Article Text

Abstract
Aims To determine the correspondence between GNAQ R183Q (c.548G>A) mutation in abnormal scleral tissue of patients with Sturge-Weber syndrome (SWS) secondary glaucoma and explore the role of GNAQ R183Q in glaucoma pathogenesis.
Methods Episcleral tissues were obtained from 8 patients: SWS secondary glaucoma (n=5) and primary congenital glaucoma (PCG, n=3). Scleral tissues were obtained from 7 patients: SWS secondary glaucoma (n=2), PCG (n=1) and juvenile open-angle glaucoma (n=4). GNAQ R183Q mutation was detected in scleral tissue by droplet digital PCR. Tissue sections from SWS were examined by immunohistochemistry to determine the expression of p-ERK.
Results The GNAQ R183Q mutation was present in 100% of the SWS abnormal sclera. Five cases were SWS patient-derived episcleral tissue, and the mutant allelic frequencies range from 6.9% to 12.5%. The other two were deep scleral tissues and the mutant frequencies were 1.5% and 5.3%. No mutations in GNAQ R183 codon were found in the sclera of PCG and juvenile open-angle glaucoma. Increased expression of p-ERK and p-JNK was detected in the endothelial cells of SWS abnormal scleral blood vessels.
Conclusions GNAQ R183Q occurred in all abnormal scleral tissue of SWS secondary glaucoma. Increased expression of p-ERK and p-JNK in endothelial cells of blood vessels was detected in the abnormal scleral tissue. This study suggests GNAQ R183Q may regulate episcleral vessels of patients with SWS through abnormal activation of ERK and JNK, providing new genetic evidence of pathogenesis of glaucoma in SWS, and the dysplasia of scleral tissue in anterior segment may be used as an early diagnostic method or treatment targets to prevent the development and progression of glaucoma in patients with SWS.
- glaucoma
- sclera and episclera
- not applicable
Data availability statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sturge-Weber syndrome (SWS) was first reported by Sturge in 1879.1 The prevalence is almost 1:50 000 and it was shown previously that no gender orientation exists in SWS.2 SWS is a neurocutaneous disorder that is characterised by a port-wine stain (PWS) that affects the skin in the distribution of the ophthalmic branch of the trigeminal nerve.3 PWS presents in 0.3% live births.4 Besides facial port-wine stain, PWS is located on the neck, trunk and extremities at much less frequencies.5 Vascular malformation was also found in the leptomeninges of the brain and choroid.3 6 In addition, manifestations included neuro-ocular symptoms such as glaucoma, seizures, developmental delay and cognitive impairments.7 The diagnosis of SWS is based on the presence of PWS, leptomeningeal angioma and glaucoma. However, not all patients display all three characteristics. Glaucoma exists in 30%~71% of patients with SWS.8–13
There were many hypotheses for SWS pathogenesis until Shirley and colleagues6 found that a GNAQ R183Q (c.548G>A) somatic mutation affected 88% and 92% tissue of patients with SWS and PWS (non-syndromic port-wine stains), respectively. GNAQ encodes the α subunit of heterotrimeric guanine nucleotide-binding protein (G protein). When ligands bind to G protein-coupled receptors (GPCRs), GPCRs undergo conformational changes and bind to G protein heterotrimers Gαβγ in the cytoplasm, catalysing the conversion of GDP from GNAQ to GTP. GTP-bind-α then dissociates from Gβγ and thereby activates downstream signalling pathways. Under normal conditions, Gα can transform to an inactive GDP-bound state through intrinsic GTPase activity. It was surmised that GNAQ R183Q (c.548G>A) mutation decreases autohydrolysis of GTP to GDP, giving rise to chronic hyperactivation of GNAQ activity. The well-known downstream signalling involves PLC-β-induced hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2), which leads to the activation of PKC and subsequent MAPK.14 15 Increased endothelial p-ERK expression has been reported in PWS and the endothelial cells of leptomeningeal vessels.16 17
SWS secondary glaucoma show a bimodal distribution of the age of onset, which suggests separate aetiologies for early-onset and late-onset glaucoma in SWS. Early-onset glaucoma has been suggested to result from anterior chamber angle anomalies,18 while juvenile-onset or adulthood-onset glaucoma is believed to be due to elevated episcleral venous pressure (EVP).19 Weiss suggested that arteriovenous shunts within episcleral hemangiomas increase pressure in the veins that drain Schlemm’s canal. In turn, the high EVP elevates intraocular pressure (IOP).20 Consistent with Phelps’ findings, our previous results suggested that scleral vascular malformations exhibit a 100% co-occurrence in the patients with SWS secondary glaucoma.21 Furthermore, we also found that patients with SWS with early-onset glaucoma had different distribution patterns of episcleral hemangiomas, and the trabeculotomy had a poorer prognosis in the patients with more excessive vascular malformations.21 Hence, we believed that vascular factors may play a pivotal role in the pathogenesis of SWS early-onset glaucoma. However, the initial factors that contributed to scleral vascular malformations in SWS secondary glaucoma remained unknown. According to the previous report, GNAQ somatic mutations may be involved with the vascular malformations in the skin and leptomeninges. Therefore, we explored whether there were GNAQ somatic mutations in the episcleral vessels of patients with SWS.
Methods
Patients
All experiments were carried out in accordance with the institutional guidelines. Written informed consent was obtained from patients or legal guardian of paediatric patients. The total number of enrolled patients clinically diagnosed with SWS, PCG and juvenile open-angle glaucoma (JOAG) was 7, 4 and 4, respectively.
The diagnosis, surgery, tissue collection and follow-up were all provided by the same ophthalmologist (WG).
Scleral biopsy
To minimise the potential impact on surgery outcome, a total of 15 scleral tissues were collected during the procedure of non-filtering anti-glaucoma surgeries including trabeculotomy or NPGS (non-penetrating glaucoma surgery). The collected episcleral tissues with attached episcleral vessels were approximately one-fifth of the total scleral thickness and with the size of 1 mm × 1 mm. The biopsy samples are taken 2 mm away from the temporal incision of scleral flap and 3 mm away from the limbus. As the episclera biopsy was taken in the electrocoagulation area and far away from the scleral flap, we believed that the procedure of tissue biopsy is supposed to be safe and had limited influences on the prognosis of these non-filtering surgeries (figure 1). Deep scleral tissues with the size of 2 mm × 3 mm were acquired during the NPGS procedure, and they were composed of the outer wall of Schlemm’s canal, sclera and perforating vessels.

Episclera biopsy in patients with SWS. Patients with SWS had high-density blood vessel distribution on the scleral surface of the operative field (A). After obtaining the episclera biopsy and local electrocoagulation, the scleral area was basically normal, which did not affect the operation (B).
Droplet digital PCR (ddPCR) analysis for GNAQ p.R183Q
DNA extraction
Genomic DNA from scleral tissue was extracted via using Qiagen QIAamp DNA Micro Kit according to the manufacturer’s instruction.
DNA concentration was measured using the Qubit dsDNA BR assay kit (Termo Fisher Scientifc) according to the manufacturer’s instruction.
Droplet digital PCR
Primers and probes were designed to target GNAQ p.R183Q as described previously.22
Sequences used were:
Forward primer (GNAQ-R183Q-F: 5′-CCTGCCTACGCAACAAGAT-3′);
Reverse primer (GNAQ-R183Q-R, 5′-GTAAGTCAAAGGGGTATTCGAT-3′);
Reference(wide-type) probe (GNAQ-R183-WT, 5′-TGCTTAGAGTTCGAGTCCCCACC-3′);
Mutant probe (GNAQ-R183-MUT, 5′-TGCTTAGAGTTCAAGTCCCCACC-3′).
Briefly, the ddPCR reaction mixture was composed of 10 µL 2× ddPCR TM Supermix for Probes (no dUTP; Bio-Rad), 900 nM forward primer, 900 nM reverse primer, 450 nM probe and 2 µL of DNA sample to a final volume of 20 µL. Then 20 µL of each reaction mixture was loaded into the sample well of an eight-channel droplet generator cartridge (Bio-Rad), and droplets were generated with 70 µL of droplet generation oil (Bio-Rad) using the manual QX200 Droplet Generator. Following droplet generation, samples were manually transferred to a 96-well PCR plate, heat-sealed with foil bag (180℃, 5 s) and amplified on a Bio-Rad C100 thermal cycler using the following cycling conditions: 95°C for 10 min for one cycle, followed by 40 cycles at 94°C for 30 s and 60°C for 1 min, 1 cycle at 98°C for 10 min and 12°C for infinite. Post-PCR products were read on the QX200 droplet reader (Bio-Rad) and analysed using QuantaSoft software.
In order to rule out the potential false-positive events which might result from molecular biological noise in ddPCR. We calculated the limit of blank (LOB) value via unilateral Poisson distribution, and the false-positive drop caused by mismatch is less than 0.01% as the criterion for the LOB value. According to the calculation results, we defined that seven or more positive droplets in the FAM channel were determined as the positive sample interpretation threshold.
Immunohistochemistry
Immunohistochemistry was performed using routine procedures as previously described.16 Briefly, deparaffinised and rehydrated sections were subjected to microwave treatment in 10 mM sodium citrate buffer, pH 6.0 for antigen retrieval. The sections were incubated in a humidified chamber with the following primary antibodies: p-ERK (Santa Cruz Biotechnology (California, USA), sc-7383, monoclonal, mouse, 1:200, overnight incubation at 4°C) and p-JNK (Santa Cruz Biotechnology (California, USA), sc-6254, monoclonal, mouse, 1:200, overnight incubation at 4°C). The positive cells were histochemically detected with the DAB method.
Statistical analyses
Statistical analyses were performed with SPSS V.6. Mutation rates of scleral tissues of patients with SWS, JOAG and PCG were compared using one-way ANOVA.
Results
In the present study, we enrolled seven patients with SWS and eight childhood glaucoma controls (four patients with PCG and four with JOAG). The subjects included in this study had significant differences in the distribution characteristics of episcleral blood vessels. All seven patients with SWS had high-density blood vessel distribution on the sclera surface of the operative field (figure 2A) while PCG (figure 2B) and JOAG (figure 2C) showed normal scleral vein morphology.

Differences between Sturge-Weber syndrome (SWS) to primary congenital glaucoma (PCG) and juvenile open-angle glaucoma (JOAG) patients’ distribution characteristics of episcleral blood vessels. Patients with SWS had high-density blood vessel distribution on the scleral surface of the operative field (A). Patients with PCG (B) and JOAG (C) showed normal scleral vein morphology.
The GNAQ R183Q mutation was quantified by ddPCR in DNA of 15 scleral samples from patients with or without SWS (JOAG and PCG) (figures 3 and 4). Demographics and basic features are shown in table 1. In the current study, the GNAQ R183Q mutation was present in 100% (seven out of seven) of the SWS abnormal scleral tissue. Meanwhile, no mutation of GNAQ R183Q was detected among these scleral tissues of patients with PCG and JOAG (figure 5, table 2). Currently, different scleral tissues from distinct regions (episclera and deep sclera) were collected for ddPCR testing for the diverse role they played in the procedure of aqueous humor drainage. Five of the seven cases were SWS patient-derived episcleral tissue, which contained abnormal vascular tissue, and the mutant allelic frequencies range from 6.9% to 12.5%. The other two cases were deep scleral tissue, which were considered to contain the outer wall of Schlemm’s canal and the penetrating branches of aqueous venous, and the mutant frequencies were 1.5% and 5.3%. In the process of anti-glaucoma surgery, we observed the mixture of aqueous humor and blood which indicated the superficial scleral tissue may be involved directly in the outflow of aqueous humor. In addition, the deep scleral tissue obtained during NPGS composed of the outer wall of Schlemm’s canal, sclera and perforating vessels which can physically affect the drainage system aqueous humor. These results suggest GNAQ R183Q mutation may run through the whole aqueous outflow pathway, including Schlemm’s canal and aqueous veins, which might directly cause glaucoma.
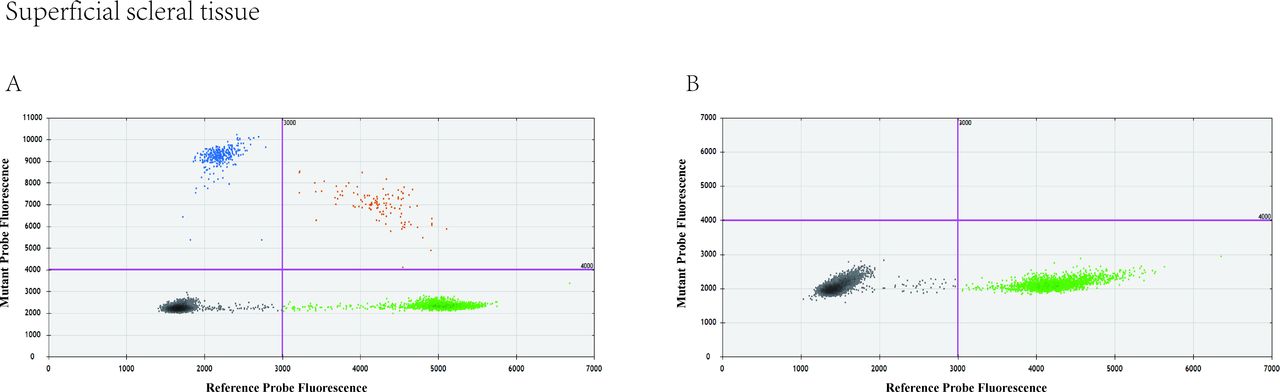
GNAQ R183Q allelic frequency in the patient-derived superficial scleral tissue. Representative droplet digital PCR (ddPCR) results of patient-derived superficial scleral tissue in patients with Sturge-Weber syndrome (A) and patients with primary congenital glaucoma (B). The dot plots show the droplet fluorescence for the wild-type allele (x-axis) and GNAQ R183Q allele (y-axis).
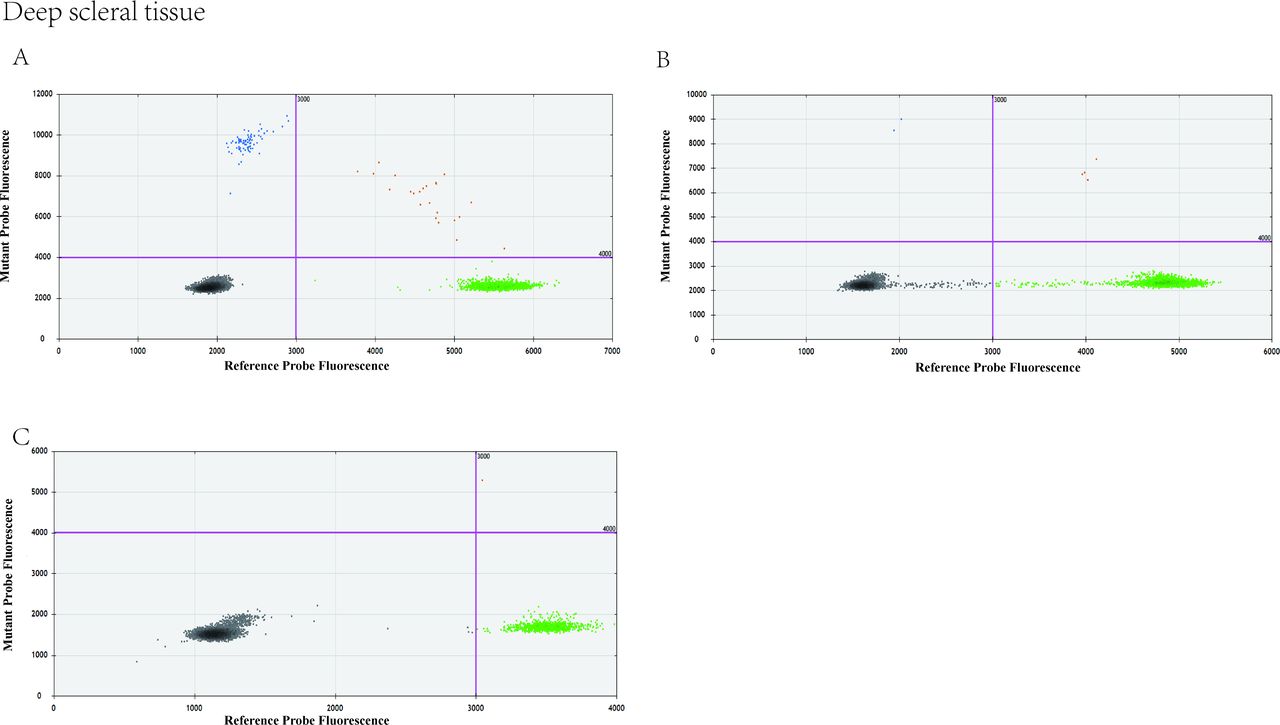
GNAQ R183Q allelic frequency in the patient-derived deep scleral tissue. Representative droplet digital PCR (ddPCR) results of patient-derived deep scleral tissue in patients with Sturge-Weber syndrome (A), primary congenital glaucoma (B) and juvenile open-angle glaucoma (C). The dot plots show the droplet fluorescence for the wild-type allele (x-axis) and GNAQ R183Q allele (y-axis).

Mutation rate of scleral tissues of Sturge-Weber syndrome (SWS), juvenile open-angle glaucoma (JOAG) and primary congenital glaucoma (PCG). The mutation rate is significantly elevated in the scleral tissues of patients with SWS when compared with the scleral tissues of patients with JOAG and those with PCG. **p<0.01.
Demographics and basic features of patients with glaucoma
Mutant clone ratios detected by ddPCR
Beyond the data of ddPCR, we also used immunochemistry technique to further validate the expression of p-JNK and p-ERK in scleral tissues, which are the activated downstream pathways of GNAQ. Expression of p-ERK was detected in episcleral vessels of SWS (figure 6A), congenital glaucoma (figure 6B) and the cadaver eye without glaucoma (figure 6C) and increased activation of p-ERK was found in patients with SWS. P-JNK can also be observed in the endothelial cells of scleral tissues in patients with SWS (figure 6D) but hardly any in that of the cadaver eye without glaucoma (figure 6E). Combined with the activation of ERK in PWS and leptomeningeal angioma taken from patients with SWS, we believe that MAPK pathway may play a role in the pathogenesis of ocular lesion.16 17 These results suggested that GNAQ R183Q mutation is specifically expressed in the endothelial cells of scleral vessels in the ocular lesions of patients with SWS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Activation of extracellular signal-regulated kinase (ERK) and c-Jun N-terminal kinase (JNK) in superficial scleral tissue. Immunohistochemistry staining showed increased activation (red asterisk) of phosphate-ERK in superficial scleral tissue of Sturge-Weber syndrome (SWS) (A) and moderate activation (arrows) in SWS (A), congenital glaucoma (B) and the cadaver eye without glaucoma (C). Expression of phosphate-JNK in SWS (arrowhead) (D) and the cadaver eye without glaucoma (arrow) (E). Scale bar=50 µm.
Discussion
To the best of our knowledge, this is the first study that showed GNAQ mutation in the anterior segment of patients with SWS. Previous studies had found this mutation in choroidal hemangiomas in a case of a patient with SWS23 24; however, choroidal hemangioma did not exist in all patients with SWS,10 and there were limited evidence that showed choroidal hemangioma occurrence related to the pathogenesis of glaucoma. Our earlier studies found that all SWS scleral surface had scleral vascular malformation.21 In some episcleral vascular malformations, the flow of blood–aqueous humor mixture could be seen,21 which showed that the presence of abnormal episcleral vascular network was also a part of the aqueous humor drainage pathway. In this study, both episcleral tissue (including malformed blood vessels) and deep scleral tissue (outer wall of Schlemm’s canal and aqueous venous penetration branch) had GNAQ R183Q mutations, suggesting that the mutation involved in the pathogenesis of SWS glaucoma. Additional specimens with appropriate methods of single-cell isolation and sequencing are needed to determine the identity of the mutant cells in this population.
In the present study, we enrolled seven patients with SWS and eight childhood glaucoma controls (four patients with PCG and four with JOAG) for detection of GNAQ R183Q mutation in the scleral tissue. The reasons for choosing PCG and JOAG as the control group were as follows: (1) the age of onset of these two diseases were similar to SWS; (2) most of these two diseases required surgical treatment, and we could obtain scleral tissue during the operation after the approval of the ethics committee.
Since its discovery, GNAQ R183Q mutation was confirmed in many SWS lesions. The mutant allelic frequencies were 1%~11.15%,25 26 1%~12.37%26 27 and 21%23 in leptomeningeal angiomatosis (LA), port-wine stain (PWS) and choroidal hemangioma of SWS, respectively. GNAQ R183Q mutant allelic frequencies reported in our study (SWS scleral tissue), generally 1.5%–12.5%, were similar to those in LA and PWS results while generally lower than that in choroidal hemangioma. This might be due to the mutation that was predominantly located within the blood vessels,27 or to be exact, in vascular endothelial cells (ECs).22 28 In ECs sorted from LA and PWS specimens, mutation frequencies of GNAQ R183Q were enriched to 24%~34.7%28 and 17.1%~42.9%. Thus, a relatively higher ddPCR result found in choroidal hemangioma is probably due to the abundant vascular structures of the choroid. To address this limitation, we would continue to collect specimens using the laser-capture microdissection method to identify the specific cell type with mutation and obtain more accurate mutation rate results in the abnormal scleral tissues of SWS secondary glaucoma.
Compared with the mutation rate range from 6.9% to 12.5% of episcleral tissue, GNAQ R183Q mutant allelic frequencies (1.5% and 5.3%) in deep scleral tissue is much lower. The episclera, which was vascularised, lies underneath the conjunctiva and Tenon’s capsule.29 There were avascular scleral stroma30 and a thin pigmented layer forming the sclera–choroid border.31 The only reason this tissue could still detect the GNAQ gene mutation is the outer wall of Schlemm’s canal and the penetrating branch of aqueous veins contained in it. Taken together, our present study might suggest that GNAQ mutation were present in the main pathways of aqueous humor outflow in patients with SWS secondary glaucoma, including Schlemm’s canal and aqueous veins, which might directly cause glaucoma.
SWS is characterised by vascular malformation. Although it is generally believed that GNAQ R183Q is the main aetiology factor, how this somatic mutation caused abnormal vascular phenotype remains unclear. Thus, the relationship between glaucoma and choroidal malformation remained unclear. Some studies have pointed out that compared with the natural Gαq model, the GNAQ R183Q mutation causes the loss of two hydrogen bonds between Gαq and GDP molecules, leading to the instability of Gαq inactivation.32 This constitutive activation may cause the continuous activation of downstream signalling pathways. Consistent with previous studies,16 17 we found increased expression of p-ERK and p-JNK in the endothelial cells of SWS abnormal scleral blood vessels. To our knowledge, this is the first study to confirm the activation of ERK and JNK in the eyes of patients with SWS. ERK and JNK are the most important components in the MAPK family.33 Shirley et al have proved the relationship between GNAQ(R183Q) mutation and elevated expression of p-ERK.26 It was worth noting that p-ERK had different degrees of activation in scleral blood vessels in patients with SWS. This may indicate the somatic mutation in episcleral vessels. One possible explanation is that endothelial cells (ECs) containing GNAQ mutation may have an overactivation of p-ERK while normal ECs only had a moderate activation of p-ERK. These results suggest the MAPK pathway may play a potential role in the SWS pathogenesis. Besides, disturbed activation of PI3K and increasing expression of VEGF and its receptors were also detected in SWS lesions.16 34 35 MAPK, PI3K and VEGF were all associated with angiogenesis.36–38 Taken together, GNAQ R183Q may contribute to vascular malformation of SWS through the combined effects of MAPK pathway, PI3K pathway as well as VEGF. Nevertheless, the connection between GNAQ mutation and downstream signals mentioned previously, and the interaction among those pathways require verification in further studies.
Recently, a case of choroidal hemangioma with SWS was reported GNAQ mutations in choroidal tissue in the ocular vascular system.23 24 However, there were only 20%–70% patients with SWS who suffered from choroidal hemangiomas.39 Thus, limited evidence showed a significant relationship between glaucoma and choroid malformation in patients with SWS. The somatic substitutions in GNAQ encoding R183Q was also found in patients with uveal melanoma, although Q209L was more common and showed stronger activation of MAPK signalling pathway.6 It was reported that the combination of MEK inhibitor (GSK1120212) and PI3K inhibitor (GSK2126458) induced cell apoptosis in a GNAQ/11-mutant-dependent manner.40 Besides, MEK inhibitor selumetinib combined with the AKT inhibitor MK2206 led to decreased cell viability in GNAQ-mutant uveal melanoma.41 Moreover, dual inhibition of PKC and MEK even caused significant tumour regression in a uveal melanoma xenograft model.42 For our findings of the GNAQ R183Q mutation and abnormally elevated MAPK signalling pathway (p-ERK and p-JNK) in scleral vascular malformation with SWS, these studies about therapeutic approach for the treatment of GNAQ-mutant diseases suggest that local application of MAPK signal pathway inhibitors may be promising treatments for alleviating dysplastic blood vessels in scleral tissue and suppressing the progression of scleral hemangiomas and in turn preventing SWS secondary glaucoma.
Conclusion
GNAQ R183Q (c.548G>A) occurred in all abnormal scleral tissue rich in dysplastic blood vessels which co-occur 100% with glaucoma in patients with SWS. Abnormally elevated MAPK signalling pathway (p-ERK and p-JNK) in endothelial cells of blood vessels was detected in the abnormal scleral tissue. This study suggests that GNAQ R183Q may regulate dysfunction of aqueous pathway of patients with SWS through abnormal activation of MAPK signalling pathways, providing new genetic evidence of pathogenesis of glaucoma in SWS, and the dysplasia of scleral tissue in anterior segment may be used as an early diagnostic method or treatment targets to prevent the development and progression of glaucoma in patients with SWS.
Data availability statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board of Ninth People’s Hospital Affiliated with the Shanghai Jiao Tong University School of Medicine (approval number: 2017-315 T235).
References
Footnotes
YW, CP and LH contributed equally.
HS and WG contributed equally.
Correction notice This article has been updated since it was first published. The funding number for the Clinical Research Program of 9th People's Hospital affiliated to Shanghai Jiao Tong University School fo Medicine has been corrected.
Contributors YW, CP and LH were involved in the concept, design, acquisition, analysis, interpretation of data and in the drafting of the manuscript. LX, XD, YL and CZ were involved in technical support, acquisition and analysis of data. HS and WG had full access to all the data in the study, took responsibility for the integrity of the data and the accuracy of the data analysis, and were involved in the revision of the manuscript and data files.
Funding This work was supported by the National Natural Science Foundation of China (81970796, 81670845), Clinical Research Program of Shanghai Municipal Health Commission (201940330), Clinical Research Program of 9th People's Hospital affiliated to Shanghai Jiao Tong University School of Medicine (JYLJ201904), the National Key R&D Program of China (2018YFC1106100, 2018YFC1106101) and the Research Grant of the Shanghai Science and Technology Committee (17DZ2260100).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance