsequent bilateral optic atrophy with large central scotomas. One patient (ID: 2) had a hereditary optic neuropathy, molecularly unsolved, with very poor residual vision with PL. Altogether, these varied inherited sight loss conditions display different patterns of vision loss, suggesting no clear correlation with CBS, except that clinicians caring for such children must be aware of this association.

{kind=link}
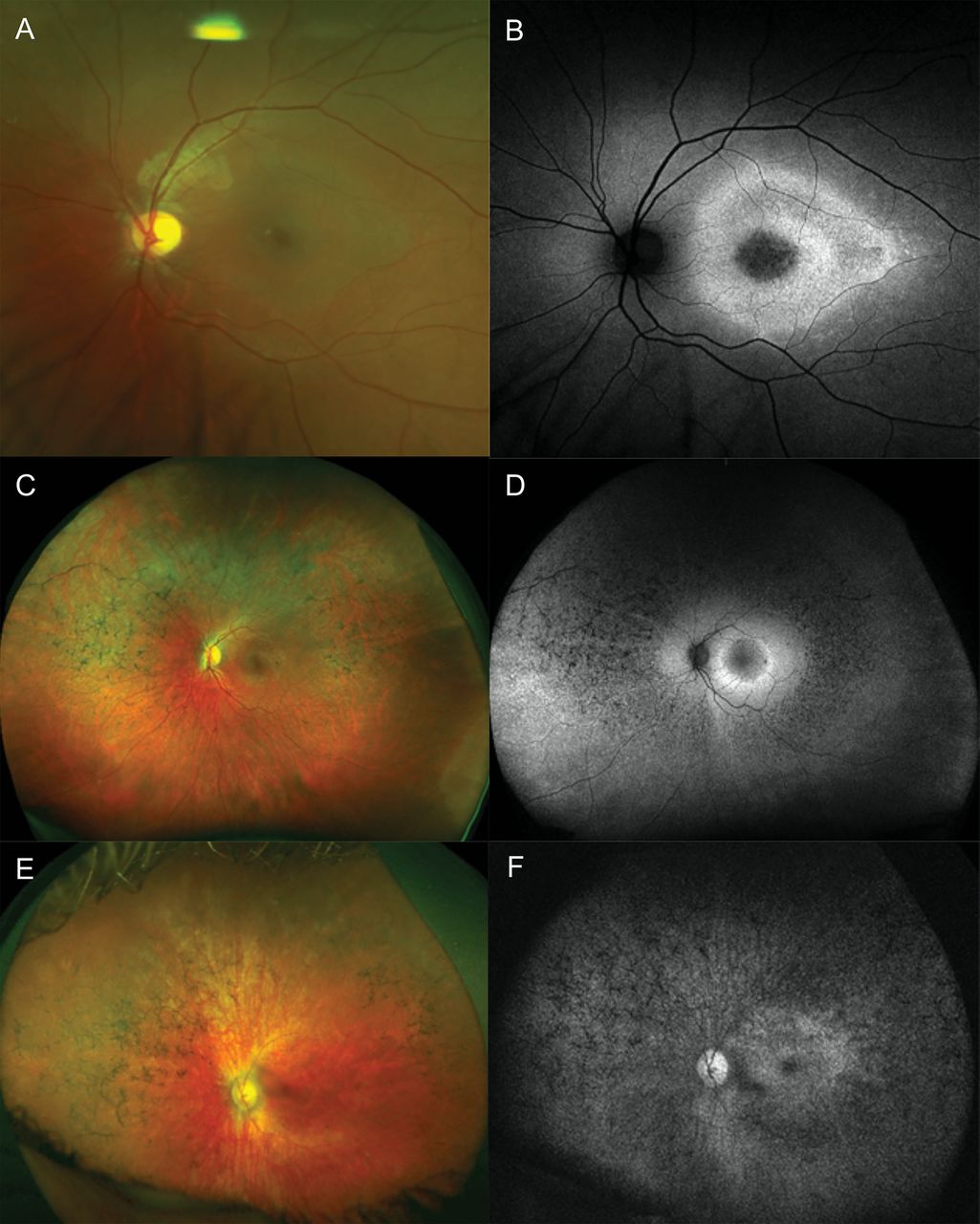
Fundus imaging of the left eye only of inherited retinal dystrophy cases experiencing Charles Bonnet syndrome. (A) Colour fundus image of patient ID: 11 (aged 11 years) with Stargardt disease caused by ABCA4 with minimal flecks and subtle macula atrophic changes and corresponding (B) fundus autofluorescence image showing hypofluorescence at the central macula with a ring of hyperautofluorescence within the arcades indicating the expanding area of retinal pigment epithelium (RPE) disease. (C) Ultra-widefield (UWF) colour fundus image of patient ID: 09 (aged 23 years) with non-syndromic retinitis pigmentosa caused by USH2A showing bone spicule retinal pigmentation in the mid-periphery, retinal vessel attenuation and some areas of depigmentation in the inferior retina, with corresponding (D) UWF fundus autofluorescence showing hyperautofluorescent ring at the macula with spots of hypoautofluorescence corresponding to RPE atrophy outside the arcades and in the mid-periphery. (E) UWF colour fundus image of patient ID: 04 (aged 14 years) with juvenile neuronal ceroid lipofuscinosis caused by CLN3 showing atrophic RPE changes with bone spicule pigment deposition in the mid-periphery, optic disc pallor and retinal vessel attenuation and corresponding (F) UWF red-free image showing a granular hypoautofluorescence throughout the retina with an abnormal area of subtle macular hyperautofluorescence.
Patient-reported descriptors of CBS characteristics were available for 11 of 13 and are shown in table 2. Twelve patients described simple hallucinations, two reported both simple and complex and one experienced hallucinations of a complex nature only. It remains unclear whether underlying diagnosis can be used as a predictor for susceptibility to either simple or complex hallucination type. Clinicians-in-training were the most common reporting healthcare professional, documenting six cases. Consultants reported three cases and optometrists in four. The most common management decision by clinical personnel was to provide information and reassurance (via information leaflet or verbally) about CBS, while in clinic in seven cases, three patients had no management documented in the patient records.
Description of CBS symptoms, clinical management decisions and patient-reported impact of hallucinations
DISCUSSION
We report the largest case series of 13 paediatric and young persons affected with CBS visiting a single centre between 2011 and 2020. The majority of patients were suffering with progressive severe sight impairment, mostly due to non-syndromic IRDs, which collectively are the most common cause of blind registrations in the working-age population in England and Wales.16 The most frequent underlying condition was STGD (OMIM #248 200), a macular dystrophy which is typically associated with loss of central vision within the first two decades of life. There is currently no approved treatment for STGD, although several trials are underway that hold promise of halting disease progression,17 18 but patients will still have residual sight loss depending on the stage of the disease when intervention becomes available. Similarly, no treatments exist for the other conditions observed in this review; therefore, patients’ vision will either remain stable or continue to deteriorate. It remains unclear if the small numbers of cases identified in this review are reflective of a lower prevalence of CBS in younger people compared to the elderly, or if these numbers are due to factors such as substantial under-reporting and difficult case ascertainment. We do not yet understand why certain individuals are affected with CBS, or in whom they will resolve with time or persist longterm.
The cohort of paediatric and adolescent patients susceptible to CBS is likely considerable in size.19 Yet, the extent to which CBS is age-dependent is open to debate.20 In previous research, older age has emerged as a risk factor for visual hallucinations, while other studies have identified younger patients more likely to report CBS.21 22 Explanations for these differences may relate to the interaction between age and deafferentation, or older patients’ decreased capability to recollect, or willingness to disclose hallucinations. Although our sample is too small to interrogate with statistical analysis, the results provide convincing evidence of the need for paediatric ophthalmologists, specialists in ocular genetics and clinical geneticists involved in the care pathways of patients with genetic eye disease or poor vision during childhood, to provide information on CBS at the point of contact. The visual hallucinations may not necessarily manifest in the initial stages of the disease but could trigger during the active sight loss phase. Hence, providing patients and families with information on CBS and hallucinatory experiences, including strategies for symptom management and sources of emotional support, may reduce the psychological impact if they do develop symptoms.
Clinical history of our patients indicated that the majority had recorded significantly reduced visual acuity in at least one eye at the time of CBS onset. This is consistent with the theory that neurophysiological mechanisms, namely deafferentation, could be responsible for the disinhibition of the visual cortex resulting in hallucinatory experiences.4 In this cohort, there was no clear correlation between visual dysfunction and CBS, with some patients displaying loss of central vision, others with near-normal central vision but extensive peripheral visual field loss and others with a normal healthy eye but vision loss in the contralateral eye. This suggests that BCVA alone is unlikely to be a sufficient predictor for CBS onset, and thus, we suggest there should be no visual acuity or functionality threshold before physicians advise or enquire about CBS symptoms.
Limited descriptions of simple hallucinations were available, with records primarily referring to onset of ‘positive visual phenomena’. This broad term is used to describe an array of visual disturbances, typically non-formed stimuli such as phosphenes (rings and spots), photopsias (small blinking flashes of light that are often continuous but tend to decrease as scotomas become denser) and palinopsia (persistence or reappearance after cessation of stimulus). A number of these visual disturbances, especially photopsia, are experienced in patients with progressive IRDs; one study reported as much as 93% of patients with retinitis pigmentosa experiencing light flashes.23 These manifestations are thought to be due to the spontaneous activity of degenerating retinal cells or remodelling in the inner plexiform layer following photoreceptor cell death. It is important to distinguish this from CBS, but it is unlikely that even these symptoms are discussed with patients from our findings.
Complex hallucinations are those containing discrete, life-like scenes or images such as people and animals. Both simple and complex hallucinations were found to be disruptive to patients’ daily lives. For example, persistence of hallucinations contributed to withdrawal from higher education for one patient. Although numbers were low, complex hallucinations appeared to be more problematic than simple hallucinations, causing fear, anxiety, disrupted sleep, reduced appetite and food aversion. Notably, all reports of complex hallucinations in this study (n=3) came from patients with IRDs, posing an increased risk of disturbing hallucinations among this patient cohort. Of further note, just one patient explicitly described symptoms as not upsetting or disruptive, while over half the reports did not include detail on the extent to which CBS impacted lifestyle and well-being. Further research on the psychological impact of CBS in paediatric and adolescent patients is warranted. Literature relating to psychological well-being in adults with CBS purports that patients do not always feel distressed or threatened by their hallucinations,7 likely due to most individuals being aware of the unreal nature of the images they see. However, data from clinical case reports indicated that two out of three children (all under 8 years) believed their hallucinations to be real.9 This finding indicates that children may be more susceptible to maladaptive responses to hallucinations, such as fear and distress; we propose this is investigated in future studies.
This case series raises important questions regarding the nature of visual hallucinations experienced in CBS. Certainly, patients describing complex hallucinations in this study would satisfy criteria for severe sight impairment registration in the United Kingdom (ie, Snellen visual acuity <3/60 with a full visual field or 6/60 with severe visual field loss). This finding is consistent with a previous inference of a correlation between reduced vision and prevalence of more complex and overwhelming hallucinations.24 Evidence from research using functional MRI suggests that hallucinatory content is correlated with the area of localised neural activity, for example, complex hallucinations such as faces have been linked to activity in the left middle fusiform gyrus.25 Further investigation to establish causal factors for onset of complex hallucinations is necessary.
Clinical management of CBS, once suspected or diagnosed, including strategies to promote effective psychological coping was variable. Clinicians often attempted to provide reassurance in clinic and guided patients to family support services and/or support group campaigns, such as Esme’s Umbrella (www.charlesbonnetsyndrome.uk). Prescription of an antipsychotic agent was observed in one case; however, no data on effectiveness was available for analysis. Melatonin was prescribed in one case to help regulate sleep that had been disturbed by hallucinations. Yet, for most patients, information on clinical management of CBS was not systematically captured within patient records. Moreover, reporting of efficacy or outcome of chosen management strategies at follow-up was scarce. Efforts are currently underway to establish optimal treatment pathways for patients with visual hallucinations, including carer support, counselling and cognitive–behavioural therapy.26 In this review, referral to counselling services or family support did not appear to be based on individual factors such as level of visual acuity, nature of hallucinations or impact of CBS on well-being. We propose that use of a purpose-made CBS pro-forma with an information leaflet could be useful in improving the quality of care provided to patients. In addition, it would improve history-taking and symptom documentation, advice on coping mechanisms and further referral to psychiatry in severe refractory cases.
We recognise some limitations to our study. First, not all paediatric and young adults with CBS may have been identified from the selected search terms if clinicians had not made reference to the condition in the electronic patient records (but only in the hard copy medical notes). Yet, the aim of this review was to describe the profile of these patients using as much appropriate data as possible, rather than determining expected numbers. This was a retrospective review and therefore no estimation of power could be provided; however, our study methods are similar to those of other published reports.27 The authors are in the process of conducting a prospective national epidemiology study to ascertain prevalence and management of CBS in children throughout the United Kingdom. Nonetheless, this series remains useful in providing information on CBS patient profile, overall management behaviour of physicians and insight into the psychological burden and everyday challenges faced by young persons with CBS.
Despite the distressing nature of CBS, visual hallucinations are seldom addressed during routine clinical assessments. Patients rarely volunteer information about hallucinations due to fears of being diagnosed with a psychiatric condition.28 29 As such, tactful inquiry as to the presence of visual hallucinations is an important component of the clinical consultation in at-risk patient groups. This is arguably a shortcoming of current paediatric ophthalmology services as there are a number of simple and effective ‘brain shunting’ exercises which may help reduce CBS symptoms.30 Strategies include frequent blinking or rapid eye movements, attempting to touch or brush away hallucinations, moving to brightly lit areas and increasing social interactions, which help counter inactivity.
This study raises awareness of the incidence of CBS in children and adolescents with sight loss. Patients may present to a range of clinical and allied healthcare professionals; hence, education is required for all those interacting with patients in high-risk groups within the hospital eye service and beyond, including the primary care setting and social services. Although factors relating to the aetiology of child and adolescent CBS are yet to be fully understood, the distinct clinical features we report may help to anticipate psychological outcomes and allow for better targeting of patient support. Moreover, our findings could be used to initiate improvements in healthcare delivery to this potentially high caseload of patients by profiling those who may be at risk of developing CBS, and we highlight the current unmet need for improved documentation of symptoms and intervention outcome. We provide these clinical characteristics in the hope that ophthalmologists, paediatricians and all those working with children experiencing progressive or severe sight loss are encouraged to ask and inform patients about visual hallucinations.
REFERENCES
Footnotes
Twitter Mariya Moosajee @MariyaMoosajee.
Contributors LJ obtained and examined medical records and contributed to the analysis, discussion and main interpretation of results and writing of the article. MM devised the study, examined medical records and image interpretation and contributed to the analysis, discussion and main interpretation of results and writing of the article.
Funding This study was funded by Thomas Pocklington Trust and Wellcome Trust (205174/Z/16/Z).
Competing interests The authors declare no conflict of interest.
Ethics approval The study was approved by London—Camden & Kings Cross Research Ethics Committee (12/LO/0141).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.
Linked Articles
- At a glance