Article Text

Abstract
Aim To identify retinal findings using dilated eye examination, which are possibly related to SARS-CoV-2 infection in hospitalised patients with confirmed severe COVID-19.
Methods In this cross-sectional study, hospitalised patients with confirmed severe COVID-19 in a single referral centre for the treatment of COVID-19, in Santo André, São Paulo Metropolitan Area, Brazil, underwent dilated eye examination of both eyes performed by a retina specialist. Findings were recorded using a portable digital fundus camera. Retinographies were analysed by two retina specialists. Medical records were reviewed for assessment of patient demographics, baseline comorbidities and clinical data.
Results There were a total of 18 patients, nine (50%) male, median IQR age of 62.5 (12) years. Ten of the 18 patients (55.6%; 95% CI 33.7 to 75.4) had abnormalities on dilated eye examination. The main findings were flame-shaped haemorrhages (N=4; 22.2%; 95% CI 9.0 to 45.2) and ischaemic pattern lesions (cotton wool spots and retinal sectorial pallor) (N=4; 22.2%; 95% CI 9.0 to 45.2), with one patient having both cotton wool spots and flame-shaped haemorrhages.
Conclusion These findings suggest that patients with severe COVID-19 have acute vascular lesions of the inner retina including flame-shaped haemorrhages and cotton wool spots. Further studies controlling for confounding factors are necessary to properly assess these findings so as to increase the understanding of COVID-19 pathophysiology and to identify new therapies.
- Retina
- Infection
- Imaging
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the COVID-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
INTRODUCTION
COVID-19, caused by the SARS-CoV-2, emerged from Wuhan, China, in December 2019 and has become a global health threat, being declared a pandemic by the WHO on 11 March 2020.
Although patients with COVID-19 usually present with fever and respiratory tract symptoms, it has been shown that COVID-19 can affect other organ systems, manifesting as cardiovascular, neurological, gustatory, gastrointestinal, hepatic, renal, olfactory, haematological, cutaneous and ocular symptoms.1
The ocular manifestations of SARS-CoV-2 infection are not completely understood; most studies have reported ocular surface disorders.2–4 Marinho et al posed the hypothesis of retinal involvement by SARS-CoV-2 and reported hyper-reflective lesions on optical coherence tomography at the level of ganglion cell and inner plexiform layers of 12 patients diagnosed with COVID-19 and mild-to-moderate symptoms.5 An autopsy study also identified viral RNA of SARS-CoV-2 in retinas of deceased patients with COVID-19.6 The pro-thrombotic status reported in critically ill patients with COVID-19 may also lead to retinal injuries in addition to retinal damage by the direct activity of SARS-CoV-2.7 8
The objective of this study was to identify retinal findings using dilated eye examinations, which are possibly related to SARS-CoV-2 infection in hospitalised patients with confirmed severe COVID-19.
MATERIALS AND METHODS
Design
This single-centre cross-sectional study was performed from 20 to 23 May 2020 with inpatients at Mário Covas State Hospital, Santo André, São Paulo Metropolitan Area, Brazil, a referral centre for the treatment of patients with COVID-19. The present study was approved by the institutional research ethics committee of the Faculdade de Medicina do ABC under protocol 4.067.204 and was carried out in accordance with the relevant guidelines and tenets of the Declaration of Helsinki. Written informed consent was obtained from patients or next of kin, consistent with Brazilian’s National Research Ethics Committee resolution for research conducted during the COVID-19 pandemic.
Participants
We included patients who consented or whose next of kin consented to participate in the study and who had a confirmed diagnosis of severe COVID-19 according to the Brazilian Epidemiological Monitoring Guidelines for the Public Health Emergency of COVID-19 published by Brazilian Ministry of Health on 3 April 2020.9 Exclusion criteria were concurrent endocarditis, other viral infections including HIV, and terminal cancer.
Dilated eye examination and retinography
Dilated eye examinations of both eyes were performed by a retina specialist using a binocular indirect ophthalmoscope and a handheld condensing a 20 D lens after 30 min of instillation of tropicamide (1%). Any macular or peripheral retinal findings were recorded using a Volk Pictor Plus (Volk Optical, Mentor, OH, USA) digital fundus camera (field of view 40°). Retinographies were then analysed by two additional retina specialists, and findings were described by each of them individually. Divergent opinions were reconciled by consensus among the three retina specialists.
Clinical data
Medical records were reviewed and the following data were analysed: general characteristics, baseline comorbidities, presence of ocular symptoms, date of confirmatory examination (reverse transcriptase-PCR (RT-PCR) from nasopharyngeal swabs for SARS-CoV-2), admittance to intensive care unit (ICU), necessity for invasive mechanical ventilation, necessity for vasoactive pharmacological support and use of anticoagulation therapy.
Statistical analyses
Results were expressed as medians and IQR for continuous variables. Categorical variables were expressed as proportions with 95% CIs that were computed using the Wilson-Brown hybrid method. These analyses were performed using GraphPad Prism (GraphPad, version 8.0, San Diego, CA, USA).
RESULTS
Sample description
A total of 18 patients were included in the study, nine (50%) male with median IQR age of 62.5 (12) years. Of these, 17 (94.4%) patients were admitted to the ICU at some point during the hospital stay, 13 (77.8%) needed invasive mechanical ventilation and 7 (44.4%) needed vasoactive pharmacological support. Twelve (66.7%) patients had a previous diagnosis of high blood pressure (HBP) and nine (50%) had diabetes mellitus (DM). No patient had ocular symptoms on medical records (table 1).
Clinical characteristics of patients with severe COVID-19 who underwent dilated eye examinations
Retinal findings
The median time (IQR) between confirmatory examination of COVID-19 (RT-PCR for SARS-CoV-2) and dilated eye examination was 11.5 (8) days. Ten of the 18 patients (55.6%; 95% CI 33.7 to 75.4) had abnormalities on dilated eye examination (table 2A and B). The main findings were flame-shaped haemorrhages (N=4; 22.2%, 95% CI 9 to 45.2) and cotton wool spots (N=3; 16.7%; 95% CI 5.8 to 39.2), with one patient having both cotton wool spots and flame-shaped haemorrhage (figure 1). One patient had retinal sectorial pallor suggestive of acute retinal ischaemia (5.6%; 95% CI 0.3 to 25.8). Other findings included peripheral retinal haemorrhages (N=2; 11.1%; 95% CI 2.0 to 32.8), retinal pigment epithelium hyperplasia (N=1; 5.6%; 95% CI 0.3 to 25.8), choroidal naevus (N=1; 5.6%; 95% CI 0.3 to 25.8) and macular haemorrhages and hard exudates (N=1; 5.6%; 95% CI 0.3 to 25.8).
Retinal findings on dilated eye examination of inpatients with severe COVID-19
{kind=link}
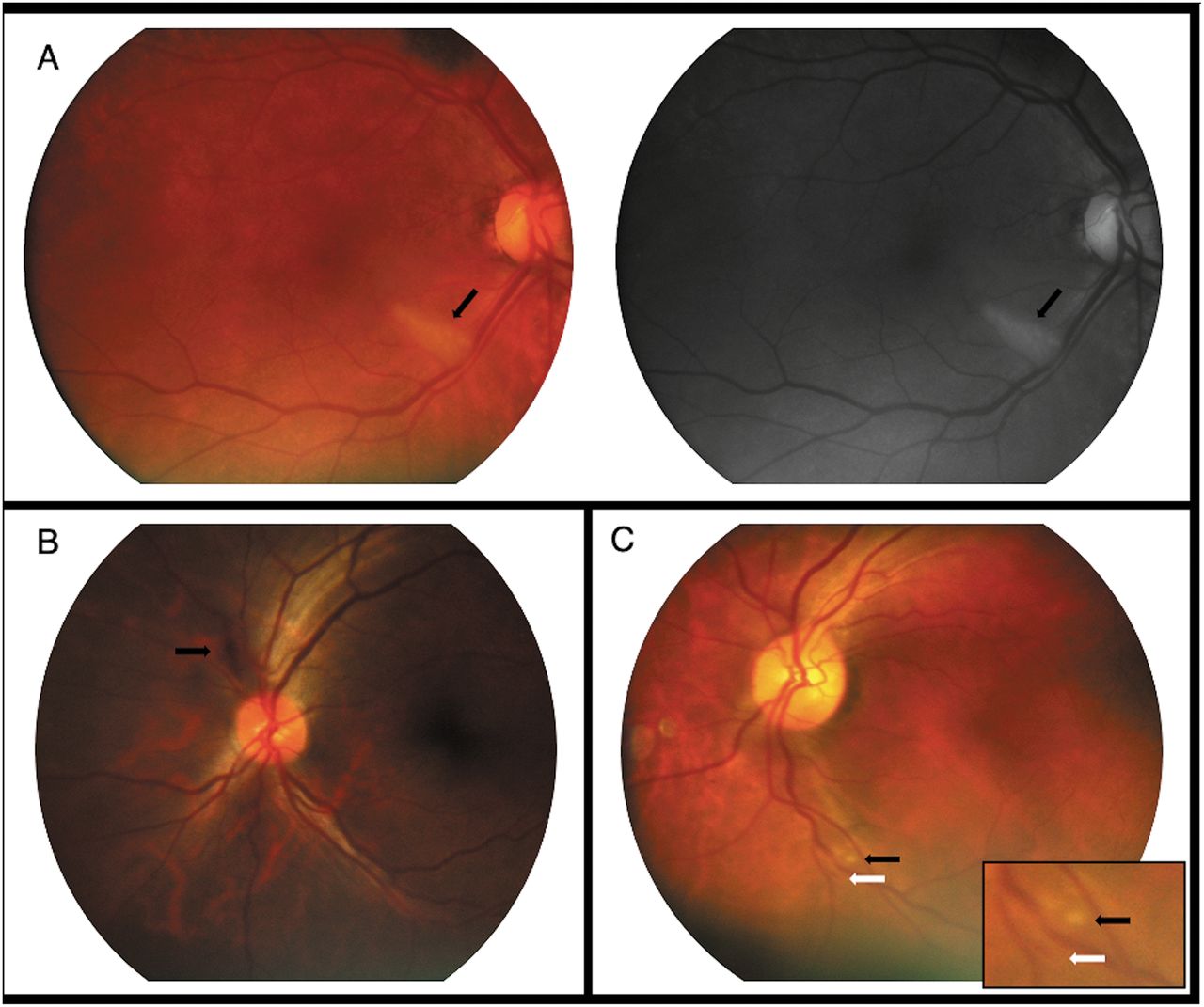
Main retinal findings of patients with severe COVID-19. Panels (A–C) represent three different patients with no baseline comorbidities. (A) Colour fundus photography and red-free imaging of the right eye of a female patient in her 60s revealing well-delimited sectorial pallor at the lower temporal arcade (black arrow). Vasoactive pharmacological support was not necessary during hospitalisation. (B) Colour fundus photography of the left eye of a male patient in his 40s revealing a peripapillary flame-shaped haemorrhage (black arrow). Vasoactive pharmacological support was necessary during hospitalisation. (C) Colour fundus photography of the left eye of a female patient in her 60s revealing a cotton wool spot (black arrow) and adjacent flame-shaped haemorrhage (white arrow) at the lower temporal arcade. Vasoactive pharmacological support was not necessary during hospitalisation.
DISCUSSION
To the best of our knowledge, this is the first report of retinal findings in hospitalised patients with severe COVID-19. Our study was designed to evaluate possible retinal involvement by SARS-CoV-2 because of the hypothesis generated regarding patients with mild-to-moderate COVID-19.5 The SARS-CoV-2 belongs to the group of coronaviruses that are known to cause ocular infections in various animal species.10
We found that 10 of the 18 patients had abnormalities on dilated eye examination, not necessarily related to SARS-CoV-2 infection, because chronic alterations like retinal pigment epithelium hypertrophy and choroidal naevus were observed. However, inner retinal vasculature acute lesions such as flame-shaped haemorrhages and cotton wool spots were the main findings, and one patient had retinal sectorial pallor suggestive of recent retina ischaemia. In some cases, these lesions appeared in the absence of vasoactive pharmacological support, DM, or systemic HBP, suggesting that they might be related to COVID-19 itself.
The retina could be affected either by direct tissue damage by SARS-CoV-2 and its immunogenicity11 or by the thrombotic complications that have been reported to have a remarkably high incidence in patients with COVID-19 admitted to the ICU.7
Direct infection and immune injury are thought to be involved in nerve damage in COVID-19.11 The inner retina is a neuronal tissue, and may also be injured by SARS-CoV-2 as has been reported for the central nervous system.12 SARS-CoV-2 RNA has already been identified in retinas of deceased patients with COVID-19,6 and other viruses are known to cause similar retinal injuries. These include HIV, dengue virus and Zika virus.13 14
It has been reported that critically ill patients with COVID-19 in the ICU have thrombotic complications at rates as high as 31%.7 Although more information is needed, the coagulopathy appears to be related to the profound inflammatory response against the SARS-CoV-2 and not to intrinsic viral activity.8 This is because the retina is one of the most metabolically active tissues in the body and its terminal circulation is particularly sensible to ischaemic events.15 We found cotton wool spots, which are thought to result from occlusion of terminal retinal arterioles in the nerve fibres and ganglion cell layer, with consequent retina ischaemia and infarction, and retinal sectorial pallor, possibly caused by branch arterial occlusion secondary to thromboembolic phenomena.14
This study had several limitations. First, there was relatively small sample size. Second, there were potential confounding factors such as baseline comorbidities and therapeutic approaches. HBP and DM are known to cause retinal lesions similar to the ones we found. Because of their high prevalence among elderly and because they are risk factors for severe presentations of COVID-19, excluding patients with HBP and DM would make the study unfeasible. Furthermore, vasoactive pharmacological support could also be a confounding factor because acute peaks of blood pressure could also cause similar lesions. Third, the ophthalmological evaluation was limited to dilated eye examination. Complementary exams such as optic coherence tomography would provide a deeper understanding of our findings; however, this was impracticable because of the patients’ clinical statuses and contact precautions. Patients will be followed up as their clinical status and contact precautions allow for multimodal retinal imaging and further investigation.
Our results suggest that the retina might be affected in patients with COVID-19. However, given the clinical characteristics of the disease, confounding factors are difficult to control. Further studies with larger samples are necessary to assess this possibility. Nevertheless, we are sharing these preliminary results in an effort to inform the scientific community about the possibility of retina lesions in patients with severe COVID-19.
Footnotes
Contributors All authors have given final approval of this version to be published. LAP, LCMS, JZA-N designed the study; LAP, LCMS, PAN, LRNC, VLL conducted the study; LAP, LCMS, PAN, HTS, JZA-N, VLL, GLV managed the data; PAN, HTS, JZA-N, GLV, FLAF, VLL interpreted the data; LAP and JZA-N prepared the manuscript; and JZA-N, VLL, FLAF did overall coordination.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The institutional research ethics committee of Faculdade de Medicina do ABC under protocol 4.067.204.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available from the corresponding author upon reasonable request.
Linked Articles
- At a glance